The Framework Convention on Tobacco Control: the Politics of Global Health Governance
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Big Tob Acco's Tricks
BIG TOBACCO'S TRICKS E-cigarette companies target youth with kid-friendly marketing. Researchers at Stanford University concluded that JUUL's marketing launch was "patently youth-oriented" and closely resembled the themes and tactics that the tobacco industry had successfully used for decades. JUUL hired social media influencers to promote JUUL and attend its launch events, amplifying the reach of JUUL's marketing on social media. JUUL's launch included a series of at least 50 highly stylized parties in cities across America. Thousands of young people were given free JUULs, often given out by attractive young girls. E-cigarette companies flood social media with youth-targeted marketing, often using influencers and celebrities and utilizing hashtags to spread their reach. E-cigarettes are easy for kids to get. Retailers are significantly less likely to card underage youth for purchase attempts of e-cigarettes than cigarettes. A California study found that tobacco and vape shops have the highest rates of sales to minors, with 45% selling to underage buyers. Studies have found that youth can succesfully purchase e-cigarettes over the internet in 94-97% of online purchase attempts. E-cigarettes companies have manipulated their products to make them more addictive. JUUL and other e-cigarette companies use "nicotine salts," which allow them to deliver high doses of nicotine with the irritation of other tobacco products. Each JUUL pod can contain as much nicotine as a pack of 20 cigarettes. www.TakeDownTobacco.org BIG TOBACCO'S TRICKS The tobacco industry spends $9.1 billion a year to market cigarettes and smokeless tobacco products in the U.S. -

Chapter 14. Tobacco Companies.Pdf
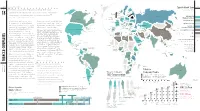
Imperial British American LEADING TOBACCO MANUFACTURER CHAPTER Tobacco Tobacco: London, UK By country, 2006 TOBACCO COMPANIES Group: Bristol, UK Imperial Tobacco/ “In the tobacco business, big is beautiful.” SWEDEN FINLAND Altria/Philip Morris None NORWAY Altadis 14 ESTONIA —RONALD WILDMANN, AN ANALYST AT ZURICH’S BANK LEU AG, British American State Monopoly No data ON THE ROTHMANS/BAT MERGER, 1999 UNITED DENMARK LATVIA KINGDOM LITHUANIA Tobacco Location of NETHERLANDS RUSSIAN FED. BELARUS Japan Tobacco Other headquarters of IRELAND POLAND International/Gallaher GERMANY major transnational BELGIUM tobacco companies Philip Morris CZECH REP. UKRAINE SLOVAKIA n recent years, dozens of cigarette manufacturing International: AUSTRIA SWITZ. REP. RUSSIAN HUNGARY MOLDOVA Lausanne, SLOVENIA FEDERATION companies have consolidated under four major private CANADA Switzerland FRANCE CROATIA ROMANIA BOSNIA AND HERZEGOVINA corporations: Altria/Philip Morris, British American SERBIA ITALY BULGARIA I Altadis: MONTENEGRO Tobacco, Japan Tobacco International, and Imperial Tobacco. FYR MACEDONIA Madrid, Spain ALBANIA State monopolies are also major cigarette manufacturers. The PORTUGAL SPAIN GREECE KAZAKHSTAN largest state monopoly is China National Tobacco Corporation, with a global cigarette market share that exceeds that of any UZBEKISTAN Altria: Richmond, GEORGIA KYRGYZSTAN private company. Because the European Union intends to AZERBAIJAN DPR UNITED STATES OF AMERICA Virginia, USA TURKEY TURKMENISTAN KOREA ARMENIA JAPAN Japan Tobacco restrict further mergers and acquisitions that increase a tobacco SYRIAN REP. MALTA KOREA International: CYPRUS ARAB CHINA TUNISIA LEBANON REP. IRAQ ISL. REP. Tokyo, Japan company’s market-share dominance, industry consolidation MOROCCO ISRAEL JORDAN OF IRAN trends may have peaked. NEPAL LIBYAN PAKISTAN The tobacco industry includes some of the most powerful ALGERIA ARAB KUWAIT JAMAHIRIYA EGYPT MEXICO UAE transnational corporate entities in the world. -
Big Tobacco, Big Avoidance Report 2020 1
