New Technique for Iridodialysis Correction: Single-Knot Sewing-Machine Suture
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ocular Injury; Hazard to Society: a Case Series
Quest Journals Journal of Medical and Dental Science Research Volume 7~ Issue 8 (2020) pp: 34-44 ISSN(Online) : 2394-076X ISSN (Print):2394-0751 www.questjournals.org Research Paper Ocular Injury; Hazard to Society: A Case Series Dr Rashmi kujur1, Dr Pallavi. M.P2, Dr Harshita Dubey3, Dr Varsha4 1Dept. of ophthalmology, Madhav dispensary JAH, GRMC, Gwalior, Madhyapradesh. 2Senior girls hostel, GRMC, Gwalior, Madhyapradesh. 3Senior girls hostel, GRMC, Gwalior, Madhyapradesh. 4Senior girls hostel, GRMC, Gwalior,Madhyapradesh. Corresponding Author: Dr.Pallavi.M.P ABSTRACT Purpose: To describe various types of ocular trauma due to different modes of injuryoccured on the same day Design: Prospective interventional study (case series) Materials & Methods: A series of cases of ocular trauma in different age group on the same day. Results: Five patients of ocular trauma were studied & managed. All five patients were males. Out of 5 cases, 3 cases had open globe injury and 2 cases had closed globe injury. Three out of five patients required surgical intervention while 2 patients were managed with medical therapy. Conclusion: This study describes the types and characteristics of ocular trauma presenting in eye department. The frequency of ocular trauma is common in males. Eye injuries resulting from ocular trauma pose a frequent threat to vision the world over. While afocussed history and prompt ocular examination are essential to immediate management, patient educationregarding safety precautions and risk reduction help to prevent future recurrences. KEYWORDS: Ocular morbidity, Ocular Injury, globe rupture, iridodialysis, fire cracker injury, hyphema, Road Traffic accident (RTA), loss of vision. Received 05 December, 2020; Accepted 20 December, 2020 © The author(s) 2020. -

Traumatic Retinal Detachment Br J Ophthalmol: First Published As 10.1136/Bjo.75.1.18 on 1 January 1991
18 BritishJournalofOphthalmology, 1991,75, 18-21 Traumatic retinal detachment Br J Ophthalmol: first published as 10.1136/bjo.75.1.18 on 1 January 1991. Downloaded from P B Johnston Abstract trauma is a well recognised cause of rhegmato- Seventy-seven patients developed retinal genous retinal detachment, which was reported breaks following an episode of ocular con- by Eagling' to affect 4-6% of such injuries. The tusion, and 65 (84.4%) of these developed characteristics of postcontusion retinal detach- rhegmatogenous retinal detachment. Surgical ments were described by Cox et all and the treatment successfully restored or maintained mechanism ofbreak formation was elucidated by retinal apposition in 74 (96-1%) of the eyes. Delori et all who studied the effect of high speed Thirty-six (46-8%) eyes recovered visual acuity projectiles on enucleated pig eyes. Experimental of6/9orbetter. Ofthe retinal breaks recognised evidence indicates that retinal breaks form at the dialysis at the ora serrata was observed in 49 time of ocular impact. However, clinical reports eyes, of which 28 were situated at the lower show considerable delay in the diagnosis of temporal quadrant. Seventeen eyes had post-traumatic retinal detachment. For example, irregular breaks arising within necrotic retina Cox et all reported that only 30% of post- at the site of scleral impact. Twenty-four traumatic retinal detachments were diagnosed (31.2%) patients had retinal break or retinal within one month of injury, and Ross4 found detachment diagnosed within 24 hours ofinjury 40% in a similar period. and 49 (63-6%) within six weeks. Immediate The following study is of a series of patients retinal detachment was a feature of necrotic who developed retinal breaks or retinal detach- retinal breaks, while inferior oral dialyses led ment after ocular contusion. -

