Caesarean Section Rates at the Standerton Hospital
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Proposed Main Seat / Sub District Within the Proposed Magisterial District Ermelo Main Seat of Msukaligwa Magisterial District
# # !C # # ### !C^ !.C# # # # !C # # # # # # # # # # ^!C # # # # # # # ^ # # ^ # # !C # ## # # # # # # # # # # # # # # # # !C# # !C # # # # # # # # # #!C # # # # # # #!C# # # # # # !C ^ # # # # # # # # # # # # ^ # # # # !C # !C # #^ # # # # # # ## # #!C # # # # # # ## !C# # # # # # # !C# ## # # # # # !C # # !C# # # # #^ # # # # # # # ## # # # # # !C # # # # ## # # # # # # ## # ## #!C # # # # # # # # # # !C # # # ## # # ## # # # # # # !C # # # ##!C ## ## ## # # # # # # # # # #^ # # ## # # # !C # # !C# # # # # # # # # # # # # # # # # # # # # # # # # # #!C # ## # ##^ # !C #!C## # # # # # # # # # # # # # ## # ## # # # !C# ^ ## # # # # # # # # # # # # # # # # # # # # # # ## # # # # # # !C # #!C # # #!C # # !C## # # # # # # !C# # # # # # # # # # ## # # # ## # ## ## # # # # # # # ## # # # # # # # # # # # # # # # # # # # # # ## # # #!C # # # ## # # # # # # # # # # ^!C # # # # # ^ # # # # # # ## # # # # # # # ## # # # # # # #!C # # !C # # !C ## # # # # #!C # # # !C# # # # # # # # # # # # # ## # # # !C# # ## # ## # # ## # # # # # # # # # # # # # # !C # # # # # # # ### #!C# # # !C !C# # !C # ## # # # # # # # # !C# # !.# # # # ## ## # #!C# # # # # # # # ## # # # # # # # # # # # # ### ##^ # # # # # # # ## # # # # ^ # !C# ## # # # # # # !C## # ## # # # # ## # # # # # ## # # # # #!C## !C# # !C# ## # !C### # # ^ # # # !C ### # # # !C# ##!C # !C # # # ^ !C ## # # #!C # ## ## # # ## # # # # # # ## !C# # # # # # # # ## # # # # # !C # ## ## # # # # !C # # ^ # ## # ## # # # !.!C ## # # ## # # # # !C # # !C# # ### # # # # # # # # # # ## !C # # # # ## !C # -

13 Mpumalanga Province
Section B: DistrictProfile MpumalangaHealth Profiles Province 13 Mpumalanga Province Gert Sibande District Municipality (DC30) Overview of the district The Gert Sibande District Municipalitya is a Category C municipality located in the Mpumalanga Province. It is bordered by the Ehlanzeni and Nkangala District Municipalities to the north, KwaZulu-Natal and the Free State to the south, Swaziland to the east, and Gauteng to the west. The district is the largest of the three districts in the province, making up almost half of its geographical area. It is comprised of seven local municipalities: Govan Mbeki, Chief Albert Luthuli, Msukaligwa, Dipaleseng, Mkhondo, Lekwa and Pixley Ka Seme. Highways that pass through Gert Sibande District Municipality include the N11, which goes through to the N2 in KwaZulu-Natal, the N17 from Gauteng passing through to Swaziland, and the N3 from Gauteng to KwaZulu-Natal. Area: 31 841km² Population (2016)b: 1 158 573 Population density (2016): 36.4 persons per km2 Estimated medical scheme coverage: 13.5% Cities/Towns: Amersfoort, Amsterdam, Balfour, Bethal, Breyten, Carolina, Charl Cilliers, Chrissiesmeer, Davel, Ekulindeni, Embalenhle, Empuluzi, Ermelo, Evander, Greylingstad, Grootvlei, Kinross, Leandra, Lothair, Morgenzon, Perdekop, Secunda, Standerton, Trichardt, Volksrust, Wakkerstroom, eManzana, eMkhondo (Piet Retief). Main Economic Sectors: Manufacturing (57.4%), agriculture (41.4%), trade (25.8%), transport (24.5%), finance (21.2%), mining (14.1%), community services (12.3%), construction (2.1%). Population distribution, local municipality boundaries and health facility locations Source: Mid-Year Population Estimates 2016, Stats SA. a The Local Government Handbook South Africa 2017. A complete guide to municipalities in South Africa. Seventh edition. Accessible at: www. -

