Saturated Fats and Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Blood Fats Explained
Blood Fats Explained HEART UK – The Cholesterol Charity providing expert support, education and influence 2 | Fats in the blood At risk of cardiovascular disease? | 3 Fats in the blood At risk of cardiovascular disease? Fats that circulate in the blood are called lipids. Very low density lipoproteins (VLDL) transport Cardiovascular disease (CVD) is the medical Blood pressure is a measure of the resistance Cholesterol and triglycerides are both lipids. mainly triglycerides made by the liver to where name for circulatory diseases such as coronary to the flow of blood around your body. It is They have essential roles in the body. In excess they are either used to fuel our muscles or stored heart disease (CHD), stroke, mini stroke (transient measured in millimetres of mercury (mmHg). Your they are harmful. for later use. ischaemic attack or TIA), angina and peripheral doctor or nurse will measure both your systolic vascular disease (PVD). You are more likely to (upper figure) and diastolic (lower figure) blood Cholesterol is needed to build cell walls and Low density lipoproteins (LDL) carry most of the develop CVD the more risk factors you have. pressure. About a third of adults have high blood to make hormones and vitamin D. Some of our cholesterol in our body from the liver to the cells pressure. If untreated it increases the risk of cholesterol comes from the food we eat; but most that need it. The cholesterol that is carried on LDLs There are two types of risk factors: heart attack and stroke. High blood pressure is is made in the liver. -

Effects of Dietary Fats on Blood Lipids: a Review of Direct Comparison Trials
Open access Editorial Open Heart: first published as 10.1136/openhrt-2018-000871 on 25 July 2018. Downloaded from Effects of dietary fats on blood lipids: a review of direct comparison trials James J DiNicolantonio, James H O’Keefe To cite: DiNicolantonio JJ, INTRODUCTION very LDL (VLDL) and HDL are also inconsis- O’Keefe JH. Effects of dietary Saturated fat has been demonised as a dietary tent.11 Thus, it is impossible to know what the fats on blood lipids: a review of overall health impact is when saturated fat is direct comparison trials. Open culprit in heart disease due to its ability to Heart 2018;5:e000871. raise low-density lipoprotein cholesterol replaced with omega-6 PUFA. doi:10.1136/ (LDL-C), whereas omega-6 polyunsaturated openhrt-2018-000871 fatty acid (PUFA) has been regarded as MONOUNSATURATED FAT VERSUS SATURATED heart healthy due to its ability to lower total FAT Accepted 3 July 2018 and LDL-C. And replacing saturated fat with Monounsaturated fat ((MUFA) such as oleic omega-6 has consistently been found to lower 1 2 acid, which is found in olive oil, has classically total cholesterol and LDL-C levels. This has been thought of as being heart healthy as been the cornerstone for the belief that the olive oil is the main dietary fat used in the omega-6 PUFA linoleic acid is heart healthy. Mediterranean region, which is well known However, the changes in LDL-C do not take for its low risk for cardiovascular disease. into account the overall changes in the entire Meals high in both MUFA and satu- lipoprotein profile. -
Saturated, Unsaturated, and Trans Fat
Lifestyle Coach Facilitation Guide: Post-Core Fats - Saturated, Unsaturated, and Trans Fat Content Overview This session answers the question “what is fat?” It explores the different types of fat, and shows which fats are healthy (monounsaturated and polyunsaturated) and which fats are unhealthy (saturated and trans fat). Participants learn tips for choosing foods with healthy fats and avoiding foods with unhealthy fats. More information on cholesterol appears in Post-Core Session: Heart Health. Lifestyle Coach Preparation Checklist Materials Post-core handouts: What is Fat? Healthy Fats: Omega-3, Monounsaturated and Polyunsaturated Fats to Avoid: Saturated and Trans Fat Identifying Healthier Alternatives Tips for Choosing the Best Types of Fat “Food and Activity Trackers” “Lifestyle Coach’s Log” Balance scale Post-Core: Fats – Saturated, Unsaturated, and Trans Fat Key messages to reinforce A completely fat-free diet would not be healthy, yet it is important that fat be consumed in moderation. The main types of “healthy” fats are monounsaturated and polyunsaturated. The main types of “unhealthy” fats are saturated and trans fat. Saturated fats are primarily found in foods that come from animals, such as meat and dairy. Try to switch to lower-fat versions of these foods. In order to avoid trans fat, look on nutrition labels for ingredients such as “partially hydrogenated” oils or shortening. In addition, look for trans fat in the nutritional information in products like commercially baked cookies, crackers, and pies, and fried foods. After the session At the completion of this session, do the following: Use the “Notes and Homework Page” for notes and follow-up tasks. -