Big Tobacco, Big Avoidance report 2020 1 Big Tobacco, Big Avoidance An analysis of the main tax avoidance structures used by British American Tobacco, Imperial Brands, Japan Tobacco International and Philip Morris International, based on annual reports of parent companies and major subsidiaries in 2010-2019 4 November 2020 A cooperative of highly specialized investigative journalists The Investigative Desk is a cooperative of highly specialised investigative journalists Office: Gaasterlandstraat 5, 1079 RH Amsterdam, the Netherlands +31 6 54674124 / www.investigativedesk.com / [email protected] Big Tobacco, Big Avoidance report 2020 2 Authors: Stefan Vermeulen (TheID) Manon Dillen (TheID) Co-author: Dr. J Robert Branston, Senior Lecturer (Associate Professor) in Business Economics School of Management, University of Bath, UK Researchers: Sergio Nieto Solis (TheID) Nadia el Khannoussi (TheID) Editor-in-chief and supervisor: Dr. Marcel Metze (TheID) The Investigative Desk is a cooperative of highly specialised investigative journalists Office: Gaasterlandstraat 5, 1079 RH Amsterdam, the Netherlands +31 6 54674124 / www.investigativedesk.com / [email protected] Big Tobacco, Big Avoidance report 2020 3 Summary of key findings There is growing pressure worldwide for companies to pay their fair share of tax. One sector that has lucrative revenue and profits is the tobacco industry (see chart). Although the sector makes billions in revenue, it pays relatively little in corporate taxes. Tobacco’s Big Four transnational companies - British American Tobacco, Imperial Brands, Japan Tobacco and Philip Morris - make extensive use of the entire range of common tax avoidance methods. We did not find any clear evidence of illegal practices (tax evasion), but analysis of their annual reports and those of a number of crucial subsidiaries in the period 2010-2019 shows that all four have ‘aggressive tax planning’ strategies, in spite of their own codes of conduct suggesting otherwise. -

The Tobacco Industry & the Black Community: the Targeting Of
TOBACCO June 2021 INDUSTRY THE TOBACCO INDUSTRY & THE BLACK COMMUNITY The Targeting of African Americans Big Tobacco, including more recent players like Juul Labs, has a sordid and lengthy history of targeting and exploiting Black, Indigenous, and other historically marginalized racial and ethnic groups, youth, the LGBTQ+ community, women, and others for corporate gain. The tobacco industry does this through sophisticated marketing tactics to lure new consumers to its deadly products and keep them hooked. An additional, lesser known tactic, one that the industry uses to whitewash its This factsheet is intended to raise awareness reputation, safeguard its regulatory influence of this form of the industry’s manipulation and power, manipulate messaging, and gain and abuse of targeted, at-risk populations. It public support is to make hefty contributions to describes the tobacco industry’s use of front culturally-relevant organizations, newspapers, groups, distortion, and corporate giving to mask magazines, and events of targeted communities. disreputable corporate conduct and highlights The tobacco industry is notorious for making recent examples of the way the industry exploits corporate donations to numerous organizations the African American community to maintain and causes championed by the very populations political access and shape policies that serve its it preys upon for profit. corporate interests. www.publichealthlawcenter.org June 2021 Corporate Malfeasance Since their inception, tobacco companies have used their vast resources -
Tobacco Companies: Philip Morris Without Some of the Risks of Smoking
56 RESEARCH Says: Cigarette Market Share 57 Chapter These companies remain some of the most Sweden Finland by country, 2008 Norway . This is thanks in part to their endless British Estonia “profitable in the world American Russian United Kingdom Tobacco Latvia Fed. 18 London, inventive ways of undermining and circumventing regulation. Lithuania Denmark Russian Federation Ireland Philip Morris USA/ Anna Gilmore, University of Bath, UK, 2011 Netherlands Belarus Philip Morris International ” Canada Poland Imperial Tobacco Group Germany Bristol, UK Belgium n recent years, publicly traded tobacco Nicoventures, a separate company dedicated to Czech Rep. Ukraine British American Tobacco Philip Morris International Slovakia Rep. Lausanne, Switzerland Austria Moldova I companies have consolidated through creating alternative nicotine products that offer Switz. Hungary Slovenia— France —Croatia Romania Imperial Tobacco Group privatization and mergers. Today there are five the same experience expected from cigarettes Bosnia & Herzegovina Serbia Kazakhstan Japan Tobacco/ major private tobacco companies: Philip Morris without