Multi-Discipline Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Human Multi-Lineage Hepatic Organoid Model for Liver Fibrosis
bioRxiv preprint doi: https://doi.org/10.1101/2020.09.01.278473; this version posted September 2, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. A Human Multi-Lineage Hepatic Organoid Model for Liver Fibrosis Yuan Guan1, Annika Enejder2, Meiyue Wang1, Zhuoqing Fang1, Lu Cui3, Shih-Yu Chen4, Jingxiao Wang1, Yalun Tan1, Manhong Wu1, Xinyu Chen1, Patrik K. Johansson2, Issra Osman1, Koshi Kunimoto3, Pierre Russo5, Sarah C. Heilshorn2 and Gary Peltz1* 1Department of Anesthesia, Stanford University School of Medicine, Stanford CA, 94305; 2Department of Materials Science and Engineering, Stanford University, Stanford CA, 94305; 3Department of Pathology, Institute of Stem Cell Biology and Regenerative Medicine (ISCBRM), Stanford University School of Medicine, Stanford, 94305, CA, USA; 4Shih-Yu Chen, Institute of Biomedical Sciences, Academia Sinica, Taipei, 11529, Taiwan; 5Perelman School of Medicine at The University of Pennsylvania, Philadelphia, PA 19104 The authors have declared that no conflict of interest exists. *Address Correspondence to: [email protected] 300 Pasteur Dr. Room L232 Stanford, CA 94305. bioRxiv preprint doi: https://doi.org/10.1101/2020.09.01.278473; this version posted September 2, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Summary Despite its devastating consequences, liver fibrosis has no treatments. Genome engineering and a hepatic organoid system was used to produce the first in vitro model for human liver fibrosis. Hepatic organoids engineered to express the most common causative mutation for Autosomal Recessive Polycystic Kidney Disease (ARPKD) developed the key features of ARPKD liver pathology (abnormal bile ducts and hepatic fibrosis) in only 21 days. -

Entrectinib (Interim Monograph)
Entrectinib (interim monograph) DRUG NAME: Entrectinib SYNONYM(S): RXDX-1011, NMS-E6282 COMMON TRADE NAME(S): ROZLYTREK® CLASSIFICATION: molecular targeted therapy Special pediatric considerations are noted when applicable, otherwise adult provisions apply. MECHANISM OF ACTION: Entrectinib is an orally administered, small molecule, multi-target tyrosine kinase inhibitor which targets tropomyosin- related kinase (Trk) proteins TrkA, TrkB, and TrkC, proto-oncogene tyrosine-protein kinase ROS (ROS1) and anaplastic lymphoma kinase (ALK). TrkA, TrkB, and TrkC are receptor tyrosine kinases encoded by the neurotrophic tyrosine receptor kinase (NTRK) genes NTRK1, NTRK2, and NTRK3, respectively. Fusion proteins that include Trk, ROS1, or ALK kinase domains drive tumorigenic potential through hyperactivation of downstream signalling pathways leading to unconstrained cell proliferation. By potently inhibiting the Trk kinases, ROS1, and ALK, entrectinib inhibits downstream signalling pathways, cell proliferation and induces tumour cell apoptosis.3-5 PHARMACOKINETICS: Oral Absorption bioavailability = 55%; Tmax = 4-6 hours; Tmax delayed 2 h by high-fat, high-calorie food intake Distribution highly bound to human plasma proteins cross blood brain barrier? yes volume of distribution 551 L (entrectinib); 81.1 L (M5) plasma protein binding >99% (entrectinib and M5) Metabolism primarily metabolized by CYP 3A4 active metabolite(s) M5 inactive metabolite(s) M11 Excretion primarily via hepatic clearance urine 3.06% feces 82.9% (36% as unchanged entrectinib, 22% as M5) terminal half life 20 h (entrectinib); 40 h (M5) clearance 19.6 L/h (entrectinib); 52.4 L/h (M5) Elderly no clinically significant difference Children comparable pharmacokinetics of entrectinib and M5 in adults and children Ethnicity no clinically significant difference Adapted from standard reference3,4 unless specified otherwise. -