Greylingstad Mpumalanga Done by Do
Archaeological investigations, done at Bakkiesfontein 568 IR, (Dipaliseng Local Municipality) Greylingstad Mpumalanga Done by Domonique-Marie Verkerk BHSC (Heritage and Cultural Tourism), 2011, UP BA Archaeology, 2012, UP Tel: 012 3333931 E-mail: [email protected] Department of Anthropology and Archaeology, University of Pretoria 5 October 2015 Summary Concentration camps were a tactic created by the British to end the South African War (1899- 1902). Many innocent Boer and African families were sent to these camps where they died of diseases, such as, poor conditions and lack of shelters. Boer families were sent to concentration camps in Heidelberg. Africans, on the other hand, were sent to the concentration camp in Greylingstad. A possible location for the African concentration camp in Greylingstad is Bakkiesfontein 568 IR. Unfortunately, there is nothing to show where this camp is as a fire destroyed many of the records. Bakkiesfontein 568 IR was chosen as a possible location for the African concentration camp in Greylingstad because of the old house, stream, stone walls, railway, SR fort and the African cemetery. Bakkiesfontein was surveyed by foot. The aim was to find the location of the concentration camp. Areas where pedestrian surveys were conducted included the house, barn, possible midden, graves, stone walls and stone circle. The pedestrian survey showed that Iron Age communities also lived on the farm. Three test-pits were also conducted. Areas where the test-pits were conducted included the midden, between stone walls and on a slope near a stone wall. The test-pits were not that successful. The artefacts found during the test- pits and surveys include; metal, ceramic pieces and pottery, glass pieces and even plastic. -

Government Notice No
6 No. 28552 GOVERNMENT GAZETTE, 3 MARCH 2006 GOVERNMENT NOTICES GOEWERMENTSKENNISGEWINGS DEPARTMENT OF ARTS AND CULTURE DEPARTEMENT VAN KUNS EN KULTUUR No. 185 3 March 2006 APPROVAL OF OFFICIAL GEOGRAPHICAL NAMES I, Z, Pallo Jordan, Minister of Arts and Culture officially approved the following geographical names on the advice of the South African Geographical Names Council on 1I November 2005. Dibaba (change of name from A settlement 10 km W of Carolina in Diepgezet) Mpumalanga Ekhandizwe (change of name from A settlement 65 km S of Globlersdal in Louis Creek) Mpumalanga eKulindeni A settlement 20 km S of Badplaas in Mpumalanga eMalahleni (change of name from A town (formerly Witbank) situated 30 Witban k) km E of Middleburg in Mpumalanga eMpuluzi A river 85 km W of Carolina in Mpumalanga eNdlulamithini (change of name from A settlement 6 km W of Standerton in Kaffirskraalkopie) Mpumalanga Engodlomezi (change of name from A mountain 86 km W of Carolina in SYd4 Mpumalanga eNtambende 1 (change of name from A settlement 9 W of Carolina in Devet) Mpumalanga eNtambende 11 (change of name from A settlement 9 W of Carolina in Nordeen) Mpumalanga STAATSKOERANT, 3 MAART 2006 No. 28552 7 eSilobela A township 1 km W of Carolina in Mpumafanga Etikhulungwane (change of name from A settlement 93 km SW of Carolina in Diepdale) Mpumalanga Etikwentsaba Estate A settlement 3 km W of Hazyview in Mpumalanga Ezimbuthumeni (change of name from A settlement 50 km E of Standerton in Kaffirskraal) Mpumalanga Ga-Morwe (change of name from A settlement f 7 km -