Saturated Fat and Beef Fat As Related to Human Health a Review of the Scientifi C Literature
FRI BRIEFINGS Saturated Fat and Beef Fat as Related to Human Health A Review of the Scientifi c Literature Ellin Doyle, Ph.D. Food Research Institute, University of Wisconsin Madison, WI 53706 [email protected] TABLE OF CONTENTS Summary ...........................................................................................................2 Introduction ............................................................................................................5 Fat Structure and Function ..................................................................................5 Fatty Acids and Triacylglycerol (Triglyceride) Structure ..................................5 Beef Fat ............................................................................................................7 Digestion and Absorption of Dietary Fats ..........................................................7 Physiological Fate of Saturated Fatty Acids ......................................................9 Research on Saturated Fat and Health — General Considerations ...................9 Cancer ..........................................................................................................10 Colorectal Cancer .............................................................................................10 Pancreatic Cancer .............................................................................................15 Lung Cancer .....................................................................................................15 Breast Cancer ...................................................................................................16 -

The Scoop on Coconut Oil Coconut Oil Is an Edible Oil Extracted from the “Meat” of Matured Coconuts
Family and Consumer Science/Extension Homemakers Club May/June 2016 The Scoop on Coconut Oil Coconut oil is an edible oil extracted from the “meat” of matured coconuts. It has several appli- cations in the food industry. It is used in processed foods because it is relatively inexpensive and can provide crisp texture to foods. Coconut oil has a high smoke point, the temperature where it starts to break down, which makes it shelf stable and ideal for foods that need a longer shelf-life. Hydrogenated and partially hydrogenated coconut oil are found in cereals, baked goods, biscuits, salty snacks, soaps, cosmetics and moisturizers. According to some health food promoters and celebrity doctors, coconut oil is the latest miracle food, claiming it can cure everything from heart disease to obesity and cancer. However, the ef- fects of coconut oil on health have not been well studied. These health claims tend to be based more on personal testimonials than on scientific evidence. In fact, there are very few studies in people showing benefits of coconut oil – most of these studies are epidemiology studies (e.g., population studies) that show a link between high coconut-consuming countries and longevity [1 -2]. Coconut oil is considered a saturated fat and contains 9 calories per gram. There are two basic types of fats – saturated and unsaturated. Unsaturated fats are healthy fats and include plant- based fats (such as vegetable oils and fats found in nuts, avocados and seeds) and fish oils. These fats should be the primary fats in your diet because they either do not affect cholesterol levels or they raise HDL (good) cholesterol without raising LDL (bad) cholesterol. -

