Extended Ophthalmoscopy and Fundus Photography) (L33567)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Wildlife Ophthalmology
Wildlife Ophthalmology DR. HEATHER REID TORONTO WILDLIFE CENTRE TORONTO, ON CANADA Why understand eyes? Wildlife need to have excellent vision to survive in the wild Eye related problems are common in wildlife admitted to rehabilitation centers What we will cover Anatomy of the eye Differences between birds and mammals The eye exam Recognizing common problems Prognosis Treatment options When to see the vet Anatomy Around the Eye: Muscles & nerves Skin Eye lids Nictitating eyelid Conjunctiva & sclera Tear glands & ducts Ossicles (birds) Anatomy Front of the Eye: Cornea Iris Pupil Ciliary body Anterior Chamber Aqueous humor Anatomy Back of the Eye: Lens Retina Optic nerve Choroid Pecten (birds) Posterior Chamber Vitreous humor Fundus of the Eye Mammal Eye Bird Eye The Avian Eye - Differences Small eye size in most birds and small pupil size makes it hard to examine Can control the size of their pupil Lower eyelid more developed The nictitating membrane spreads the tears allowing birds to blink less Moves horizontally across eye The Avian Eye - Differences Eyes are not as protected by skull Less muscles around eye so less eye movement Boney ossicles support the eye Three main eye shapes; flat, globose & tubular The Avian Eye - Differences Four different color receptors compared to the three in mammals means better color detail Can see in the ultraviolet range Higher flicker rate – can detect lights that flicker at more than 100 flashes per second (humans detect at 50) The Avian Eye - Differences In some species the eye -

Ocular Injury; Hazard to Society: a Case Series
Quest Journals Journal of Medical and Dental Science Research Volume 7~ Issue 8 (2020) pp: 34-44 ISSN(Online) : 2394-076X ISSN (Print):2394-0751 www.questjournals.org Research Paper Ocular Injury; Hazard to Society: A Case Series Dr Rashmi kujur1, Dr Pallavi. M.P2, Dr Harshita Dubey3, Dr Varsha4 1Dept. of ophthalmology, Madhav dispensary JAH, GRMC, Gwalior, Madhyapradesh. 2Senior girls hostel, GRMC, Gwalior, Madhyapradesh. 3Senior girls hostel, GRMC, Gwalior, Madhyapradesh. 4Senior girls hostel, GRMC, Gwalior,Madhyapradesh. Corresponding Author: Dr.Pallavi.M.P ABSTRACT Purpose: To describe various types of ocular trauma due to different modes of injuryoccured on the same day Design: Prospective interventional study (case series) Materials & Methods: A series of cases of ocular trauma in different age group on the same day. Results: Five patients of ocular trauma were studied & managed. All five patients were males. Out of 5 cases, 3 cases had open globe injury and 2 cases had closed globe injury. Three out of five patients required surgical intervention while 2 patients were managed with medical therapy. Conclusion: This study describes the types and characteristics of ocular trauma presenting in eye department. The frequency of ocular trauma is common in males. Eye injuries resulting from ocular trauma pose a frequent threat to vision the world over. While afocussed history and prompt ocular examination are essential to immediate management, patient educationregarding safety precautions and risk reduction help to prevent future recurrences. KEYWORDS: Ocular morbidity, Ocular Injury, globe rupture, iridodialysis, fire cracker injury, hyphema, Road Traffic accident (RTA), loss of vision. Received 05 December, 2020; Accepted 20 December, 2020 © The author(s) 2020. -