some of the risks of smoking. Bulgaria Albania —FYR Japan Japan Tobacco International Philip Morris International Italy Macedonia DPR Portugal Uzbekistan China National International, Altria/Philip Morris USA, Japan New York, NY Spain Georgia Kyrgyzstan Korea United States of America Greece Tobacco Corporation Korea Estimates of revenues from the global tobacco Armenia— —Azerbaijan Beijing State-Owned Tobacco Company Turkmenistan Rep Tobacco International, British American Altria Group/Philip Morris USA Turkey industry vary widely but are likely approaching Richmond, VA —Malta Syrian Tobacco, and Imperial Tobacco. In addition to Tunisia Cyprus— China Japan Tobacco/ Other Arab Rep. Japan Tobacco International half a trillion dollars annually. Although Lebanon*— Isl. -
Addiction at Any Cost: Philip Morris International Uncovered Chapter One Chapter
ADDICTION AT ANY COST Philip Morris International Uncovered ADDICTION AT ANY COST Philip Morris International Uncovered Acknowledgements & Contributions We acknowledge the support of Bloomberg Philanthropies Stopping Tobacco Organizations and Products project funding (www.bloomberg.org). The following researchers from the University of Bath authored each of the report chapters: Chapter 1 – Mateusz Zatonski, Silvy Peeters, Anna Gilmore Chapter 2 – Britta K Matthes, Rosemary Hiscock, Karen Evans-Reeves Chapter 3 – Karen Evans-Reeves, Kathrin Lauber (contributions from Janet Hoek, Lindsay Robertson and Debby Sy) Chapter 4 – Tess Legg with input from Anna Gilmore Chapter 5 – Tess Legg with input from Anna Gilmore Karen Evans-Reeves acted as lead author and editor of the report. Anna Gilmore provided substantive edits for each chapter. The authors would like to thank STOP Partners – the Global Center for Good Governance on Tobacco Control, Vital Strategies & The International Union Against Tuberculosis and Lung Disease (The Union) – for feedback on a draft of the report, Union subgrantees for providing information on combustible cigarette marketing and Lindsay Robertson for editorial assistance. Vital Strategies were responsible for the production design and publishing of the report and a corresponding website. Contents Executive Summary Glossary of Terms 10 Chapter 1 The Tobacco Industry and Harm Reduction: A History of Deception 22 Chapter 2 Global Tobacco and Next Generation Product Market, and Philip Morris International 30 Chapter 3 Philip -

The Tobacco Industry Documents What They Are, What They Tell Us, and How to Search Them
THE TOBACCO INDUSTRY DOCUMENTS WHAT THEY ARE, WHAT THEY TELL US, AND HOW TO SEARCH THEM A PRACTICAL MANUAL The WHO Tobacco Free Initiative would like to thank Dr Norbert Hirschhorn for the preparation of this document. F O R E W O R D THE TOBACCO INDUSTRY DOCUMENTS:WHAT THEY ARE, WHAT THEY TELL US, AND HOW TO SEARCH THEM 04 In 1998, six million once secret documents from seven cigarette manufacturers doing business in the US became available to the public as a result of legal action. There were documents from 7 cigarette manufacturers and two affiliated organizations: Philip Morris Incorporated, R.J. Reynolds Tobacco Company, Brown & Williamson Tobacco Corporation, British American Tobacco Industries, Lorillard Tobacco Company, the American Tobacco Company, the Liggett Group, the Tobacco Institute and the Council for Tobacco Research. The documents that include letters, fax, memos, etc written by company scientist, consultants, lawyers, top executives, other employees and outside organizations amounted to over 35 million pages. In 2002, the WHO Regional Office for the Eastern Mediterranean published the first edition of The tobacco industry documents: what they are, what they tell us, and how to search them. A practical manual. The aim was to help journalists, public health professionals and advocates, government officials and the public to search these documents and thereby expand their use outside academia. Recognizing the value of the information contained in these internal industry document archives, while also acknowledging its limitations, the WHO Tobacco Free Initiative decided to publish a second edition of the manual. The information provided in these documents, as well as the reports that have been prepared describing their content, provide a wealth of information about some of the plans and processes of the tobacco companies in their attempt to delay or obstruct tobacco control measures and policies. -