07052020 MR ASCO20 Curtain Raiser
Media Release New data at the ASCO20 Virtual Scientific Program reflects Roche’s commitment to accelerating progress in cancer care First clinical data from tiragolumab, Roche’s novel anti-TIGIT cancer immunotherapy, in combination with Tecentriq® (atezolizumab) in patients with PD-L1-positive metastatic non- small cell lung cancer (NSCLC) Updated overall survival data for Alecensa® (alectinib), in people living with anaplastic lymphoma kinase (ALK)-positive metastatic NSCLC Key highlights to be shared on Roche’s ASCO virtual newsroom, 29 May 2020, 08:00 CEST Basel, 7 May 2020 - Roche (SIX: RO, ROG; OTCQX: RHHBY) today announced that new data from clinical trials of 19 approved and investigational medicines across 21 cancer types, will be presented at the ASCO20 Virtual Scientific Program organised by the American Society of Clinical Oncology (ASCO), which will be held 29-31 May, 2020. A total of 120 abstracts that include a Roche medicine will be presented at this year's meeting. "At ASCO, we will present new data from many investigational and approved medicines across our broad oncology portfolio," said Levi Garraway, M.D., Ph.D., Roche's Chief Medical Officer and Head of Global Product Development. “These efforts exemplify our long-standing commitment to improving outcomes for people with cancer, even during these unprecedented times. By integrating our medicines and diagnostics together with advanced insights and novel platforms, Roche is uniquely positioned to deliver the healthcare solutions of the future." Together with its partners, Roche is pioneering a comprehensive approach to cancer care, combining new diagnostics and treatments with innovative, integrated data and access solutions for approved medicines that will both personalise and transform the outcomes of people affected by this deadly disease. -

FLT3 Inhibitors in Acute Myeloid Leukemia Mei Wu1, Chuntuan Li2 and Xiongpeng Zhu2*
Wu et al. Journal of Hematology & Oncology (2018) 11:133 https://doi.org/10.1186/s13045-018-0675-4 REVIEW Open Access FLT3 inhibitors in acute myeloid leukemia Mei Wu1, Chuntuan Li2 and Xiongpeng Zhu2* Abstract FLT3 mutations are one of the most common findings in acute myeloid leukemia (AML). FLT3 inhibitors have been in active clinical development. Midostaurin as the first-in-class FLT3 inhibitor has been approved for treatment of patients with FLT3-mutated AML. In this review, we summarized the preclinical and clinical studies on new FLT3 inhibitors, including sorafenib, lestaurtinib, sunitinib, tandutinib, quizartinib, midostaurin, gilteritinib, crenolanib, cabozantinib, Sel24-B489, G-749, AMG 925, TTT-3002, and FF-10101. New generation FLT3 inhibitors and combination therapies may overcome resistance to first-generation agents. Keywords: FMS-like tyrosine kinase 3 inhibitors, Acute myeloid leukemia, Midostaurin, FLT3 Introduction RAS, MEK, and PI3K/AKT pathways [10], and ultim- Acute myeloid leukemia (AML) remains a highly resist- ately causes suppression of apoptosis and differentiation ant disease to conventional chemotherapy, with a me- of leukemic cells, including dysregulation of leukemic dian survival of only 4 months for relapsed and/or cell proliferation [11]. refractory disease [1]. Molecular profiling by PCR and Multiple FLT3 inhibitors are in clinical trials for treat- next-generation sequencing has revealed a variety of re- ing patients with FLT3/ITD-mutated AML. In this re- current gene mutations [2–4]. New agents are rapidly view, we summarized the preclinical and clinical studies emerging as targeted therapy for high-risk AML [5, 6]. on new FLT3 inhibitors, including sorafenib, lestaurtinib, In 1996, FMS-like tyrosine kinase 3/internal tandem du- sunitinib, tandutinib, quizartinib, midostaurin, gilteriti- plication (FLT3/ITD) was first recognized as a frequently nib, crenolanib, cabozantinib, Sel24-B489, G-749, AMG mutated gene in AML [7]. -
