Traumatic Iridodialysis Associated with Hyphema Secondary to Injury from a Bungee Cord
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Long Term Follow-Up of Limbal Transplantation for Unilateral Chemical Injuries: 1997-2014 Nikolaos S
perim Ex en l & ta a l ic O Tsiklis et al., J Clin Exp Ophthalmol 2016, 7:6 p in l h t C h f Journal of Clinical & Experimental a o DOI: 10.4172/2155-9570.1000621 l m l a o n l o r g u y o J Ophthalmology ISSN: 2155-9570 ResearchResearch Article Article Open Access Long Term Follow-up of Limbal Transplantation for Unilateral Chemical Injuries: 1997-2014 Nikolaos S. Tsiklis1, Dimitrios S. Siganos2, Ahmed Lubbad3, Vassilios P. Kozobolis4 and Charalambos S. Siganos1,3* 1Department of Ophthalmology, Heraklion University Hospital, Greece 2Heraklion, Crete, Vlemma Eye Institute of Athens, Greece 3Laboratory of Vision and Optics, School of Medicine, University of Crete, Greece 4Eye Institute of Thrace, Democritus University, Alexandroupolis, Greece Abstract Purpose: To evaluate the long term results of limbal transplantation (LT) in patients with unilateral total limbal stem cell deficiency (LSCD) after chemical injury. Methods: The study includes 22 eyes of 22 consecutive patients (20 males and 2 females) who presented with total LSCD after unilateral chemical burns and underwent Limbal transplantation (LT) in the Cornea Service of the Depart- ment of Ophthalmology at the Heraklion University Hospital in Crete during the period from 1997 to 2014. All 22 cases underwent Conjunctival Limbal autogaft (CLAU) while in 14 surgeries it was combined with amniotic membrane trans- plantation (AMT). A second stage penetrating keratoplasty (PKP) was performed in 11 cases for visual rehabilitation. The healing time, the changes in VA and the stability of epithelial ocular surface integrity were looked for. Results: One case failed within 3 months of surgery, while the rest 21 eyes after CLAU maintained ocular surface epithelial integrity during the follow up period (7.8 ± 3.5 years), and showed improvement partially or totally in corneal neovascularization, symblepharon and ocular motility. -

Ocular Injury; Hazard to Society: a Case Series
Quest Journals Journal of Medical and Dental Science Research Volume 7~ Issue 8 (2020) pp: 34-44 ISSN(Online) : 2394-076X ISSN (Print):2394-0751 www.questjournals.org Research Paper Ocular Injury; Hazard to Society: A Case Series Dr Rashmi kujur1, Dr Pallavi. M.P2, Dr Harshita Dubey3, Dr Varsha4 1Dept. of ophthalmology, Madhav dispensary JAH, GRMC, Gwalior, Madhyapradesh. 2Senior girls hostel, GRMC, Gwalior, Madhyapradesh. 3Senior girls hostel, GRMC, Gwalior, Madhyapradesh. 4Senior girls hostel, GRMC, Gwalior,Madhyapradesh. Corresponding Author: Dr.Pallavi.M.P ABSTRACT Purpose: To describe various types of ocular trauma due to different modes of injuryoccured on the same day Design: Prospective interventional study (case series) Materials & Methods: A series of cases of ocular trauma in different age group on the same day. Results: Five patients of ocular trauma were studied & managed. All five patients were males. Out of 5 cases, 3 cases had open globe injury and 2 cases had closed globe injury. Three out of five patients required surgical intervention while 2 patients were managed with medical therapy. Conclusion: This study describes the types and characteristics of ocular trauma presenting in eye department. The frequency of ocular trauma is common in males. Eye injuries resulting from ocular trauma pose a frequent threat to vision the world over. While afocussed history and prompt ocular examination are essential to immediate management, patient educationregarding safety precautions and risk reduction help to prevent future recurrences. KEYWORDS: Ocular morbidity, Ocular Injury, globe rupture, iridodialysis, fire cracker injury, hyphema, Road Traffic accident (RTA), loss of vision. Received 05 December, 2020; Accepted 20 December, 2020 © The author(s) 2020. -