Smartphone-Based Dilated Fundus Photography and Near Visual Acuity Testing As Inexpensive Screening Tools to Detect Referral Warranted Diabetic Eye Disease
Smartphone-Based Dilated Fundus Photography and Near Visual Acuity Testing as Inexpensive Screening Tools to Detect Referral Warranted Diabetic Eye Disease BRIAN C. TOY, MD,*† DAVID J. MYUNG, MD, PHD,*† LINGMIN HE, MD,*† CAROLYN K. PAN, MD,*† ROBERT T. CHANG, MD,* ALISON POLKINHORNE, MA,‡ DOUGLAS MERRELL, BS,‡ DOUG FOSTER, MBA,‡ MARK S. BLUMENKRANZ, MD* Purpose: To compare clinical assessment of diabetic eye disease by standard dilated examination with data gathered using a smartphone-based store-and-forward teleoph- thalmology platform. Methods: 100 eyes of 50 adult patients with diabetes from a health care safety-net ophthalmology clinic. All patients underwent comprehensive ophthalmic examination. Concurrently, a smartphone was used to estimate near visual acuity and capture anterior and dilated posterior segment photographs, which underwent masked, standardized review. Quantitative comparison of clinic and smartphone-based data using descriptive, kappa, Bland-Altman, and receiver operating characteristic analyses was performed. Results: Smartphone visual acuity was successfully measured in all eyes. Anterior and posterior segment photography was of sufficient quality to grade in 96 and 98 eyes, respectively. There was good correlation between clinical Snellen and smartphone visual acuity measurements (rho = 0.91). Smartphone-acquired fundus photographs demon- strated 91% sensitivity and 99% specificity to detect moderate nonproliferative and worse diabetic retinopathy, with good agreement between clinic and photograph grades (kappa = 0.91 ± 0.1, P , 0.001; AUROC = 0.97, 95% confidence interval, 0.93–1). Conclusion: The authors report a smartphone-based telemedicine system that demon- strated sensitivity and specificity to detect referral-warranted diabetic eye disease as a proof-of-concept. Additional studies are warranted to evaluate this approach to expanding screening for diabetic retinopathy. -

Effects of Nd:YAG Laser Capsulotomy in Posterior Capsular Opacification
Original Research Article Effects of Nd:YAG laser capsulotomy in posterior capsular opacification Praveen Kumar G S1, Lavanya P2*, Raviprakash D3 1Assistant Professor, 2Associate Professor, 3Professor & HOD, Department of Ophthalmology, Shridevi institute of Medical Sciences and Research Hospital, Sira Road, NH-4 Bypass Road, Tumkur- 572106, INDIA. Email: [email protected] Abstract Background: Posterior capsular opacification (PCO) is the most common long-term complication of cataract surgery in both phacoemulsification and extracapsular cataract extraction (ECCE). The overall incidence of PCO and the incidence of neodymium-doped yttrium–aluminum–garnet (Nd:YAG) laser posterior capsulotomy has decreased from 50% in the 1980s and early 1990s to less than 10% today. Reported complications of Nd:YAG laser posterior capsulotomy include elevated intraocular pressure, iritis, corneal damage, intraocular lens (IOL) damage, cystoids macular edema, disruption of the anterior hyaloid surface, increased risk of retinal detachment, and IOL movement or dislocation. In some patients, a refraction change is noticed after Nd:YAG laser posterior capsulotomy, but proving this remains difficult. Materials and Methods: Nd; YAG LASER capsulotomy was performed in 200 eyes of 200 patients, some with pseudophakia and some with aphakia at Kurnool medical college, Kurnool. They were followed up between October 2008 and September 2010. Results: Elevation of IOP has been well documented after anterior segment laser procedures. The IOP rise after YAG laser posterior capsulotomy is of short duration starting about 1 hr after laser procedure and lasting for 24 hrs. In this study, in 1case IOP came down to normal level after 3 days and in another case after 7 days. -

Traumatic Retinal Detachment Br J Ophthalmol: First Published As 10.1136/Bjo.75.1.18 on 1 January 1991
18 BritishJournalofOphthalmology, 1991,75, 18-21 Traumatic retinal detachment Br J Ophthalmol: first published as 10.1136/bjo.75.1.18 on 1 January 1991. Downloaded from P B Johnston Abstract trauma is a well recognised cause of rhegmato- Seventy-seven patients developed retinal genous retinal detachment, which was reported breaks following an episode of ocular con- by Eagling' to affect 4-6% of such injuries. The tusion, and 65 (84.4%) of these developed characteristics of postcontusion retinal detach- rhegmatogenous retinal detachment. Surgical ments were described by Cox et all and the treatment successfully restored or maintained mechanism ofbreak formation was elucidated by retinal apposition in 74 (96-1%) of the eyes. Delori et all who studied the effect of high speed Thirty-six (46-8%) eyes recovered visual acuity projectiles on enucleated pig eyes. Experimental of6/9orbetter. Ofthe retinal breaks recognised evidence indicates that retinal breaks form at the dialysis at the ora serrata was observed in 49 time of ocular impact. However, clinical reports eyes, of which 28 were situated at the lower show considerable delay in the diagnosis of temporal quadrant. Seventeen eyes had post-traumatic retinal detachment. For example, irregular breaks arising within necrotic retina Cox et all reported that only 30% of post- at the site of scleral impact. Twenty-four traumatic retinal detachments were diagnosed (31.2%) patients had retinal break or retinal within one month of injury, and Ross4 found detachment diagnosed within 24 hours ofinjury 40% in a similar period. and 49 (63-6%) within six weeks. Immediate The following study is of a series of patients retinal detachment was a feature of necrotic who developed retinal breaks or retinal detach- retinal breaks, while inferior oral dialyses led ment after ocular contusion. -