Superior Courts Act: Determination of Areas Under Jurisdiction Of
4 No. 42420 GOVERNMENT GAZETTE, 26 APRIL 2019 GOVERNMENT NOTICES • GOEWERMENTSKENNISGEWINGS Justice and Constitutional Development, Department of/ Justisie en Staatkundige Ontwikkeling, Departement van DEPARTMENT OF JUSTICE AND CONSTITUTIONAL DEVELOPMENT NO. 615 26 APRIL 2019 615 Superior Courts Act (10/2013): Determination of Areas under the Jurisdiction of the Mpumalanga Division of the High Court of South Africa 42420 SUPERIOR COURTS ACT, 2013 (ACT NO. 10 OF 2013): DETERMINATION OF AREAS UNDER THE JURISDICTION OF THE MPUMALANGA DIVISION OF THE HIGH COURT OF SOUTH AFRICA I, Tshililo Michael Masutha, Minister of Justice and Correctional Services, acting under section 6(3)(a) and (c) of the Superior Courts Act, 2013 (Act No. 10 of 2013), hereby, after consultation with the Judicial Service Commission, with effect from1 May 2019 - (a) establish a local seat of the Mpumalanga Division of the High Court of South Africa with its seat at the old Magistrate's Court building at the corner of Dr Beyers Naude and OR Tambo streets, Middelburg; and (b) determine the areas under the jurisdiction of the Division as indicated in the accompanying Schedule. of TM MASUTHA, MP (ADV) MINISTER OF JUSTICE AND CORRECTIONAL SERVICES This gazette is also available free online at www.gpwonline.co.za Item DivisionName of Main Seat AreaDivisionunderthejurisdictionSCHEDULEoftheLocal Seat Area of jurisdiction of the local seat Mpumalanga Mbombela Thedistricts following within magisterialthe Mpumalanga districts Province and sub- asMiddelburg districtsThe followingwithin -
Contacts Financial Performance
+ - Lekwa B3 local municipality in Gert Sibande, Mpumalanga Population: 115 661 Size: 4 564.9 km² Density: 25.3 / km² Leaflet | Map data © OpenStreetMap contributors, CC-BY-SA Contacts Last updated October 2020 Mayor/Executive Mayor 017 712 9600 Mr LBR Dhlamini Email municipality 017 712 9634 Main Administration Building Cnr B Naude & M Maiyela Street [email protected] Standerton 2430 Secretary of Mayor/Executive Mayor Ms Precious Nonhlanhla Ngcobo 017 712 9635 [email protected] Municipal Manager Ms G P Mhlongo-Ntshangase 017 712 9613 [email protected] Secretary of Municipal Manager Deputy Mayor/Executive Mayor Secretary of Deputy Mayor/Executive Mayor Chief Financial O{cer Secretary of Financial Manager Mrs I Edwards 017 712 9613 [email protected] Financial Performance Audit Outcomes 2018-2019 2017-2018 2016-2017 2015-2016 Disclaimer of opinion Quali}ed Unquali}ed - Emphasis of Unquali}ed - Emphasis of Matter items Matter items No report available Read report Read report Read report What do dizerent audit outcomes mean? Unquali}ed Opinion Unquali}ed Opinion No Findings Emphasis of Matter Items Same as an Unquali}ed Opinion with no }ndings, but the Same as an Unquali}ed Opinion with no }ndings, but the Auditor-General wants to bring something particular to the Auditor-General wants to bring something particular to the attention of the reader. attention of the reader. Quali}ed Opinion Adverse Opinion The Auditor-General expresses reservations about the fair This is expressed when the auditor concludes that the annual presentation of the }nancial statements. There is some }nancial statements do not present the municipality’s }nancial departure from the Generally Recognised Accounting Practices position, results of operations and cash ~ows in line with (GRAP) but is not su{ciently serious as to warrant an adverse Generally Recognised Accounting Practices (GRAP). -