Traumatic Glaucoma Mimicking Primary Open Angle Glaucoma
Traumatic glaucoma mimicking primary open angle glaucoma Xiaoming Duan ( [email protected] ) Research article Keywords: Traumatic glaucoma, Primary angle glaucoma, Trabecular pigmentation, Angle recession, Iridodialysis Posted Date: July 24th, 2019 DOI: https://doi.org/10.21203/rs.2.11863/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/9 Abstract Backgrounds To retrospectively analyze the clinical and ocular features in eyes with traumatic glaucoma misdiagnosed as primary open angle glaucoma (POAG). Methods We reviewed nineteen eyes with traumatic glaucoma misdiagnosed and collected their ocular and supplementary examination results. Results The outpatient age was 47.1±12.8 years old. The traumatic history was from 1 to 40 years. The history of hand or stone was present about 21.1% of patients, followed by balls (15.8%) and wooden stick (15.8%). The peak IOPs were 33.0±10.6mmHg. Iridodialysis was seen in 2 patients. Trabecular pigmentation grade more than 3 was noticed in 15 patients. Angle recession was found in all patients. No patient was found lens location and fundus damage. Conclusions Patients with long traumatic history, mild ocular signs and insidious symptoms were more likely to be misdiagnosed. It might be more prudent to diagnose as POAG while there was signicant difference in the condition of both eyes. Background Glaucoma is characterized by retinal ganglion cell degeneration, alterations in optic nerve head topography, and associated visual eld (VF) loss. It was known as a group of diseases, not a single disease. It was divided into many types, including in primary, secondary and developmental glaucoma. -

Traumatic Retinal Detachment Br J Ophthalmol: First Published As 10.1136/Bjo.75.1.18 on 1 January 1991
18 BritishJournalofOphthalmology, 1991,75, 18-21 Traumatic retinal detachment Br J Ophthalmol: first published as 10.1136/bjo.75.1.18 on 1 January 1991. Downloaded from P B Johnston Abstract trauma is a well recognised cause of rhegmato- Seventy-seven patients developed retinal genous retinal detachment, which was reported breaks following an episode of ocular con- by Eagling' to affect 4-6% of such injuries. The tusion, and 65 (84.4%) of these developed characteristics of postcontusion retinal detach- rhegmatogenous retinal detachment. Surgical ments were described by Cox et all and the treatment successfully restored or maintained mechanism ofbreak formation was elucidated by retinal apposition in 74 (96-1%) of the eyes. Delori et all who studied the effect of high speed Thirty-six (46-8%) eyes recovered visual acuity projectiles on enucleated pig eyes. Experimental of6/9orbetter. Ofthe retinal breaks recognised evidence indicates that retinal breaks form at the dialysis at the ora serrata was observed in 49 time of ocular impact. However, clinical reports eyes, of which 28 were situated at the lower show considerable delay in the diagnosis of temporal quadrant. Seventeen eyes had post-traumatic retinal detachment. For example, irregular breaks arising within necrotic retina Cox et all reported that only 30% of post- at the site of scleral impact. Twenty-four traumatic retinal detachments were diagnosed (31.2%) patients had retinal break or retinal within one month of injury, and Ross4 found detachment diagnosed within 24 hours ofinjury 40% in a similar period. and 49 (63-6%) within six weeks. Immediate The following study is of a series of patients retinal detachment was a feature of necrotic who developed retinal breaks or retinal detach- retinal breaks, while inferior oral dialyses led ment after ocular contusion. -