Vertical Perspective Medical Assistance Program
Kansas Vertical Perspective Medical Assistance Program December 2006 Provider Bulletin Number 688 General Providers Emergent and Nonemergent Diagnosis Code List Attached is a list of diagnosis codes and whether the Kansas Medical Assistance Program (KMAP) considers the code to be emergent or nonemergent. Providers are responsible for validating whether a particular diagnosis code is covered by KMAP under the beneficiary’s benefit plan and that all program requirements are met. This list does not imply or guarantee payment for listed diagnosis codes. Information about the Kansas Medical Assistance Program as well as provider manuals and other publications are on the KMAP Web site at https://www.kmap-state-ks.us. If you have any questions, please contact the KMAP Customer Service Center at 1-800-933-6593 (in-state providers) or (785) 274-5990 between 7:30 a.m. and 5:30 p.m., Monday through Friday. EDS is the fiscal agent and administrator of the Kansas Medical Assistance Program for the Kansas Health Policy Authority. Page 1 of 347 Emergency Indicators as noted by KMAP: N – Never considered emergent S – Sometimes considered emergent (through supporting medical documentation) Y – Always considered emergent Diagnosis Emergency Diagnosis Code Description Code Indicator 0010 Cholera due to Vibrio Cholerae S 0011 Cholera due to Vibrio Cholerae El Tor S 0019 Unspecified Cholera S 019 Late Effects of Tuberculosis N 0020 Typhoid Fever S 0021 Paratyphoid Fever A S 0022 Paratyphoid Fever B S 0023 Paratyphoid Fever C S 024 Glanders Y 025 Melioidosis -

Coding Competencies for Ophthalmic Techs – 2020 Coding Update
3/5/2020 Coding Competencies for Ophthalmic Techs – 2020 Coding Update OAO Ophthalmic Medical Technology Friday, March 13, 2020 Joy Woodke, COE, OCS, OCSR 1 Financial Disclosure Joy Woodke, COE, OCS o This presenter does not have a financial interest or relationship to disclose relative to this activity. o Academy Coding & Practice Management Executive 2 Topics 2020 Coding Updates Coding Competencies Diagnostic testing services Modifiers Tech Takeaways Understanding insurance policies Ongoing coding education Resources 3 1 3/5/2020 2020 Coding Updates Extended Ophthalmoscopy & Cataract Surgery 4 Extended Ophthalmoscopy (EO) • CPT eliminated initial and subsequent codes for EO • New codes for drawing of • Peripheral retina, with scleral depression: 5% in work value over deleted initial EO • Optic nerve or macula: 32% compared to deleted initial EO 5 Extended Ophthalmoscopy (EO) • 92225 Ophthalmoscopy, extended, with retinal drawing (eg, for retinal detachment, melanoma), with interpretation and report; initial • 92226 subsequent 6 2 3/5/2020 Extended Ophthalmoscopy (EO) 92201 Ophthalmoscopy, extended; with retinal drawing and scleral depression of peripheral retinal disease (eg, for retinal tear, retinal detachment, retinal tumor) with interpretation and report, unilateral or bilateral 7 Ophthalmoscopy 92201 8 8 Extended Ophthalmoscopy (EO) 92202 with drawing of optic nerve or macula (eg, for glaucoma, macular pathology, tumor) with interpretation and report, unilateral or bilateral 9 3 3/5/2020 Ophthalmoscopy 92202 10 Extended Ophthalmoscopy (EO) • Payment was unilateral. 2020 is bilateral. 2019 2020 92225 $29.87 per eye 92201 $27.21 Only bill for the eye that has 92202 $17.21 pathology. 92226 $27.63 per eye Only bill for the eye that has pathology 11 Extended Ophthalmoscopy (EO) • Payment is the same whether one or both eyes are examined and pathology is drawn and labeled. -

