Meningitis and Meningococcal Sepsis in Immunocompetent Adults
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Glasgow Coma Scale
CalculatedPOWERED BY Decisions Clinical Decision Support for Pediatric Emergency Medicine Practice Subscribers Glasgow Coma Scale Introduction: The Glasgow Coma Scale (GCS) estimates coma severity based on eye, verbal, and motor criteria. Click the thumbnail above to access the calculator. Points & Pearls • The Glasgow Coma Scale (GCS) allows provid- agreement between providers, training and ers in multiple settings and with varying levels education are available online from the GCS of training to communicate succinctly about a creators at www.glasgowcomascale.org. patient’s mental status. • Simpler scores that have been shown to per- • The GCS has been shown to have statistical form as well as the GCS in the prehospital and correlation with a broad array of adverse neuro- emergency department setting (for initial evalu- logic outcomes, including brain injury, need for ation); these are often contracted versions of the neurosurgery, and mortality. GCS itself. For example, the Simplified Motor • The GCS score has been incorporated into Score (SMS) uses the motor portion of the GCS numerous guidelines and assessment scores only. THE SMS and other contracted scores are (eg, Advanced Cardiac Life Support, Advanced less well studied than the GCS for outcomes Trauma Life Support, Acute Physiology and like long-term mortality, and the GCS has been Chronic Health Evaluation I-III, the Trauma and studied as trended over time, while the SMS has Injury Severity Score, and the World Federation not. of Neurologic Surgeons Subarachnoid Hemor- rhage Grading Scale) Critical Actions Although it has been adopted widely and in a Points to keep in mind: variety of settings, the GCS score is not intended • Correlation with outcome and severity is most for quantitative use. -
Sequential Organ Failure Assessment (SOFA) Score
CalculatedPOWERED BY Decisions Clinical Decision Support for Emergency Medicine Practice Subscribers Sequential Organ Failure Assessment (SOFA) Score Introduction: The SOFA score predicts mortality risk for patients in the intensive care unit based on lab results and clinical data. Click the thumbnail above to access the calculator. Points & Pearls • The Sequential Organ Failure Assessment namically or to determine the success or failure of (SOFA) is a mortality prediction score that is an intervention in the ICU. based on the degree of dysfunction of 6 organ systems. • The score is calculated at admission and every Why to Use 24 hours until discharge, using the worst param- The SOFA score can be used to determine the eters measured during the prior 24 hours. level of organ dysfunction and mortality risk in • The scores can be used in several ways, including: ICU patients. » As individual scores for each organ to deter- mine the progression of organ dysfunction. » As a sum of scores on a single intensive care When to Use unit (ICU) day. • The SOFA can be used on all patients who » As a sum of the worst scores during the ICU are admitted to an ICU. stay. • It is not clear whether the SOFA is reliable for • The SOFA score stratifies mortality risk in ICU patients who were transferred from another patients without restricting the data used to ICU. admission values. Critical Actions Instructions Clinical prediction scores such as the SOFA and the Calculate the SOFA score using the worst value Acute Physiologic Assessment and Chronic Health for each variable in the preceding 24-hour Evaluation (APACHE II) can be measured on all period. -

Lumbar Puncture (LP)
Lumbar puncture (LP) What is a lumbar puncture (LP)? Who will perform this test? An LP is a common and routine procedure, also A doctor trained in performing this procedure known as a spinal tap, where a very small will do the LP. A trained children’s nurse will hold needle is inserted through the base of the spine your infant in the appropriate position (which to collect a sample of the fluid surrounding the is lying on their side curled up in a tight ball). brain and spinal cord. This fluid is called Another team member may also be present to cerebrospinal fluid (CSF). help. Why do we need to do this? Can you be present during the LP? LP is the only way to confirm a case of Yes, you can tell the team that you would like to meningitis (swelling of the lining of the brain be present. However, many parents find it caused by an infection in the CSF). distressing to see any procedures being done on their baby and would rather not be present. This National guidelines strongly recommended that is perfectly understandable. Please let the team an LP is done alongside other routine know and they will usually agree to whatever investigations, such as blood and urine tests, works best for you but be aware that it is best to look for signs of infection if meningitis is to be quiet so the doctor can concentrate on the suspected. This is a routine and very important procedure. investigation. Is it a painful procedure? Getting a sample of CSF will help Drs to find out An LP is an uncomfortable procedure similar to if your child has meningitis and if what is a blood test or drip being inserted. -