Acute Management of Penetrating Eye Injury and Ruptured Globe
Acute management of penetrating eye injury and ruptured globe Disclaimer SEE ALSO: Endophthalmitis, Hyphaema, Peri- and post-operative Management of Penetrating Eye Injury and Ruptured Globe, Procedure for Management of Eye Trauma DESCRIPTION – The immediate management of penetrating eye injury (PEI), with or without intra-ocular foreign body (IOFB), and ruptured globe to maximise outcome. HOW TO ASSESS Red Flags: Immediate Advanced Trauma Life Support (ATLS) assessment: Airway, Breathing, Circulation, Disability, Exposure (ABCDE) Establish mechanism of injury to exclude other injuries which may require management at a general hospital, e.g. cervical spine, head injury Open globe should be examined carefully to avoid extrusion of intraocular contents Consider occult injury if mechanism suggestive Shield at all times (do not pad) Early referral for pre-anaesthetic assessment and medical review (if needed), to assess pre-existing or new medical issues and the patient’s suitability for management at RVEEH. Preoperative bloods, ECG and imaging as indicated. EXPECTED PATIENT Refer to and complete the ‘Emergency Expect Form’ (MR 37) in the Emergency Department. Make sure patient’s contact details (mobile) are recorded. Do not accept patients who have injuries other than ocular i.e. multi-trauma or who are medically unstable. Children under the age of 6 months should be referred directly to the Royal Children’s Hospital. Children aged from 6 months to 2 years with significant co-morbidities may not be appropriate to be managed at RVEEH. 1 Penetrating eye injury and ruptured globe CPG v4 19092017 All paediatric patients which may need referral to RCH, must be discussed with RCH Ophthalmology registrar or Consultant PRIOR to referral in order to confirm specialty coverage and operating theatre availability should surgery be required. -

Vertical Perspective Medical Assistance Program
Kansas Vertical Perspective Medical Assistance Program December 2006 Provider Bulletin Number 688 General Providers Emergent and Nonemergent Diagnosis Code List Attached is a list of diagnosis codes and whether the Kansas Medical Assistance Program (KMAP) considers the code to be emergent or nonemergent. Providers are responsible for validating whether a particular diagnosis code is covered by KMAP under the beneficiary’s benefit plan and that all program requirements are met. This list does not imply or guarantee payment for listed diagnosis codes. Information about the Kansas Medical Assistance Program as well as provider manuals and other publications are on the KMAP Web site at https://www.kmap-state-ks.us. If you have any questions, please contact the KMAP Customer Service Center at 1-800-933-6593 (in-state providers) or (785) 274-5990 between 7:30 a.m. and 5:30 p.m., Monday through Friday. EDS is the fiscal agent and administrator of the Kansas Medical Assistance Program for the Kansas Health Policy Authority. Page 1 of 347 Emergency Indicators as noted by KMAP: N – Never considered emergent S – Sometimes considered emergent (through supporting medical documentation) Y – Always considered emergent Diagnosis Emergency Diagnosis Code Description Code Indicator 0010 Cholera due to Vibrio Cholerae S 0011 Cholera due to Vibrio Cholerae El Tor S 0019 Unspecified Cholera S 019 Late Effects of Tuberculosis N 0020 Typhoid Fever S 0021 Paratyphoid Fever A S 0022 Paratyphoid Fever B S 0023 Paratyphoid Fever C S 024 Glanders Y 025 Melioidosis -