South African Jewish Board of Deputies Report of The
The South African Jewish Board of Deputies JL 1r REPORT of the Executive Council for the period July 1st, 1933, to April 30th, 1935. To be submitted to the Eleventh Congress at Johannesburg, May 19th and 20th, 1935. <י .H.W.V. 8. Co י É> S . 0 5 Americanist Commiitae LIBRARY 1 South African Jewish Board of Deputies. EXECUTIVE COUNCIL. President : Hirsch Hillman, Johannesburg. Vice-President» : S. Raphaely, Johannesburg. Morris Alexander, K.C., M.P., Cape Town. H. Moss-Morris, Durban. J. Philips, Bloemfontein. Hon. Treasurer: Dr. Max Greenberg. Members of Executive Council: B. Alexander. J. Alexander. J. H. Barnett. Harry Carter, M.P.C. Prof. Dr. S. Herbert Frankel. G. A. Friendly. Dr. H. Gluckman. J. Jackson. H. Katzenellenbogen. The Chief Rabbi, Prof. Dr. j. L. Landau, M.A., Ph.D. ^ C. Lyons. ^ H. H. Morris Esq., K.C. ^י. .B. L. Pencharz A. Schauder. ^ Dr. E. B. Woolff, M.P.C. V 2 CONSTITUENT BODIES. The Board's Constituent Bodies are as. follows :— JOHANNESBURG (Transvaal). 1. Anykster Sick Benefit and Benevolent Society. 2. Agoodas Achim Society. 3. Beth Hamedrash Hagodel. 4. Berea Hebrew Congregation. 5. Bertrams Hebrew Congregation. 6. Braamfontein Hebrew Congregation. 7. Chassidim Congregation. 8. Club of Polish Jews. 9. Doornfontein Hebrew:: Congregation.^;7 10. Eastern Hebrew Benevolent Society. 11. Fordsburg Hebrew Congregation. 12. Grodno Sifck Benefit and Benevolent Society. 13. Habonim. 14. Hatechiya Organisation. 15. H.O.D. Dr. Herzl Lodge. 16. H.O.D. Sir Moses Montefiore Lodge. 17. Jeppes Hebrew Congregation, 18. Johannesburg Jewish Guild. 19. Johannesburg Jewish Helping Hand and Burial Society. -

Presentation to the National Council of Provinces
PRESENTATION TO THE NATIONAL COUNCIL OF PROVINCES PRESENTED BY ACTING EXECUTIVE MAYOR: CLLR.D NHLAPO 29/10/2020 1 PRESENTATION OUTLINE To be a Model City a Centre of Excellence and City Model be a To INTRODUCTION PUBLIC PARTICIPATION SERVICE DELIVERY GOOD GOVERNANCE VISION SOUND FINANCIAL MANAGEMENT BUILDING CAPABLE LOCAL GOVERNMENT CONCLUSION 2 INTRODUCTION Govan Mbeki Local Municipality is situated conglomerates, namely; Leandra (Leslie, in the south-eastern part of Mpumalanga Lebohang and Eendracht) in the western Province, abutting Gauteng Province in the edge, The Greater Secunda (Trichardt, south-west; approximately 150km east of Evander, Kinross and Secunda / Johannesburg and 300km south-west of Embalenhle) conurbation in the central part Nelspruit (capital city of Mpumalanga). and Bethal / Emzinoni in the east. Govan Mbeki Municipality is one of the 7 local municipalities under the jurisdiction of Gert Sibande District (the other districts being Ehlanzeni and Nkangala) and one of the 18 local municipalities within Mpumalanga. The Govan Mbeki area is mainly agricultural / rural with 3 urban 3 INTRODUCTION • Govan Mbeki Municipality is the 4th largest economy in Mpumalanga province and contribution to the provincial economy in 2019 was 12.7% and 47.2% to district economy. The comparative advantage of the municipality is in mining and manufacturing • Govan Mbeki has been identified amongst the struggling municipalities in the province in so far as meeting its service delivery obligations to the satisfaction of the consumers. • Consequently, the municipality has been receiving support from Treasury, Cogta and GSDM. • The municipality continues to operate under difficult conditions as evident in the escalation of the debtors book. -