Post-Lumbar Puncture Headache—Does Hydration Before Puncture Prevent Headache and Affect Cerebral Blood Flow?
Journal of Clinical Medicine Article Post-Lumbar Puncture Headache—Does Hydration before Puncture Prevent Headache and Affect Cerebral Blood Flow? Magdalena Nowaczewska 1,* , Beata Kukulska-Pawluczuk 2, Henryk Ka´zmierczak 3 and Katarzyna Pawlak-Osi ´nska 1 1 Department of Pathophysiology of Hearing and Balance, Ludwig Rydygier Collegium Medicum in Bydgoszcz Nicolaus Copernicus University, M. Curie 9, 85-090 Bydgoszcz, Poland; [email protected] 2 Department of Neurology, Ludwig Rydygier Collegium Medicum in Bydgoszcz Nicolaus Copernicus University, M. Curie 9, 85-090 Bydgoszcz, Poland; [email protected] 3 Department of Otolaryngology, Head and Neck Surgery, and Laryngological Oncology, Ludwik Rydygier Collegium Medicum in Bydgoszcz Nicolaus Copernicus University, M. Curie 9, 85-090 Bydgoszcz, Poland; [email protected] * Correspondence: [email protected]; Tel.: +48-52-585-4716 Received: 8 September 2019; Accepted: 15 October 2019; Published: 17 October 2019 Abstract: Headache is a common complication after diagnostic lumbar puncture (DLP). We aimed to check whether hydration before puncture influences the incidence of post-lumbar puncture headache (PLPH) and affects cerebral blood flow. Ninety-nine patients enrolled for puncture were assigned to a group with (n = 40) or without hydration (n = 59). In the hydration group, 1000 mL 0.9% NaCl was infused and a minimum of 1500 mL oral fluids was recommended within the 24 h before puncture. A Transcranial Doppler (TCD) was performed before and after DLP. Mean velocity (Vm) and pulsatility index (PI) were measured in the middle cerebral arteries (MCAs). PLPH occurred in 28 patients (28.2%): six (15.4%) from the hydrated and 22 (37.3%) from the non-hydrated group (p < 0.023). -

Trauma Measure #5 Documentation of Glasgow Coma Score at Time of Initial Evaluation in TBI
Trauma Measure #5 Documentation of Glasgow Coma Score at Time of Initial Evaluation in TBI National Quality Strategy Domain: Communication and Care Coordination Measure Type (Process/Outcome): Process 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY DESCRIPTION: Percentage of trauma activations for patients aged 18 years or older evaluated as part of a trauma activation or trauma consultation who have a traumatic intracranial hemorrhage on initial head CT for which a Glasgow Coma Score (GCS) at the time of initial evaluation is documented in the medical record within 1 hour of hospital arrival. INSTRUCTIONS: This measure is to be reported each time a patient is evaluated as part of a trauma activation or trauma consultation and is found to have a traumatic intracranial hemorrhage on initial head CT. It is anticipated that clinicians who are responsible for the initial trauma evaluation of TBI patients as specified in the denominator coding will submit this measure. Measure Reporting via Registry: Abbreviated Injury Scale (AIS) codes, patient demographics, and the medical record are used to identify patients who are included in the measure’s denominator. The listed numerator options are used to report the numerator of the measure. DENOMINATOR: All patients aged 18 years or older evaluated by an eligible professional as part of a trauma activation or trauma consultation who have a traumatic intracranial hemorrhage on initial head CT). Denominator Criteria: Patients aged 18 years or older AND Patients evaluated as part of a trauma activation -

On-Line Table 1: Clinical, EEG, and Perfusion Data of Patients with NCSE Age Pre- Lat Signs/ Perfusion (Visual Seizure No
On-line Table 1: Clinical, EEG, and perfusion data of patients with NCSE Age Pre- Lat Signs/ Perfusion (visual Seizure No. (yr) Sex seizure Jerks GCS Ventilation EEG analysis) Classification Epilepsy Comorbidity Survival 1.1 59 M Coma R/Ϫ 6 ϩ SW Hyperperfusion Ins L Coma with NCSE – Cardiac arrest – FT L 1.2 72 F GTCS L/Ϫ 3 ϩ SW Hyperperfusion SSE ϩ Chronic infarction L ϩ PR PR 1.3 60 F GTCS No/Ϫ 3 ϩ SW Hyperperfusion SSE ϩ Traumatic brain injury ϩ FR FR 1.4 72 F GTCS R/ϩ 7 – SW Hyperperfusion SSE ϩ Chronic infarction L – TL TL 1.5 89 F GTCS L/Ϫ 8 – SW Hyperperfusion SSE ϩ Chronic infarction R – FR FR 1.6 67 F CP No/ϩ 11 – SW No Hyperperfusion CPSE ϩ Chronic infarction L ϩ FL 1.7 62 F GTCS R/Ϫ 5 ϩ SW Hyperperfusion SSE – Meningo-encephalitis – FR Ins,TL 1.8 67 M GTCS R/ϩ 5 ϩ SL Hyperperfusion SSE – Subacute SDH L ϩ FP L Ins L 1.9 63 F CP L/Ϫ 11 – SW No hyperperfusion CPSE ϩ Chronic infarction L ϩ TP L Note:—Lat indicates lateralizing; Pre, preceding: R, right; L, left; SW, spike-wave activity; F, frontal; T, temporal; P, parietal; Ins, insular; SDH, subdural hemorrhage; SL, slowing; EEG, electroencephalography; NCSE, nonconvulsive status epilepticus; GCS, Glasgow Coma Scale; GTCS, generalized tonic-clonic seizure; CP, complex-partial; CPSE, complex-partial status epilepticus; SSE, subtle status epilepticus. AJNR Am J Neuroradiol ͉͉www.ajnr.org E1 On-line Table 2: Clinical, EEG, and perfusion data of patients with a postictal state Age Pre- Lat Perfusion (visual No. -