Fatty Acids: Structures and Introductory Article Properties Article Contents
Fatty Acids: Structures and Introductory article Properties Article Contents . Introduction Arild C Rustan, University of Oslo, Oslo, Norway . Overview of Fatty Acid Structure . Major Fatty Acids Christian A Drevon, University of Oslo, Oslo, Norway . Metabolism of Fatty Acids . Properties of Fatty Acids Fatty acids play a key role in metabolism: as a metabolic fuel, as a necessary component of . Requirements for and Uses of Fatty Acids in Human all membranes, and as a gene regulator. In addition, fatty acids have a number of industrial Nutrition uses. Uses of Fatty Acids in the Pharmaceutical/Personal Hygiene Industries Introduction doi: 10.1038/npg.els.0003894 Fatty acids, both free and as part of complex lipids, play a number of key roles in metabolism – major metabolic fuel (storage and transport of energy), as essential components subsequent one the b carbon. The letter n is also often used of all membranes, and as gene regulators (Table 1). In ad- instead of the Greek o to indicate the position of the double dition, dietary lipids provide polyunsaturated fatty acids bond closest to the methyl end. The systematic nomencla- (PUFAs) that are precursors of powerful locally acting ture for fatty acids may also indicate the location of double metabolites, i.e. the eicosanoids. As part of complex lipids, bonds with reference to the carboxyl group (D). Figure 2 fatty acids are also important for thermal and electrical outlines the structures of different types of naturally insulation, and for mechanical protection. Moreover, free occurring fatty acids. fatty acids and their salts may function as detergents and soaps owing to their amphipathic properties and the for- Saturated fatty acids mation of micelles. -

Cut Down on Saturated Fats
DIETARY GUIDELINES Cut Down on FOR AMERICANS 2015-2020 EIGHTH EDITION Saturated Fats Limiting saturated fats is important for your health — and it doesn’t mean you have to cut down on flavor. Learn how to swap out saturated fats for healthier options. The 2015–2020 Dietary Guidelines for Americans recommends limiting calories from saturated fats to less than 10% of the total calories you eat and drink each day. That’s about 200 calories for a 2,000 calorie diet. What are saturated fats? What are unsaturated fats? Saturated fats are one type of fat in the foods we eat and the Unsaturated fats are beverages we drink. Most come from animal products, like dairy, found in some foods and meat, and poultry. To limit the amount of saturated fats you eat, most oils. There are 2 choose lower-fat and lean options of dairy, meat, and poultry — types of unsaturated fats: like skim milk, lean beef, and grilled chicken breast without monounsaturated fatty acids the skin. (MUFA) and polyunsaturated Eating too many foods high in saturated fats can be bad for your fatty acids (PUFA). health. By replacing saturated fats with unsaturated fats, you may While saturated fats have lower your risk of getting heart disease. health risks, unsaturated fats have health benefits. Focus on getting unsaturated What foods and beverages are higher fats from: in saturated fats? • Seafood (like salmon, trout, herring, tuna, and mackerel) • Meats higher in fat, like beef ribs, sausage, and some • W alnuts, almonds, cashews, processed meats and most other nuts • Higher-fat dairy, like regular-fat cheeses and whole or 2% milk • Sesame, pumpkin, and flax • Butter, stick margarine, cream, and cream cheese seeds • Some tropical oils, like coconut and palm kernel oil • Olive, canola, peanut, • Cakes, cookies, and some snack foods sunflower, safflower, corn, soybean, and cottonseed oils* Dishes with many ingredients — like pizza, casseroles, burgers, • A vocados tacos, and sandwiches — tend to have ingredients that are high in saturated fats. -