Government Notice No
STAATSKOERANT, 10 FEBRUARIE 2006 ~0.28458 7 GOVERNMENT NOTICES GOEWERMENTSKENNISGEWINGS DEPARTMENT OF ARTS AND CULTURE DEPARTEMENT VAN KUNS EN KULTUUR No. 113 10 February 2006 APPROVAL OF OFFICIAL PLACE NAMES I, Z, Pallo Jordan, Minister of Arts and Culture officially approved the following place names on the advice of the South African Geographical Names Council on 11 November 2005. Dibaba (change of name from Diepgezet) A settlement IO km W of Carolina in Mpumalanga Ekhandizwe (change of name from Louis A settlement 65 km S of Globlersdal Creek) in Mpumalanga eKulindeni A settlement 20 km S of Badplaas in Mpumalanga eMalahleni (change of name from Witbank) A settlement in Witbank CBD in Mpumalanga Umfazezala (correction of spelling from A river 9 km S of Umdoni uM fazaza na) Municipality in KZN Emfazezala (correction of spelling from A village 9 krn S of Urndoni eMfazazana) municipality in Mpumalanga eMpangeleni (change of name from A settlement in Standerton in Boesmanskraal) Mpumalanga eMpuluzi A river 85 km W of Carolina in Mpumalanga eMthenteni (correction of spelling from A town 9 km N of Hibiscus District elllltentweni) Municipality in KwaZulu-Natal 8 No. 28458 GOVERNMENT GAZETTE, 10 FEBRUARY 2006 eMuziwezinto A town 8 km W of uMdoni (correction of spelling from Emuziwezinto) Municipality in KwaZulu-Natal Umuziwezinto (correction of spelling from A river 8 km W of uMdoni uMuziwezinto) Municipality in KwaZulu-Natal Engodtomezi (change of name from Syde) A mountain 86 km W of Carolina in Mpumalanga eSilobela A township 1 km W of -
Amazon Missions
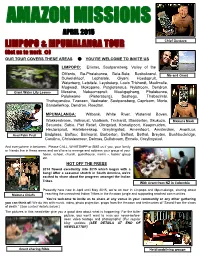
AMAZON MISSIONS APRIL 2015 LIMPOPO & MPUMALANGA TOUR Chief Gustavo (Get us to work ) OUR TOUR COVERS THESE AREAS YOU’RE WELCOME TO INVITE US LIMPOPO: Ellisras, Soutpansberg, Valley of the Olifants, Ba-Phalaborwa, Bela-Bela, Bosbokrand, Me and Grant Duiwelskloof, Lephalale, Giyani, Hoedspruit, Waterberg, Letsitele, Leydsdorp, Louis Trichardt, Modimolle, Mogwadi, Mokopane, Potgietersrus, Nylstroom, Dendron, Giant Water Lily Leaves Messina, Naboomspruit, Mookgophong, Phalaborwa, Polokwane (Pietersburg), Seshego, Thabazimbi, Thohoyandou, Tzaneen, Vaalwater, Soutpansberg, Capricorn, Moria, Bandelierkop, Dendron, Roedtan. MPUMALANGA: Witbank, White River, Waterval Boven, Wakkerstroom, Volksrust, Vaalbank, Trichardt, Standerton, Skukuza, Makuna Mask Secunda, Sabie, Piet Retief, Ohrigstad, Komatipoort, Kaapmuiden, Hectorspruit, Hartebeeskop, Greylingstad, Amersfoort, Amsterdam, Avontuur, Asai Palm Fruit Badplaas, Balfour, Balmoral, Barberton, Belfast, Bethal, Breyten, Bushbuckridge, Carolina, Chrissiesmeer, Delmas, Dullstroom, Ermelo, Greylingstad. And everywhere in between. Please CALL, WHATSAPP or SMS us if you, your family or friends live in these areas and we’d love to arrange and address your group at your home, school, church, guesthouse, men’s -, ladies’ group etc. HOT OFF THE PRESS 2014 flowed excellently into 2015 which began with a bang! After a seasonal stretch in South America, we’re excited to share about the progress amongst the Indian Tribes. With Grant from NZ in Colombia Presently here now in April until May 2015, we’re on tour in Limpopo and Mpumalanga, sharing about reaching the unreached Indian Tribes in the Amazon jungle and supporting reached communities. Makuna Chiefs You’re welcome to invite us to share at any venue in your community or any other gathering you can think of! We do this with music, video, photo projection, props from the Amazon and testimonies of “Saved from the claws of death.” (See contact details below.) The pictures in this newsletter give you a good idea about what is happening. -