Vertical Perspective Medical Assistance Program
Kansas Vertical Perspective Medical Assistance Program December 2006 Provider Bulletin Number 688 General Providers Emergent and Nonemergent Diagnosis Code List Attached is a list of diagnosis codes and whether the Kansas Medical Assistance Program (KMAP) considers the code to be emergent or nonemergent. Providers are responsible for validating whether a particular diagnosis code is covered by KMAP under the beneficiary’s benefit plan and that all program requirements are met. This list does not imply or guarantee payment for listed diagnosis codes. Information about the Kansas Medical Assistance Program as well as provider manuals and other publications are on the KMAP Web site at https://www.kmap-state-ks.us. If you have any questions, please contact the KMAP Customer Service Center at 1-800-933-6593 (in-state providers) or (785) 274-5990 between 7:30 a.m. and 5:30 p.m., Monday through Friday. EDS is the fiscal agent and administrator of the Kansas Medical Assistance Program for the Kansas Health Policy Authority. Page 1 of 347 Emergency Indicators as noted by KMAP: N – Never considered emergent S – Sometimes considered emergent (through supporting medical documentation) Y – Always considered emergent Diagnosis Emergency Diagnosis Code Description Code Indicator 0010 Cholera due to Vibrio Cholerae S 0011 Cholera due to Vibrio Cholerae El Tor S 0019 Unspecified Cholera S 019 Late Effects of Tuberculosis N 0020 Typhoid Fever S 0021 Paratyphoid Fever A S 0022 Paratyphoid Fever B S 0023 Paratyphoid Fever C S 024 Glanders Y 025 Melioidosis -
Cases That Have Stuck with Me
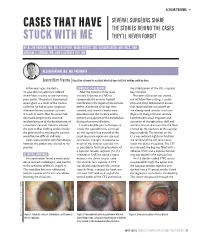
OCULAR TRAUMA s SEVERAL SURGEONS SHARE CASES THAT HAVE THE STORIES BEHIND THE CASES STUCK WITH ME THEY’LL NEVER FORGET BY ALLON BARSAM, MD, MA, FRCOPHTH; MARK KONTOS, MD; SOOSAN JACOB, MD, FRCS, DNB; MICHAEL E. SNYDER, MD; AND ELIZABETH YEU, MD ALLON BARSAM, MD, MA, FRCOPHTH Severe Blunt Trauma | A positive outcome for a patient who had been told that nothing could be done. A few years ago, I treated a SURGICAL PROCEDURE the stabilization of the IOL –capsular 41-year-old man who had suffered After the creation of the main bag complex. severe blunt trauma to one eye many incision, I injected an OVD to Phacoemulsification was carried years earlier. The patient experienced tamponade the anterior hyaloid out with low flow settings. I used a severe glare as a result of the trauma, membrane in the region of the zonular stop-and-chop technique to ensure such that he had to wear sunglasses defect. A cohesive OVD was then that minimal force was placed on whenever he was outdoors or even injected, and three iris hooks were the already weak zonular structures in a well-lit room. Also, his vision had placed to keep the iris back and to (Figure 2). Using a Simcoe cannula, decreased progressively since the prevent propagation of the iridodialysis I performed manual irrigation and incident because of the development of during phacoemulsification. aspiration of the epinuclear shell and a traumatic cataract. Doctors advised I used a double-pass technique to soft lens matter to ensure that the force the patient that nothing could remedy create the capsulorhexis, centered exerted on the contents of the capsular the glare and that treating the cataract on the capsular bag instead of the bag was gentle. -

Eleventh Edition
SUPPLEMENT TO April 15, 2009 A JOBSON PUBLICATION www.revoptom.com Eleventh Edition Joseph W. Sowka, O.D., FAAO, Dipl. Andrew S. Gurwood, O.D., FAAO, Dipl. Alan G. Kabat, O.D., FAAO Supported by an unrestricted grant from Alcon, Inc. 001_ro0409_handbook 4/2/09 9:42 AM Page 4 TABLE OF CONTENTS Eyelids & Adnexa Conjunctiva & Sclera Cornea Uvea & Glaucoma Viitreous & Retiina Neuro-Ophthalmic Disease Oculosystemic Disease EYELIDS & ADNEXA VITREOUS & RETINA Blow-Out Fracture................................................ 6 Asteroid Hyalosis ................................................33 Acquired Ptosis ................................................... 7 Retinal Arterial Macroaneurysm............................34 Acquired Entropion ............................................. 9 Retinal Emboli.....................................................36 Verruca & Papilloma............................................11 Hypertensive Retinopathy.....................................37 Idiopathic Juxtafoveal Retinal Telangiectasia...........39 CONJUNCTIVA & SCLERA Ocular Ischemic Syndrome...................................40 Scleral Melt ........................................................13 Retinal Artery Occlusion ......................................42 Giant Papillary Conjunctivitis................................14 Conjunctival Lymphoma .......................................15 NEURO-OPHTHALMIC DISEASE Blue Sclera .........................................................17 Dorsal Midbrain Syndrome ..................................45 -