CAUSES, COMPLICATIONS &TREATMENT of A“RED EYE”
CAUSES, COMPLICATIONS & TREATMENT of a “RED EYE” 8 Most cases of “red eye” seen in general practice are likely to be conjunctivitis or a superficial corneal injury, however, red eye can also indicate a serious eye condition such as acute angle glaucoma, iritis, keratitis or scleritis. Features such as significant pain, photophobia, reduced visual acuity and a unilateral presentation are “red flags” that a sight-threatening condition may be present. In the absence of specialised eye examination equipment, such as a slit lamp, General Practitioners must rely on identifying these key features to know which patients require referral to an Ophthalmologist for further assessment. Is it conjunctivitis or is it something more Iritis is also known as anterior uveitis; posterior uveitis is serious? inflammation of the choroid (choroiditis). Complications include glaucoma, cataract and macular oedema. The most likely cause of a red eye in patients who present to 4. Scleritis is inflammation of the sclera. This is a very rare general practice is conjunctivitis. However, red eye can also be presentation, usually associated with autoimmune a feature of a more serious eye condition, in which a delay in disease, e.g. rheumatoid arthritis. treatment due to a missed diagnosis can result in permanent 5. Penetrating eye injury or embedded foreign body; red visual loss. In addition, the inappropriate use of antibacterial eye is not always a feature topical eye preparations contributes to antimicrobial 6. Acid or alkali burn to the eye resistance. The patient history will usually identify a penetrating eye injury Most general practice clinics will not have access to specialised or chemical burn to the eye, but further assessment may be equipment for eye examination, e.g. -
Cases That Have Stuck with Me
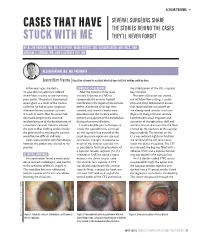
OCULAR TRAUMA s SEVERAL SURGEONS SHARE CASES THAT HAVE THE STORIES BEHIND THE CASES STUCK WITH ME THEY’LL NEVER FORGET BY ALLON BARSAM, MD, MA, FRCOPHTH; MARK KONTOS, MD; SOOSAN JACOB, MD, FRCS, DNB; MICHAEL E. SNYDER, MD; AND ELIZABETH YEU, MD ALLON BARSAM, MD, MA, FRCOPHTH Severe Blunt Trauma | A positive outcome for a patient who had been told that nothing could be done. A few years ago, I treated a SURGICAL PROCEDURE the stabilization of the IOL –capsular 41-year-old man who had suffered After the creation of the main bag complex. severe blunt trauma to one eye many incision, I injected an OVD to Phacoemulsification was carried years earlier. The patient experienced tamponade the anterior hyaloid out with low flow settings. I used a severe glare as a result of the trauma, membrane in the region of the zonular stop-and-chop technique to ensure such that he had to wear sunglasses defect. A cohesive OVD was then that minimal force was placed on whenever he was outdoors or even injected, and three iris hooks were the already weak zonular structures in a well-lit room. Also, his vision had placed to keep the iris back and to (Figure 2). Using a Simcoe cannula, decreased progressively since the prevent propagation of the iridodialysis I performed manual irrigation and incident because of the development of during phacoemulsification. aspiration of the epinuclear shell and a traumatic cataract. Doctors advised I used a double-pass technique to soft lens matter to ensure that the force the patient that nothing could remedy create the capsulorhexis, centered exerted on the contents of the capsular the glare and that treating the cataract on the capsular bag instead of the bag was gentle. -

Eleventh Edition
SUPPLEMENT TO April 15, 2009 A JOBSON PUBLICATION www.revoptom.com Eleventh Edition Joseph W. Sowka, O.D., FAAO, Dipl. Andrew S. Gurwood, O.D., FAAO, Dipl. Alan G. Kabat, O.D., FAAO Supported by an unrestricted grant from Alcon, Inc. 001_ro0409_handbook 4/2/09 9:42 AM Page 4 TABLE OF CONTENTS Eyelids & Adnexa Conjunctiva & Sclera Cornea Uvea & Glaucoma Viitreous & Retiina Neuro-Ophthalmic Disease Oculosystemic Disease EYELIDS & ADNEXA VITREOUS & RETINA Blow-Out Fracture................................................ 6 Asteroid Hyalosis ................................................33 Acquired Ptosis ................................................... 7 Retinal Arterial Macroaneurysm............................34 Acquired Entropion ............................................. 9 Retinal Emboli.....................................................36 Verruca & Papilloma............................................11 Hypertensive Retinopathy.....................................37 Idiopathic Juxtafoveal Retinal Telangiectasia...........39 CONJUNCTIVA & SCLERA Ocular Ischemic Syndrome...................................40 Scleral Melt ........................................................13 Retinal Artery Occlusion ......................................42 Giant Papillary Conjunctivitis................................14 Conjunctival Lymphoma .......................................15 NEURO-OPHTHALMIC DISEASE Blue Sclera .........................................................17 Dorsal Midbrain Syndrome ..................................45 -