Omega-6:Omega-3 Fatty Acid Ratio and Total Fat Content of the Maternal Diet Alter Offspring Growth and Fat Deposition in the Rat
nutrients Article Omega-6:Omega-3 Fatty Acid Ratio and Total Fat Content of the Maternal Diet Alter Offspring Growth and Fat Deposition in the Rat Sally A. V. Draycott 1,2,*, Matthew J. Elmes 1, Beverly S. Muhlhausler 2,3 and Simon Langley-Evans 1 1 Sutton Bonington Campus, School of Biosciences, University of Nottingham, Loughborough LE12 5RD, UK; [email protected] (M.J.E.); [email protected] (S.L.-E.) 2 Food and Nutrition Research Group, Department of Food and Wine Science, School of Agriculture, Food and Wine, University of Adelaide, Adelaide, SA 5064, Australia; [email protected] 3 Commonwealth Scientific and Industrial Research Organisation, Adelaide, SA 5000, Australia * Correspondence: [email protected] Received: 1 July 2020; Accepted: 13 August 2020; Published: 19 August 2020 Abstract: Omega-3 long-chain polyunsaturated fatty acids (LCPUFA) have been shown to inhibit lipogenesis and adipogenesis in adult rats. Their possible early life effects on offspring fat deposition, however, remain to be established. To investigate this, female Wistar rats (n = 6–9 per group) were fed either a 9:1 ratio of linoleic acid (LA) to alpha-linolenic acid (ALA) or a lower 1:1.5 ratio during pregnancy and lactation. Each ratio was fed at two total fat levels (18% vs. 36% fat w/w) and offspring were weaned onto standard laboratory chow. Offspring exposed to a 36% fat diet, irrespective of maternal dietary LA:ALA ratio, were lighter (male, 27 g lighter; female 19 g lighter; p < 0.0001) than those exposed to an 18% fat diet between 3 and 8 weeks of age. -

The Truth About Coconut Oil ( by Kathleen M
The Truth About Coconut Oil (http://www.webmd.com/diet/features/coconut-oil-and-health) By Kathleen M. Zelman, MPH, RD, LD, WebMD Expert Column Coconut oil, according to recent reports, is the latest food cure-all. Claims abound that coconut oil is a health food that can cure everything from poor immune function, thyroid disease, and heart disease, to obesity, cancer, and HIV. So should you stock up on coconut oil? Not so fast. The evidence that coconut oil is super-healthful is not convincing and these claims appear to be more testimonials than clinical evidence. There is very limited evidence on disease outcomes, says Dariush Mozaffarian, MD, DrPH, of Harvard Medical School and Harvard School of Public Health. "All that has been studied well is the impact of coconut oil on cholesterol levels and the findings are intriguing but we still don't know if it is harmful or beneficial," Mozaffarian says. Neither the American Heart Association (AHA) nor the U.S. government's 2010 Dietary Guidelines suggest that coconut oil is any better or preferable over other saturated fats. Coconut oil, like all saturated fats, should be limited to 7%-10% of calories because it can increase risk for heart disease, according to the AHA and 2010 Dietary Guidelines. What Is Coconut Oil? Pure virgin coconut oil, containing no hydrogenation (the process of adding hydrogen to make a liquid fat hard), contains 92% saturated fat -- the highest amount of saturated fat of any fat. Most saturated fats are solid at room temperature, found in animal products (such as meat, dairy, poultry with skin, and beef fat) and contain cholesterol. -