Endoscopic Vitreoretinal Surgery: Principles, Applications and New Directions Radwan S
Ajlan et al. Int J Retin Vitr (2019) 5:15 International Journal https://doi.org/10.1186/s40942-019-0165-z of Retina and Vitreous REVIEW Open Access Endoscopic vitreoretinal surgery: principles, applications and new directions Radwan S. Ajlan1*, Aarsh A. Desai2 and Martin A. Mainster1 Abstract Purpose: To analyze endoscopic vitreoretinal surgery principles, applications, challenges and potential technological advances. Background: Microendoscopic imaging permits vitreoretinal surgery for tissues that are not visible using operat- ing microscopy ophthalmoscopy. Evolving instrumentation may overcome some limitations of current endoscopic technology. Analysis: Transfer of the fine detail in endoscopic vitreoretinal images to extraocular video cameras is constrained currently by the caliber limitations of intraocular probes in ophthalmic surgery. Gradient index and Hopkins rod lenses provide high resolution ophthalmoscopy but restrict surgical manipulation. Fiberoptic coherent image guides offer surgical maneuverability but reduce imaging resolution. Coaxial endoscopic illumination can highlight delicate vitreo- retinal structures difficult to image in chandelier or endoilluminator diffuse, side-scattered lighting. Microendoscopy’s ultra-high magnification video monitor images can reveal microscopic tissue details blurred partly by ocular media aberrations in contemporary surgical microscope ophthalmoscopy, thereby providing a lower resolution, invasive alternative to confocal fundus imaging. Endoscopic surgery is particularly useful when ocular -

2Nd Quarter 2001 Medicare Part a Bulletin
In This Issue... From the Intermediary Medical Director Medical Review Progressive Corrective Action ......................................................................... 3 General Information Medical Review Process Revision to Medical Record Requests ................................................ 5 General Coverage New CLIA Waived Tests ............................................................................................................. 8 Outpatient Hospital Services Correction to the Outpatient Services Fee Schedule ................................................................. 9 Skilled Nursing Facility Services Fee Schedule and Consolidated Billing for Skilled Nursing Facility (SNF) Services ............. 12 Fraud and Abuse Justice Recovers Record $1.5 Billion in Fraud Payments - Highest Ever for One Year Period ........................................................................................... 20 Bulletin Medical Policies Use of the American Medical Association’s (AMA’s) Current Procedural Terminology (CPT) Codes on Contractors’ Web Sites ................................................................................. 21 Outpatient Prospective Payment System January 2001 Update: Coding Information for Hospital Outpatient Prospective Payment System (OPPS) ......................................................................................................................... 93 he Medicare A Bulletin Providers Will Be Asked to Register Tshould be shared with all to Receive Medicare Bulletins and health care -
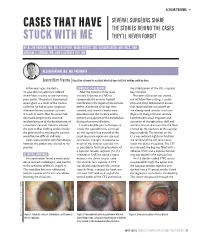
Cases That Have Stuck with Me
OCULAR TRAUMA s SEVERAL SURGEONS SHARE CASES THAT HAVE THE STORIES BEHIND THE CASES STUCK WITH ME THEY’LL NEVER FORGET BY ALLON BARSAM, MD, MA, FRCOPHTH; MARK KONTOS, MD; SOOSAN JACOB, MD, FRCS, DNB; MICHAEL E. SNYDER, MD; AND ELIZABETH YEU, MD ALLON BARSAM, MD, MA, FRCOPHTH Severe Blunt Trauma | A positive outcome for a patient who had been told that nothing could be done. A few years ago, I treated a SURGICAL PROCEDURE the stabilization of the IOL –capsular 41-year-old man who had suffered After the creation of the main bag complex. severe blunt trauma to one eye many incision, I injected an OVD to Phacoemulsification was carried years earlier. The patient experienced tamponade the anterior hyaloid out with low flow settings. I used a severe glare as a result of the trauma, membrane in the region of the zonular stop-and-chop technique to ensure such that he had to wear sunglasses defect. A cohesive OVD was then that minimal force was placed on whenever he was outdoors or even injected, and three iris hooks were the already weak zonular structures in a well-lit room. Also, his vision had placed to keep the iris back and to (Figure 2). Using a Simcoe cannula, decreased progressively since the prevent propagation of the iridodialysis I performed manual irrigation and incident because of the development of during phacoemulsification. aspiration of the epinuclear shell and a traumatic cataract. Doctors advised I used a double-pass technique to soft lens matter to ensure that the force the patient that nothing could remedy create the capsulorhexis, centered exerted on the contents of the capsular the glare and that treating the cataract on the capsular bag instead of the bag was gentle. -