NCCN Guidelines for Myeloid/Lymphoid Neoplasms with Eosinophilia and Tyrosine Kinase Fusion Genes V.2.2021 –Interim on 07/21/20
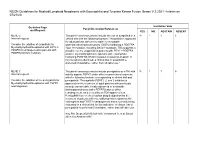
NCCN Guidelines for Myeloid/Lymphoid Neoplasms with Eosinophilia and Tyrosine Kinase Fusion Genes V.2.2021 –Interim on 07/21/20 Guideline Page Institution Vote Panel Discussion/References and Request YES NO ABSTAIN ABSENT MLNE-5 The panel consensus was to include the use of avapritinib in a 18 1 1 6 Internal request: clinical trial with the following footnote: "Avapritinib is approved for adult patients with unresectable or metastatic Consider the addition of avapritinib for gastrointestinal stromal tumors (GISTs) harboring a PDGFRA Myeloid/lymphoid Neoplasms with FIP1L1- exon 18 mutation, including D842V mutations. This suggests a PDGFRA rearrangement in patients with possible role for avapritinib in patients with FIP1L1-PDGFRA– PDGFRA D842V mutation. positive myeloid/lymphoid neoplasms with eosinophilia harboring PDGFRA D842V mutation resistant to imatinib. If this mutation is identified, a clinical trial of avapritinib is preferred (if available), rather than off-label use." MLNE-7 The panel consensus was to include pemigatinib as a TKI with 18 1 1 6 Internal request: activity against FGFR1 under other recommended regimens with the following footnote corresponding to clinical trial and Consider the addition of the pemigatinib for pemigatinib: "Pemigatinib (FGFR1, 2, and 3 inhibitor) is Myeloid/lymphoid Neoplasms with FGFR1 approved for the treatment of adult patients with previously rearrangement. treated, unresectable, locally advanced or metastatic cholangiocarcinoma and a FGFR2 fusion or other rearrangement, as detected by an FDA-approved test. Pemigatinib has received orphan drug designation for the treatment of patients with myeloid/lymphoid neoplasms with eosinophilia and FGFR1 rearrangement and is currently being evaluated in a clinical trial for this indication. -

Leukemia Insights June 2021
JUNE 2021 In this month’s Leukemia Insights newsletter, written by Prithviraj Bose, M.D. and Srdan Verstovsek, M.D., Ph.D., and sponsored in part by the Charif Souki Cancer Research ABOUT MyMDAnderson Fund, we discuss our novel therapeutic approaches for the rare hematologic malignancies, systemic mastocytosis and myeloid/lymphoid neoplasms with myMDAnderson is a secure, eosinophilia. Learn more about our Leukemia program. personalized web site helping community physicians expedite patient referrals, as well as improve continuity Spotlight on rare, atypical, myeloid of care through information access and streamlined communications. neoplasms: systemic mastocytosis and Physicians who have referred patients myeloid/lymphoid neoplasms with to MD Anderson or plan to do so, can utilize the HIPAA compliant features eosinophilia and FGFR1 rearrangements of myMDAnderson to: • Refer a patient • View your patient's appointments Systemic Mastocytosis Access patient reports • Send and receive secure Systemic mastocytosis (SM) is a rare myeloid neoplasm messages driven in approximately 95% of cases by an activating