Visual Outcomes of Hyphema in Closed Globe Injury, Managed at a Tertiary Care Institute
Jebmh.com Original Research Article Visual Outcomes of Hyphema in Closed Globe Injury, Managed at a Tertiary Care Institute Prasanta Kumar Nanda1, Jayaram Meher2, Bishnuprasad Rath3 1Professor and HOD, Department of Ophthalmology, SCB Medical College and Hospital, Cuttack, Odisha. 2Postgraduate Resident, Department of Ophthalmology, SCB Medical College and Hospital, Cuttack, Odisha. 3Postgraduate Resident, Department of Ophthalmology, SCB Medical College and Hospital, Cuttack, Odisha. ABSTRACT BACKGROUND An accumulation of blood in the anterior chamber is known as hyphema. An injury Corresponding Author: to the eye or its surrounding tissue, constitutes most of the calls for emergency in Dr. Jayaram Meher, SR Hostel, Room No. 166, ophthalmology. This study aims to determine the causes and visual outcome SCB Medical College and Hospital, following treatment in patients with hyphema following closed globe injury. Cuttack, Odisha. E-mail: [email protected] METHODS DOI: 10.18410/jebmh/2020/15 This is a prospective study involving 76 patients which done from February 2019 to September 2019 in the Department Of Ophthalmology. Detailed history was Financial or Other Competing Interests: None. taken regarding the type, mode of injury, duration of injury and the eye affected. Lid and adnexal injuries, visual acuity at the time of admission were recorded. How to Cite This Article: Detailed anterior segment evaluation on slit lamp was done. Appropriate treatment Nanda PK, Meher J, Rath B. Visual was given. The patients were followed after 1 week, and at the end of 6 weeks. outcomes of hyphema in closed globe injury, managed at a tertiary care RESULTS institute. J. Evid. Based Med. Healthc. 2020; 7(2), 68-72. -

Interesting and Artistic 1 2 3 Grand Prize Winner
s BEST OF 2018: PHOTO CONTEST 1 s SERGEI LUZHETSKIY, MD DANIEL DE SOUZA A Dog’s Cataract COSTA, MD s 2 A Spontaneous Displacement of the Lens WINNER GRAND PRIZE WINNER s PATRIK RAJS Gramophone Record 3 in the Eye INTERESTING AND ARTISTIC YONG s WINNERS OF KAM, MD Anterior CRST’S ANNUAL Segment Dysgenesis 2018 PHOTO CONTEST INTERESTING AND ARTISTIC 1 This is an image of an inherited cataract in a dog. 2 This photo is of the eye of a 46-year-old woman who presented with displacement of the lens into the anterior 4 chamber with no history of ocular trauma. 3 This photo is of the eye of a patient with presbyopia who underwent laser cataract surgery. A multifocal IOL was captured GRAND with a combination of two vintage Zeiss and Pentax lenses. WINNER PRIZE RARE AND UNUSUAL WINNER s This photo shows the eye of a newborn patient with DANIEL 4 increased IOP; a diffusely edematous, hazy, and enlarged DE SOUZA cornea; and an absent Schlemm canal and trabecular COSTA, MD meshwork on surgical exploration, consistent with severe A Prominent anterior segment dysgenesis. Symblepharon 5 The eye of this 5-year-old girl has epidermolysis bullosa and serious ocular manifestations of this condition. Biomicroscopy examination revealed the presence of 5 6 symblepharon in both eyes. The ocular complication was so severe that it deformed the palpebral anatomy. Significant keratoglobus in the eye of this patient with s AARON S. WANG, MD 6 Fish Tank Down Syndrome, who frequently rubs his eyes. This picture RARE AND UNUSUAL was taken just prior to corneal transplantation. -

SEEING Beyond Abuse
SEEING Beyond Abuse By Jessica L. Young, O.D. Pennsylvania Optometric Association’s 2010 Young Optometrist of the Year Many may think that visiting an eye doctor would be the last place for an abuse victim to go. After reading this article, you may disagree. One day, a 49 year- old woman came to see me for a routine eye examination. Her vision was getting a little worse and she thought, "Maybe I need a new pair of glasses." During the examination, I noticed a tear in the iris of her right eye. Upon checking her eye pressure I found that it was elevated in her right eye. I asked the woman if she had ever sustained any injuries to her eyes. She confirmed that she had in fact been hit many times in her eyes and face years ago by a former boyfriend. I explained how the trauma had damaged her eye and the increased eye pressure could lead to optic nerve damage and vision loss if left untreated. We decided to begin medicated eye drops to lower the eye pressure. So far the drops are successfully keeping the pressure down, reducing her chances of vision loss. This woman very well may have lost her eyesight had she not happened to come for a regular eye exam. Physical assault resulting in trauma to the eye can have both immediate and lasting effects. If trauma to the eye occurs, urgent medical attention should be sought to treat any immediate damage. Visiting an eye doctor is prudent for anyone who has ever sustained trauma to the eye at any time.