Interesting and Artistic 1 2 3 Grand Prize Winner
s BEST OF 2018: PHOTO CONTEST 1 s SERGEI LUZHETSKIY, MD DANIEL DE SOUZA A Dog’s Cataract COSTA, MD s 2 A Spontaneous Displacement of the Lens WINNER GRAND PRIZE WINNER s PATRIK RAJS Gramophone Record 3 in the Eye INTERESTING AND ARTISTIC YONG s WINNERS OF KAM, MD Anterior CRST’S ANNUAL Segment Dysgenesis 2018 PHOTO CONTEST INTERESTING AND ARTISTIC 1 This is an image of an inherited cataract in a dog. 2 This photo is of the eye of a 46-year-old woman who presented with displacement of the lens into the anterior 4 chamber with no history of ocular trauma. 3 This photo is of the eye of a patient with presbyopia who underwent laser cataract surgery. A multifocal IOL was captured GRAND with a combination of two vintage Zeiss and Pentax lenses. WINNER PRIZE RARE AND UNUSUAL WINNER s This photo shows the eye of a newborn patient with DANIEL 4 increased IOP; a diffusely edematous, hazy, and enlarged DE SOUZA cornea; and an absent Schlemm canal and trabecular COSTA, MD meshwork on surgical exploration, consistent with severe A Prominent anterior segment dysgenesis. Symblepharon 5 The eye of this 5-year-old girl has epidermolysis bullosa and serious ocular manifestations of this condition. Biomicroscopy examination revealed the presence of 5 6 symblepharon in both eyes. The ocular complication was so severe that it deformed the palpebral anatomy. Significant keratoglobus in the eye of this patient with s AARON S. WANG, MD 6 Fish Tank Down Syndrome, who frequently rubs his eyes. This picture RARE AND UNUSUAL was taken just prior to corneal transplantation. -

To Assess the Intraoperative Complications in Small Incision Cataract Surgery and Visual Outcome
Acta Scientific Ophthalmology (ISSN: 2582-3191) Volume 3 Issue 8 August 2020 Research Article To Assess the Intraoperative Complications in Small Incision Cataract Surgery and Visual Outcome Smita Kunwar1*, Janak Poudel2 and Dr. Jyoti Kattige3 Received: July 14, 2020 1B. Optom Vittala International Institute of Ophthalmology, Bangalore, India Published: July 28, 2020 2B. Optom,Vittala International Institute of Ophthalmology Bangalore, India © All rights are reserved by Janak Poudel., 3Consultant Ophthalmologist, Fellowship in Glaucoma, Bangalore, India *Corresponding Author: Janak poudel B.Optom, Vittala International Institute of et al. Ophthalmology, Bangalore, India. DOI: 10.31080/ASOP.2020.03.0154 Abstract Background and Objective: Small incision cataract surgical procedure is the most normally performed surgical treatment for cataract in growing countries. This system is safe and effective to boom the output of cataract surgical services, at the identical time affordable. The present have a look at is undertaken to recognize the prevalence of intraoperative complications and how exceptional the complications may be minimized and dealt with and additionally its visual outcome. Method: A general of 471 instances turned into studied. Intraoperative complications have been studied and managed. Visual outcome following these complications have been studied with the aid of noting the BCVA after 1st week and 6th week of surgical treatment. Results: Out of 471 patients, 52(11%) patients The intraoperative complications were posterior capsular rupture occurred in 29 patients (55.8%), iris prolapse in 18 patients (34.6%), premature entry in 6 patients (11.5%), iridodialysis in 1 patient (1.9%), zonular dialysis in 1 patients (1.9%). 52 patients who had intraoperative problem came for follow up till sixth weeks, 28 cases (53.8%) had post-operative BCVA 6/9 or higher in 1st week and 24 cases had post-operative BCVA 6/18 or worse in 1st week. -