mutation in c-KIT, usually D816V. SM is characterized as indolent, smoldering or advanced, based on the presence JOIN THE COVERSATION and number of so-called B- and C-findings. The latter Connect with us. signify organ damage and are a hallmark of advanced SM (AdvSM). AdvSM, in turn, is typically sub-classified as aggressive SM (ASM), SM with an associated hematologic neoplasm (SM-AHN, the most common subtype) and mast cell leukemia (MCL). Patients with indolent SM (ISM) and smoldering SM (SSM) enjoy much better survival than JOIN OUR MAILING LIST those with AdvSM, although symptoms in all three subtypes can be severe and debilitating. -

CDER Breakthrough Therapy Designation Approvals Data As of December 31, 2020 Total of 190 Approvals
CDER Breakthrough Therapy Designation Approvals Data as of December 31, 2020 Total of 190 Approvals Submission Application Type and Proprietary Approval Use Number Number Name Established Name Applicant Date Treatment of patients with previously BLA 125486 ORIGINAL-1 GAZYVA OBINUTUZUMAB GENENTECH INC 01-Nov-2013 untreated chronic lymphocytic leukemia in combination with chlorambucil Treatment of patients with mantle cell NDA 205552 ORIGINAL-1 IMBRUVICA IBRUTINIB PHARMACYCLICS LLC 13-Nov-2013 lymphoma (MCL) Treatment of chronic hepatitis C NDA 204671 ORIGINAL-1 SOVALDI SOFOSBUVIR GILEAD SCIENCES INC 06-Dec-2013 infection Treatment of cystic fibrosis patients age VERTEX PHARMACEUTICALS NDA 203188 SUPPLEMENT-4 KALYDECO IVACAFTOR 21-Feb-2014 6 years and older who have mutations INC in the CFTR gene Treatment of previously untreated NOVARTIS patients with chronic lymphocytic BLA 125326 SUPPLEMENT-60 ARZERRA OFATUMUMAB PHARMACEUTICALS 17-Apr-2014 leukemia (CLL) for whom fludarabine- CORPORATION based therapy is considered inappropriate Treatment of patients with anaplastic NOVARTIS lymphoma kinase (ALK)-positive NDA 205755 ORIGINAL-1 ZYKADIA CERITINIB 29-Apr-2014 PHARMACEUTICALS CORP metastatic non-small cell lung cancer (NSCLC) who have progressed on or are intolerant to crizotinib Treatment of relapsed chronic lymphocytic leukemia (CLL), in combination with rituximab, in patients NDA 206545 ORIGINAL-1 ZYDELIG IDELALISIB GILEAD SCIENCES INC 23-Jul-2014 for whom rituximab alone would be considered appropriate therapy due to other co-morbidities -

2020 Master Class Course Best Practices and Expanding Treatment Options in Soft Tissue Sarcomas Including GIST George D
2020 Master Class Course Best Practices and Expanding Treatment Options in Soft Tissue Sarcomas including GIST George D. Demetri, MD FACP FASCO 1 George D. Demetri, MD Faculty Disclosure • Scientific consultant with sponsored research to Dana-Farber: Bayer, Pfizer, Novartis, Epizyme, Roche/Genentech, Epizyme, LOXO Oncology, AbbVie, GlaxoSmithKline, Janssen, PharmaMar, Daiichi-Sankyo, AdaptImmune • Scientific consultant: GlaxoSmithKline, EMD-Serono, Sanofi, ICON plc, MEDSCAPE, Mirati, WCG/Arsenal Capital, Polaris, MJ Hennessey/OncLive, C4 Therapeutics, Synlogic, McCann Health • Consultant/SAB member with minor equity holding: G1 Therapeutics, Caris Life Sciences, Erasca Pharmaceuticals, RELAY Therapeutics, Bessor Pharmaceuticals, Champions Biotechnology, Caprion/HistoGeneX • Board of Directors member and Scientific Advisory Board Consultant with minor equity holding: Blueprint Medicines, Translate BIO • Patents/Royalties: Novartis royalty to Dana-Farber for use patent of imatinib in GIST • Non-Financial Interests: AACR Science Policy and Government Affairs Committee Chair, Alexandria Real Estate Equities, Faculty of this CE activity may include discussions of products or devices that are not currently labeled for use by the FDA. The faculty have been informed of their responsibility to disclose to the audience if they will be discussing off label or investigational uses (any uses not approved by the FDA) of products or devices. 