Tobacco Industry Paradise
300 Tobacco Control 2001;10:300–303 Tob Control: first published as 10.1136/tc.10.4.300 on 1 December 2001. Downloaded from COVER ESSAY Germany: tobacco industry paradise Martina Poetschke-Langer, Susanne Schunk Arriving in Germany, visitors are immediately As the examples in this paper demonstrate, confronted with the social acceptability of the voluntary agreements on tobacco advertis- smoking. Even in the international airport at ing are largely ignored. For example, West Frankfurt, one of the first German airports to advertising showing the body builder (fig 1) ban smoking, authorities re-established might not show a woman under 30, but it “restricted” but open smoking areas, so that shows intense physical activity. West has passengers are continuously exposed to various billboard advertisements with refer- environmental tobacco smoke. On most ence to sports—for example, people on German trains, visitors will find bistros with bicycles and holding the Olympic torch (see crowds of smokers. Although smoking in pub- cover). Nil targets an intellectual audience and lic is not allowed for people aged under 16 advertises with prominent smoking actors and years, nobody pays attention to the film makers, the ads making statements such as restriction—typically, parents do not interfere “imprisoned but happy”. Advertising for when their children smoke as many parents are “light”, “mild” and “ultra” cigarettes is as smokers themselves. Like Japan, Germany has common as advertising for regular cigarettes vending machines on almost every corner. despite a voluntary agreement of restricted use With 80 million inhabitants, Germany has of those terms. more than 800 000 vending machines, one Because of the voluntary agreements, in machine for every 30 smokers with free access 1999, Philip Morris and Reemtsma were for adults and children day and night. -

Why Cannabis Is Part of the Future of Big Tobacco
8/2/2021 Why Cannabis Is Part Of The Future Of Big Tobacco EDITORS' PICK | Aug 2, 2021, 07:00am EDT | 1,349 views Why Cannabis Is Part Of The Future Of Big Tobacco Dario Sabaghi Contributor Follow Vices I cover the cannabis industry with a focus on Europe. Listen to this article now -04:40 Powered by Trinity Audio 2 Get unlimited access to the most tru https://www.forbes.com/sites/dariosabaghi/2021/08/02/cannabis-is-part-of-the-future-of-big-tobacco/?sh=29710c4571ed 1/5 8/2/2021 Why Cannabis Is Part Of The Future Of Big Tobacco Hand holding burning joint and smoke in form of marijuana leaf. GETTY When Philip Morris International (PMI) CEO Jacek Olczak told The Mail on Sunday that the UK government should treat cigarettes like petrol cars and ban them in 10 years, many wondered why the world’s biggest tobacco company would self-sabotage itself with such a draconian statement. However, a few days later, the British American Tobacco (BAT) executive Kingsley Wheaton told BBC Radio 4's Today program that cannabis and its derivates are part of the company’s future. "I think [CBD vaping] is part of the future, but the present challenge is reduced harm in tobacco and nicotine alternatives, encouraging people to switch," he said. Both statements from the top world’s biggest tobacco companies reveal an ongoing business model shift of Big Tobacco. Also, they reveal a reaction to consumer trends. By taking into consideration the health impact of their products, tobacco companies are trying to show their efforts to get away from traditional tobacco cigarettes. -

Big Tobacco, E Cigarettes and the Future of Nicotine Delivery
Addicting the Next Generation: Big Tobacco, E Cigarettes and the Future of Nicotine Delivery Senator David Carlucci 1 Introduction This report studies the emergence of the e-cigarette market. Specifically, it shows that although young people are smoking less, they are picking up e-cigarettes at an alarming rate. The tobacco industry is investing heavily in this emerging market, hoping to get a new generation of young people addicted to their products. Young people are a vital segment of the tobacco industry’s market. An astounding 98% of people who smoke tried their first cigarette by age 26. Eighty- nine percent tried their first by 18.’ Studies show that young people who try e-cigarettes are more likely to smoke traditional cigarettes. In order to avoid a new generation becoming addicted to nicotine, this report outlines several legislative solutions. History of Big Tobacco’s Big Fraud The devastating health effects of smoking have long been clear. Smoking causes death and disease. Yet, the tobacco industry ran a campaign of deception for decades to obfuscate this central truth. The first studies to find a correlation between smoking and health issues occurred in the I 930s and 40s. These early studies had little effect on the rates of smoking because the public largely did not have access to these studies and the studies themselves only showed a correlation between smoking and cancer. They had not yet found causation. But a Reader’s Digest article in 1952 seemed to change all that. Entitled “Cancer by the Carton,” this article documented for the general public for the first time in detail the dangers of smoking. -
Case 1:20-Cv-00896 Document 5 Filed 04/01/20 USDC Colorado Page 1 of 207
Case 1:20-cv-00896 Document 5 Filed 04/01/20 USDC Colorado Page 1 of 207 IN THE UNITED STATES DISTRICT COURT FOR THE DISTRICT OF COLORADO Civil Action No. CITY AND COUNTY OF DENVER, Plaintiff, v. JUUL LABS, INC. F/K/A PAX LABS, INC.; EONSMOKE LLC; ALTRIA GROUP, INC.; ALTRIA CLIENT SERVICES LLC; ALTRIA GROUP DISTRIBUTION COMPANY; NU MARK LLC; AND NU MARK INNOVATIONS, LTD.; Defendants. COMPLAINT Case 1:20-cv-00896 Document 5 Filed 04/01/20 USDC Colorado Page 2 of 207 TABLE OF CONTENTS I. INTRODUCTION ........................................................................................................ 1 II. JURISDICTION AND VENUE.................................................................................... 6 III. PARTIES ..................................................................................................................... 7 IV. ALLEGATIONS OF FACT........................................................................................ 10 A. JUUL: Runaway Commercial Success and Public Health Disaster .................. 10 1. Redesigning “the most successful consumer product of all time” ................................................................................................... 10 2. Following Big Tobacco’s footsteps: Nicotine Salts .............................. 16 JLI designed JUUL products to contain and deliver as much nicotine as possible .................................................................... 22 B. Following Big Tobacco’s Playbook, JLI Launched JUUL with a Blatantly Youth-Oriented Campaign -

The Future of Tobacco Stocks: a Scenario Analysis
5)&'6563&0'50#"$$0450$,4 "TDFOBSJPBOBMZTJT +VMZ The Future of Tobacco Stocks: A Scenario Analysis Acknowledgements This document was prepared for Tobacco Free Portfolios, a non-governmental organisation encouraging tobacco-free investment. Research for and preparation of the document was carried out by Professor Rob Bauer and his team of research assistants from Maastricht University School of Business and Economics. Rob Bauer is Professor of Finance (Institutional Investors Chair) and Director of the European Centre for Corporate Engagement (ECCE) at Maastricht University, and Executive Director of the International Centre for Pension Management (ICPM) in Toronto, Canada. His team of research assistants comprises students from the Maastricht University Honours Programme in the second and third years of their bachelor studies: Fabian Grohmann (BSc in International Business, 2nd year), Fabian Süßmann (BSc in International Business, 3rd year), Filip Dobrzynski (BSc in Economics and Business Economics, 3rd year), Jeroen Schmitz (BSc in International Business, 3rd year), Julian Alves (BSc in Economics and Business Economics, 2nd year) and Moritz Dillmann (BSc in Economics and Business Economics, 2nd year). Special thanks go to Jeroen Derwall, Assistant Professor of Finance at Maastricht University, for providing additional guidance and expertise in the process of creating and developing the valuation tool and sensitivity analyses. This process was further facilitated by the work of Tim Koller, Marc Goedhart and David Wessels from McKinsey & Company, whose guide to corporate valuation provided the foundations of our valuation tool. We would also like to thank Arabesque Asset Management for having access to its S-Ray tool and data regarding Tobacco firms.