Final Thesis
ABSTRACT What a Fat Debacle: Saturated and Trans Fatty Acids Effect on Health and the Future of Food Manufacturing Processes Liz Kong Director: Dr. Janelle M. Walter The recommended consumption of fat has been changed multiple times by the USDA’s Dietary Guidelines for Americans in the past decade due to expanding nutrition knowledge. Not only the amount of fat, but the type of fat in the American diet is considered for recommendations to health and food production. Saturated fats in general have long been shown to contribute to chronic diseases such as cardiovascular disease, cancer, and obesity. In response to consumers’ demands for healthier food products, food manufacturers started using the hydrogenation process to lower the saturated fat content of foods. However, research on health implications and subsequent policy changes of these trans fatty acids, such as listing trans fat content on food label nutrition facts, led the same food companies to re-evaluate the hydrogenation process, or production of trans fat, and begin using alternatives to partially hydrogenated oils. Fifteen food companies were contacted through their websites and surveyed about what kinds of oils and/or methods they used to replace the previously used partially hydrogenated oils in their food products to maintain standards for taste and texture. This research and literature review reveals that food companies are back to using saturated fats and tropical oils, especially coconut oil, instead of the cheap trans fats in their products. Contradicting facts on saturated fats and coconut oil are further explored, with the emphasis on the beneficial functions of coconut oil. -
Comparison of Dietary Fats Chart
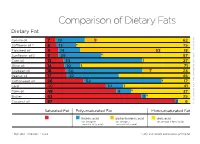
Comparison of Dietary Fats Dietary Fat Canola oil 7 19 9 62 Saower oil † 8 13 75 Flaxseed oil 9 14 53 18 ACCESSED MAY 2016 Sunflower oil ‡ 9 29 57 Corn oil 13 53 1 27 Olive oil 14 10 1 71 Soybean oil 16 50 7 23 Peanut oil 17 32 45 Cottonseed oil 26 52 17 Lard 40 10 1 41 Palm oil 49 9 37 Butter 63 3 25 Coconut oil 87 2 6 SOURCES: CANADIAN NUTRIENT FILE AND USDA NATIONAL NUTRIENT DATABASE Saturated Fat Polyunsaturated Fat Monounsaturated Fat linoleic acid alpha-linolenic acid oleic acid (an omega-6 (an omega-3 (an omega-9 fatty acid) essential fatty acid) essential fatty acid) † High Oleic ‡ Mid Oleic * Trace Fatty acid content expressed as g/100g fat Canola Oil is Healthy Dietary fat, in moderation, is needed to provide energy and help absorb fat-soluble vitamins. Canola oil provides more of the healthy fats than any other common cooking and salad oil. Health professionals recommend: Canola oil may reduce the risk of heart disease Keep total fat intake between 20 to 35 percent of calories In fact, the U.S. Food and Drug Administration authorized a qualified health claim Limit sources of saturated fats and replace with sources for canola oil based on its unsaturated fat content. of unsaturated fats* Avoid trans fat The claim states “limited and not conclusive scientific evidence suggests that eating about 1.5 tablespoons (19 grams) of canola oil daily may reduce the risk of Canola Oil Is: coronary heart disease due to the unsaturated fat content in canola oil. -

Lauric Acid Versus Palmitic Acid: Effects on Adipose Tissue Inflammation, Insulin Resistance, and Non-Alcoholic Fatty Liver Disease in Obesity
biology Article Lauric Acid versus Palmitic Acid: Effects on Adipose Tissue Inflammation, Insulin Resistance, and Non-Alcoholic Fatty Liver Disease in Obesity Viswanathan Saraswathi 1,2,*, Narendra Kumar 1,2, Thiyagarajan Gopal 1,2, Saumya Bhatt 1,2, Weilun Ai 1,2 , Carmen Ma 1,2, Geoffrey A. Talmon 3 and Cyrus Desouza 1,2 1 Department of Internal Medicine, Division of Diabetes, Endocrinology, and Metabolism, University of Nebraska Medical Center, Omaha, NE 68198, USA; [email protected] (N.K.); [email protected] (T.G.); [email protected] (S.B.); [email protected] (W.A.); [email protected] (C.M.); [email protected] (C.D.) 2 VA Nebraska-Western Iowa Health Care System, Omaha, NE 68105, USA 3 Department of Pathology and Microbiology, University of Nebraska Medical Center, Omaha, NE 68198, USA; [email protected] * Correspondence: [email protected]; Tel.: +1-402-995-3033; Fax: +1-402-449-0604 Received: 27 August 2020; Accepted: 14 October 2020; Published: 22 October 2020 Simple Summary: The aim of this study was to compare the effect of palmitic acid (PA), a long-chain fatty acid, and lauric acid (LA), a medium-chain fatty acid, on obesity-related metabolic disorders. We used a mouse model of diet-induced obesity and fed them a modified high fat diet supplemented with 3% PA or LA for 12 wk. An LA diet led to an increase in visceral fat mass with a reduction in inflammation compared to the PA diet. We also noted that PA significantly increased systemic insulin resistance whereas LA showed only a trend towards an increase compared to lean control mice.