2 Soft Tissue Sarcomas: Approximate Anatomic Distribution Head and Neck 10% Upper extremities 15% Trunk 10% Retroperitoneal, pelvic and visceral Lower extremities 15% 50% (includes GIST and GYN sarcomas) Modified from Clark MA et al. NEJM 2005;353:701-11 3 Sarcomas represent an exceedingly diverse set of diseases Bone Sarcomas 10% GIST Un- differentiated Liposarcomas Leiomyo- Sarcomas 4 Ducimetiere et al. -

Precision Medicine in Pediatric Neurooncology: a Review
UCLA UCLA Previously Published Works Title Precision Medicine in Pediatric Neurooncology: A Review. Permalink https://escholarship.org/uc/item/6tv2b43d Journal ACS chemical neuroscience, 9(1) ISSN 1948-7193 Authors Mochizuki, Aaron Y Frost, Isaura M Mastrodimos, Melina B et al. Publication Date 2018 DOI 10.1021/acschemneuro.7b00388 Peer reviewed eScholarship.org Powered by the California Digital Library University of California HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author ACS Chem Manuscript Author Neurosci. Author Manuscript Author manuscript; available in PMC 2019 July 24. Published in final edited form as: ACS Chem Neurosci. 2018 January 17; 9(1): 11–28. doi:10.1021/acschemneuro.7b00388. Precision Medicine in Pediatric Neurooncology: A Review Aaron Y. Mochizuki∥, Isaura M. Frost∥, Melina B. Mastrodimos∥, Ashley S. Plant┴, Anthony C. Wang#, Theodore B. Moore∥, Robert M. Prins#,∇,○, Paul S. Weiss*,†,‡,§,∇, Steven J. Jonas*,†,∥,◆,¶ †California NanoSystems Institute, University of California, Los Angeles, Los Angeles, California 90095, United States ‡Department of Chemistry and Biochemistry, University of California, Los Angeles, Los Angeles, California 90095, United States §Department of Materials Science and Engineering, University of California, Los Angeles, Los Angeles, California 90095, United States ∥Department of Pediatrics, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, California 90095, United States ┴Division of Pediatric Oncology, Children’s Hospital of Orange -

Patent Application Publication ( 10 ) Pub . No . : US 2019 / 0192440 A1
US 20190192440A1 (19 ) United States (12 ) Patent Application Publication ( 10) Pub . No. : US 2019 /0192440 A1 LI (43 ) Pub . Date : Jun . 27 , 2019 ( 54 ) ORAL DRUG DOSAGE FORM COMPRISING Publication Classification DRUG IN THE FORM OF NANOPARTICLES (51 ) Int . CI. A61K 9 / 20 (2006 .01 ) ( 71 ) Applicant: Triastek , Inc. , Nanjing ( CN ) A61K 9 /00 ( 2006 . 01) A61K 31/ 192 ( 2006 .01 ) (72 ) Inventor : Xiaoling LI , Dublin , CA (US ) A61K 9 / 24 ( 2006 .01 ) ( 52 ) U . S . CI. ( 21 ) Appl. No. : 16 /289 ,499 CPC . .. .. A61K 9 /2031 (2013 . 01 ) ; A61K 9 /0065 ( 22 ) Filed : Feb . 28 , 2019 (2013 .01 ) ; A61K 9 / 209 ( 2013 .01 ) ; A61K 9 /2027 ( 2013 .01 ) ; A61K 31/ 192 ( 2013. 01 ) ; Related U . S . Application Data A61K 9 /2072 ( 2013 .01 ) (63 ) Continuation of application No. 16 /028 ,305 , filed on Jul. 5 , 2018 , now Pat . No . 10 , 258 ,575 , which is a (57 ) ABSTRACT continuation of application No . 15 / 173 ,596 , filed on The present disclosure provides a stable solid pharmaceuti Jun . 3 , 2016 . cal dosage form for oral administration . The dosage form (60 ) Provisional application No . 62 /313 ,092 , filed on Mar. includes a substrate that forms at least one compartment and 24 , 2016 , provisional application No . 62 / 296 , 087 , a drug content loaded into the compartment. The dosage filed on Feb . 17 , 2016 , provisional application No . form is so designed that the active pharmaceutical ingredient 62 / 170, 645 , filed on Jun . 3 , 2015 . of the drug content is released in a controlled manner. Patent Application Publication Jun . 27 , 2019 Sheet 1 of 20 US 2019 /0192440 A1 FIG . -