Wills Eye Manual 3Ed.Pdb
The Wills Eye Manual, 3rd Edition MedScut ISilo v1.0 CONTENTS Frontmatter CHAPTER 1 DIFFERENTIAL DIAGNOSIS OF OCULAR SYMPTOMS CHAPTER 2 DIFFERENTIAL DIAGNOSIS OF OCULAR SIGNS CHAPTER 3 TRAUMA 3.1 Chemical Burn 3.2 Corneal Abrasion 3.3 Corneal and Conjunctival Foreign Bodies 3.4 Conjunctival Laceration 3.5 Eyelid Laceration 3.6 Traumatic Iritis 3.7 Hyphema and Microhyphema 3.8 Commotio Retinae 3.9 Traumatic Choroidal Rupture 3.10 Orbital Blow-Out Fracture 3.11 Traumatic Retrobulbar Hemorrhage 3.12 Intraorbital Foreign Body 3.13 Corneal Laceration 3.14 Ruptured Globe and Penetrating Ocular Injury 3.15 Intraocular Foreign Body 3.16 Traumatic Optic Neuropathy CHAPTER 4 CORNEA 4.1 Superficial Punctate Keratitis (SPK) 4.2 Dry-eye Syndrome 4.3 Filamentary Keratopathy 4.4 Exposure Keratopathy 4.5 Neurotrophic Keratopathy 4.6 Recurrent Corneal Erosion 4.7 Thermal/Ultraviolet Keratopathy 4.8 Thygeson’s Superficial Punctate Keratopathy 4.9 Phlyctenulosis 4.10 Pterygium/Pingueculum 4.11 Band Keratopathy 4.12 Infectious Corneal Infiltrate/Ulcer 4.13 Fungal Keratitis 4.14 Acanthamoeba 4.15 Herpes Simplex Virus 4.16 Herpes Zoster Virus (HZV) 4.17 Contact Lens–related Problems 4.18 Contact Lens–induced Giant Papillary Conjunctivitis 4.19 Interstitial Keratitis 4.20 Peripheral Corneal Thinning 4.21 Dellen 4.22 Staphylococcal Hypersensitivity 4.23 Keratoconus 4.24 Corneal Dystrophies 4.25 Fuchs’ Endothelial Dystrophy 4.26 Wilson’s Disease (Hepatolenticular Degeneration) 4.27 Corneal Graft Rejection 4.28 Aphakic Bullous Keratopathy Pseudophakic Bullous -

1 42. Ophthalmology Daniel G Vaughan Ocular Emergencies It Is
42. Ophthalmology Daniel G Vaughan Ocular emergencies It is not necessary to refer every patient with an eye disease to an ophthalmologist for treatment. In general, sties, bacterial conjunctivitis, superficial trauma to the lids, corneas, and conjunctiva, and superficial corneal foreign bodies can be treated just as effectively by the surgeon or primary physician as by the ophthalmologist. More serious eye disease such as the following should be referred as soon as possible for specialized care: iritis, acute glaucoma, retinal detachment, strabismus, contusion of the globe, and severe corneal trauma or infection. In the management of acute ocular disorders, it is most important to establish a definitive diagnosis before prescribing treatment. The maxim "All red eyes are not pinkeye" is a useful one, and the physician must be alert for the more serious iritis, keratitis, or glaucoma. The common practice of prescribing "shotgun" topical antibiotic combinations containing corticosteroids is to be discouraged, because inappropriate use of steroids can lead to complications. This chapter attempts to summarize the basic principles and technics of diagnosis and management of common ocular problems, with special emphasis on emergencies, particularly those caused by trauma. Ocular emergencies may be classified as true emergencies or urgent cases. A true emergency is one in which the patient is suffering severe pain or in which a few hours' delay in treatment can lead to permanent ocular damage. An urgent case is one in which treatment should be started as soon as possible but in which a delay of a few days can be tolerated. Foreign Bodies If a patient complains of "something in my eye" and gives a consistent history, a foreign body is usually present even though it may not be readily visible. -

OC.UM.CP.0063 Visual Field Testing
ENVOLVE VISION BENEFITS, INC. INCLUDING ALL ASSOCIATED SUBSIDIARIES CLINICAL POLICY AND PROCEDURE DEPARTMENT: Utilization DOCUMENT NAME: Visual Field Testing Management (92081/92082/92083) PAGE: 1 of 63 REFERENCE NUMBER: OC.UM.CP.0063 EFFECTIVE DATE: 01/01/2018 REPLACES DOCUMENT: 277-UM-R8, 3036 MM-R6 RETIRED: REVIEWED: 10/23/2018 SPECIALIST REVIEW: Yes REVISED: 10/23/2018 PRODUCT TYPE: All COMMITTEE APPROVAL: 12/05/2018 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted standards of medical practice, peer-reviewed medical literature, government agency/program approval status, and other indicia of medical necessity. The purpose of this Clinical Policy is to provide a guide to medical necessity. Benefit determinations should be based in all cases on the applicable contract provisions governing plan benefits (“Benefit Plan Contract”) and applicable state and federal requirements including Local Coverage Determinations (LCDs), as well as applicable plan-level administrative policies and procedures. To the extent there are any conflicts between this Clinical Policy and the Benefit Plan Contract provisions, the Benefit Plan Contract provisions will control. Clinical policies are intended to be reflective of current scientific research and clinical thinking. This Clinical Policy is not intended to dictate to providers how to practice medicine, nor does it constitute a contract or guarantee regarding results. Providers are expected to exercise professional medical judgment in providing the most appropriate care, and are solely responsible for the medical advice and treatment of members. SUBJECT: Medical necessity determination for performance of visual field testing. -