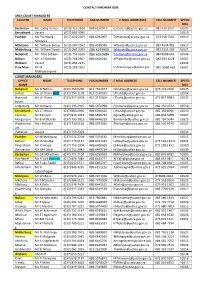
CONTACT INFORMATION AREA COURT MANAGERS CLUSTER NAME TELEPHONE FAX NUMBER E-MAIL ADDRESSES CELL NUMBER SPEED DIAL Barberton
CONTACT INFORMATION AREA COURT MANAGERS CLUSTER NAME TELEPHONE FAX NUMBER E-MAIL ADDRESSES CELL NUMBER SPEED DIAL Barberton Ms. Cathy Venter (013) 712 2104 086 6150972 [email protected] 082 334 2937 16503 Eerstehoek Vacant (017) 883 0090 16510 Evander Ms Thembela (017) 632 2204 086 6292907 [email protected] 073 158 7502 16512 Mcetywa Mdutjana Mr. William Baloyi (013) 947 2363 086 4018346 [email protected] 083 4304 485 16517 Middelburg Mr. William Nyathi (013) 262 2033 086 6293960 [email protected] 083 5355 283 16521 Nelspruit Mr. Titus Letlape (013) 753 6200 086 6292684 [email protected] 084 8388 663 16504 Nsikazi Mr. A Thabethe (013) 793 0567 086 6446010 [email protected] 082 933 3228 16527 Witbank Vacant (013) 656 2221 16534 Prov Man Mr IR (013) 283 7501 [email protected] 082 9568 663 16551 Mohlamonyane COURT MANAGERS OFFICE NAME TELEPHONE FAX NUMBER E MAIL ADDRESS CELL NUMBER SPEED NAME DIAL Nelspruit Ms N Ndlovu (013) 753 6299 013 7554077 [email protected] 076 271 2920 16525 Belfast Ms LP Thaha (Act) (013) 253 1138 013 2530035 [email protected] 16504 Waterval Ms LP Thaha (013) 257 0004 013 2570004 [email protected] 072 833 8983 16533 Boven Lydenburg Mr Chiloane (013) 235 2325 086 5070998 [email protected] 082 256 4722 16518 Eerstehoek Ms LT Mtuta (017) 883 0090 086 6046420 [email protected] 082 359 8096 16510 Carolina Mr DA Gule (017) 843 1033 086 5699732 [email protected] 082 844 5008 16507 Morgenzon Mr B Mahlambi (017) 793 3013 086 6446329 [email protected] -

Important Bird & Biodiversity Areas
CONSERVING IBAS BirdLife South Africa conserves IBAs by prioritising sites for conservation action, obtaining formal protection, developing IBAS OF MPUMALANGA Important Bird & management plans for IBAs and biomes, defending priority Approx. Protection Qualifying sites that are under threat and implementing monitoring pro- Name IBA No. size (ha) status criteria Biodiversity Areas grammes. Volunteer based Local Conservation Groups (LCGs) sup- port these projects by surveying IBAs, implementing conservation Misty Mountain Natural SA013 70 Fully C1 Heritage Site of action and educating the local youth about birds and habitats. BirdLife South Africa works with bird clubs, landowners and other Kaapsehoop SA014 770 Fully A1, A2, A3 MPUMALANGA organisations across Mpumalanga to establish LCGs. Loskop Dam Nature SA015 23 340 Fully C1, C4i Biodiversity Stewardship is a national programme that engages Reserve private and communal landowners to assist them to formally de- Steenkampsberg SA016 196 250 Partial A1, A2, A3, A4i, ii clare their high biodiversity value lands as legally protected areas, and to improve the management of these lands for supporting Songimvelo Nature SA017 46 540 Fully A1, A2, A3 Reserve livelihoods and biodiversity conservation. The Regional Conserva- tion Manager is working with partners to implement stewardship Amersfoort–Bethal– SA018 343 320 None A1, A2, A3, Carolina A4i, ii work aimed at formally proclaiming priority IBAs as protected areas. BirdLife South Africa comments on proposed developments Chrissie Pans SA019 111