PIONEER: a Randomized, Double-Blind, Placebo-Controlled, Phase 2 Study of Avapritinib in Patients with Indolent Or Smoldering Sy
PIONEER: A Randomized, Double-Blind, Placebo-Controlled, Phase 2 Study of Avapritinib in Patients with Indolent or Smoldering Systemic Mastocytosis with Symptoms Inadequately Controlled with Standard Therapy Cem Akin, Hanneke Oude Elberink, Jason Gotlib, Vito Sabato, Karin Hartmann, Sigurd Broesby-Olsen, Mariana Castells, Michael W. Deininger, Mark L. Heaney, Tracy I. George, Deepti Radia, Massimo Triggiani, Paul van Daele, Daniel J. DeAngelo, Oleg Schmidt-Kittler, Hui-Min Lin, Andrew Morrison, Brenton Mar, Frank Siebenhaar, Marcus Maurer American Academy of Allergy Asthma and Immunology Annual Meeting March 16, 2020 Disclosures • Investigator: Blueprint Medicines’ ongoing Phase 2 PIONEER trial in indolent and smoldering systemic mastocytosis • Consultant: Blueprint Medicines, Novartis • AYVAKIT™ (avapritinib) is approved by the FDA for the treatment of adults with unresectable or metastatic gastrointestinal stromal tumor (GIST) harboring a platelet-derived growth factor receptor alpha (PDGFRA) exon 18 mutation, including PDGFRA D842V mutations, in the United States. Avapritinib has not been approved by the FDA or any other health authority for use in the United States for any other indication or in any other jurisdiction for any indication. • All data in this presentation are based on a cut-off date of December 27, 2019 unless otherwise specified. 2 Systemic mastocytosis (SM) is a clonal mast cell (MC) neoplasm driven by KIT D816V SM Prevalence of ~1:10,000 ~32,000 estimated in US KIT D816V ~5% Advanced SM Organ damage and decreased survival -

Crenolanib Is a Selective Type I Pan-FLT3 Inhibitor
Crenolanib is a selective type I pan-FLT3 inhibitor Catherine Choy Smitha,b,1, Elisabeth A. Lasatera,1, Kimberly C. Lina, Qi Wangc, Melissa Quino McCreeryd, Whitney K. Stewarta, Lauren E. Damona, Alexander E. Perle, Grace R. Jeschkee, Mayumi Sugitae, Martin Carrolle, Scott C. Koganb,d, John Kuriyanc, and Neil P. Shaha,b,2 aDivision of Hematology/Oncology, bHelen Diller Family Comprehensive Cancer Center, and dDivision of Laboratory Medicine, University of California, San Francisco, CA 94143; cDepartment of Molecular and Cell Biology, University of California, Berkeley, CA 94720; and eDivision of Hematology/Oncology, Perelman School of Medicine and the Abramson Cancer Center, University of Pennsylvania, Philadelphia, PA 19104 Edited* by Charles L. Sawyers, Memorial Sloan–Kettering Cancer Center, New York, NY, and approved February 13, 2014 (received for review November 4, 2013) Tyrosine kinase inhibitors (TKIs) represent transformative thera- inhibitor and holds significant promise for achieving prolonged pies for several malignancies. Two critical features necessary for remissions. However, ponatinib potently inhibits a number of maximizing TKI tolerability and response duration are kinase selec- kinases, which may be responsible for unanticipated serious tivity and invulnerability to resistance-conferring kinase domain (KD) cardiovascular toxicities that have emerged with this agent. mutations in the intended target. No prior TKI has demonstrated The ability to selectively suppress resistance-conferring muta- both of these properties.