International Council of Ophthalmology and Based on Their Curriculum 2009
HANDBOOK FOR JUNIOR RESIDENTS AND MEDICAL STUDENTS LEARNING EMERGENCY OPHTHALMOLOGY Compiled by The Task Force on Undergraduate Teaching in Ophthalmology of the International Council of Ophthalmology and based on their curriculum 2009 1 In this booklet we have put together common ophthalmic emergency conditions that we think you need to know and key ophthalmic disorders we think you need to have seen. There are descriptions and colour pictures of these conditions. This pocket sized book summaries the key points in the ophthalmology curriculum complied by the Task Force of the International Council of Ophthalmology and is a format that is very portable! Sue Lightman, Do Nhu Hon and Peter McCluskey On behalf of the International Council of Ophthalmology and Vietnam National Institute of Ophthalmology, Hanoi Medical University 2010 Other Contributing Authors with thanks Anh Dinh Kim , Anh Nguyen Quoc, Chau Hoang Thi Minh, Dong Pham Ngoc, Ha Tran Minh, Hon Do Nhu, Ngoc Do Quang, Quan Bui Dao, Richard Andrews, Thang Nguyen Canh, Thanh Pham Thi Kim, Thuy Nguyen Thi Thu, Thuy Vu Thi Bich, Tung Mai Quoc, Van Pham Thi Khanh, Van Pham Trong, Yen Nguyen Thu, Simon Taylor 2 Have you seen? Tick Do you Tick Note for you: if yes know if yes Remember how it is to look it up caused and treated? Trauma Periorbital haematoma Orbital blowout Lid laceration Subconjunctival Haemorrhage Chemical burns – cornea and conjunctiva Foreign body Corneal abrasion Hyphema Iridodialysis Cataract Lens subluxation /dislocation Intraocular foreign body Scleral rupture 3 Painful Red Eye Chalazion Dacryocystitis Orbital cellulitis Conjunctivitis Scleritis Episcleritis Viral keratitis Bacterial keratitis Shingles Uveitis Acute angle-closure glaucoma Endophthalmitis Sudden Painless Loss of Vision Vitreous haemorrhage Retinal tear/detachment Central retinal artery occlusion Central retinal vein occlusion Others 4 Proptosis VII nerve palsy TRAUMA Ocular trauma is very common, especially in developing countries. -

Osteo-Odonto Keratoprosthesis in Stevens-Johnson Syndrome: a Case
OOKPinSJS 窑CaseReport窑 Osteo-odontokeratoprosthesisinStevens-Johnson syndrome:acasereport 1DepartmentofOphthalmology,FacultyofMedicine,Universityof graftsmaynothelpinsuchcasestoprovideusefulvision. Malaya,KualaLumpur,Malaysia Forsuchcases,osteo-odontokeratoprosthesis(OOKP) 2Cornealservicesdepartment,SingaporeNationalEyeCentre& whichwasfirstdescribedbyStrampelli [1] andlateron DepartmentofOphthalmology,YongLooLinSchoolofMedicine, modifiedbyFalcinelli [2] andHull [3] isauseful NationalUniversityofSingapore,Singapore methodforvisualrehabilitationbecauseofitshigher Correspondenceto: ReddySC.DepartmentofOphthalmology, retentionrateandbetterlong-termvisualoutcome.Thisisa UCSISchoolofMedicine,TerengganuCampus,BukitKhor,21600 complexartificialcornealsurgicalprocedure thatis Marang,Terengganu,[email protected] performedintwostagesforvisualrehabilitationincasesof Received:2011-01-11Accepted:2011-03-10 cornealblindnesswithdryocularsurfaceinwhichcorneal transplantationwithamnioticmembraneandlimbalgrafts Abstract havefailed.Instageone,anautologuscaninetoothis ·AIM:Toreportasuccessfulosteo-odontokeratoprosthesis removed,modifiedto receivean optical polymethyl (OOKP)procedureinacaseofendstageofcornealblindness methacrylatecylinder;andimplantedinasubmuscular duetoStevens-Johnsonsyndrome(SJS). pocketunderthelowereyelidfor2-4months.Theocular ·METHODS:Aninterventionalcasereport. surfaceisdenudedandreplacedwithafullthicknessbuccal mucosa.Instagetwo,thetoothcylindercomplex(osteo- · RESULTS:Wedescribea35-year-oldIndianwoman,a odontolamina)isretrievedandsurroundingexcesssoft