Eleventh Edition
SUPPLEMENT TO April 15, 2009 A JOBSON PUBLICATION www.revoptom.com Eleventh Edition Joseph W. Sowka, O.D., FAAO, Dipl. Andrew S. Gurwood, O.D., FAAO, Dipl. Alan G. Kabat, O.D., FAAO Supported by an unrestricted grant from Alcon, Inc. 001_ro0409_handbook 4/2/09 9:42 AM Page 4 TABLE OF CONTENTS Eyelids & Adnexa Conjunctiva & Sclera Cornea Uvea & Glaucoma Viitreous & Retiina Neuro-Ophthalmic Disease Oculosystemic Disease EYELIDS & ADNEXA VITREOUS & RETINA Blow-Out Fracture................................................ 6 Asteroid Hyalosis ................................................33 Acquired Ptosis ................................................... 7 Retinal Arterial Macroaneurysm............................34 Acquired Entropion ............................................. 9 Retinal Emboli.....................................................36 Verruca & Papilloma............................................11 Hypertensive Retinopathy.....................................37 Idiopathic Juxtafoveal Retinal Telangiectasia...........39 CONJUNCTIVA & SCLERA Ocular Ischemic Syndrome...................................40 Scleral Melt ........................................................13 Retinal Artery Occlusion ......................................42 Giant Papillary Conjunctivitis................................14 Conjunctival Lymphoma .......................................15 NEURO-OPHTHALMIC DISEASE Blue Sclera .........................................................17 Dorsal Midbrain Syndrome ..................................45 -
Using the Ophthalmoscope: Viewing the Optic Disc and Retina
Using the Ophthalmoscope: Viewing the Optic Disc and Retina Judith Warner, MD University of Utah THE OPHTHALMOSCOPE DIRECT OPHTHALMOSCOPY • Jan Purkinje 1823 • Hermann von Helmholtz 1851 • Hand held ophthalmoscope • Direct up-right image Dials of the Ophthalmoscope RED-FREE FILTER (GREEN LIGHT) 450 nm monochromatic light nerve fiber layer optic nerve drusen OTHER DIALS • Used for measuring lesion size • Looking for the center of fixation OTHER DIALS: SLIT BEAM The wheel has lenses of power Panoptic-ophthalmoscope Direct type Wider field of view Distance from pt greater Similar apertures Not as easy to carry Slightly dimmer light source Not as magnified view of Disc Clean the rubber cup between patients Photographs: http://panoptic.welchallyn.com/faq.html WHEN EVER POSSIBLE: DILATE THE PATIENT Steps to Direct Ophthalmoscopy • Dimly lit room • Dilating drops • Patient fixates distant target • Align yourself • Red reflex • Dial in HOW TO USE THE DIRECT Ophthalmoscope.avi ophthalmoscope.wmv THE RED REFLEX The layers you will go through to see the optic disc THE OPTIC NERVE WHAT YOU SHOULD OBSERVE IN EVERYONE RIGHT EYE AND LEFT EYE THE NORMAL DISC • The disc is 1.62 mm or 1 million fibers • Central retinal artery and vein • Lamina Cribrosa • The optic cup The Normal Disc Appearance The lamina cribrosa is an important disc structure --Means Sieve --Anatomically present in all discs --Visible in about 1/3 --Shallow in myopia Look at the Cup-to-disc ratio: WHAT IS THE CUP-TO-DISC RATIO? .7 NO CUP 0.1 CUP 0.3 CUP 0.7 CUP 0.9 CUP What is the cup