The Clinical Effect of Lumbar Puncture in Normal Pressure Hydrocephalus
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.45.1.64 on 1 January 1982. Downloaded from Journal of Neurology, Neurosurgery, and Psychiatry 1982;45:64-69 The clinical effect of lumbar puncture in normal pressure hydrocephalus C WIKKELS0, H ANDERSSON, C BLOMSTRAND, G LINDQVIST From the Department of Neurology and Neurosurgery, Sahlgren Hospital, University of Goteborg, Sweden SUMMARY Owing to all the difficulties involved in selecting patients with normal pressure hydro- cephalus for shunt-operation, a cerebrospinal fluid-tap-test (CSF-TT) is introduced. Psychometric and motor capacities of the patients are measured before and after lumbar puncture and removal of 40-50 ml CSF. Patients fulfilling criteria for normal pressure hydrocephalus were compared to patients with dementia and atrophy shown by computed tomography. Normal pressure hydro- cephaluspatients showed temporary improvement after lumbar puncture. The extent ofthe temporary improvement appeared to be well correlated with the improvement after shunt operation. Accord- ingly, the CSF-TT seems to be of value when selecting those patients who will probably benefit from a shunt operation. The syndrome of normal pressure hydrocephalus is pressure by lumbar puncture caused both subjective Protected by copyright. characterised by gait disturbance, progressive mental and objective temporary improvement in some deterioration and urinary incontinence.' Particularly patients with normal pressure hydrocephalus.10 16 17 noteworthy is the complex gait disturbance with Such patients also improved after CSF-shunting. spastic-ataxia, extrapyramidal components, and However, no details have been given about the commonly dyspraxia of gait.2 In addition, there is in amount of CSF which was drained or to what degree typical cases mental "slowing up" with lack of the CSF pressure was lowered. -

Ventriculoperitoneal Shunts in the Emergency Department: a Review
Open Access Review Article DOI: 10.7759/cureus.6857 Ventriculoperitoneal Shunts in the Emergency Department: A Review Michael Ferras 1 , Nicholas McCauley 1 , Trilok Stead 2 , Latha Ganti 3, 4, 5 , Bobby Desai 6 1. Emergency Medicine, Ocala Regional Medical Center, University of Central Florida, Ocala, USA 2. Emergency Medicine, Trinity Preparatory School, Winter Park, USA 3. Emergency Medicine, Envision Physician Services, Orlando, USA 4. Emergency Medicine, University of Central Florida College of Medicine/Hospital Corporation of America Graduate Medical Education Consortium of Greater Orlando, Orlando, USA 5. Emergency Medicine, Polk County Fire Rescue, Bartow, USA 6. Emergency Medicine, Ocala Regional Medical Center, University of Central Florida College of Medicine, Ocala, USA Corresponding author: Latha Ganti, [email protected] Abstract In this paper, we review the indications, complications, and pitfalls associated with ventriculoperitoneal (VP) shunts. As most VP shunt problems initially present to the emergency department, it is important for emergency physicians to be well-versed in managing them. In the article, the possible reasons for shunt failure are explored and summarized using an infographic. We also examine potential clinical presentations of VP shunt failure. Categories: Emergency Medicine, Neurosurgery Keywords: ventriculoperitoneal shunts Introduction And Background Emergency department physicians usually see a large number of patients with medical maladies managed by the aid of instrumentation or hardware such as a ventriculoperitoneal (VP) shunt. While patients have shunts placed for multiple reasons, it is important for emergency service providers to know how to evaluate, troubleshoot, and treat those with VP shunt complications. An estimated 30,000 VP shunt procedures are performed yearly in the United States [1]. -

Role of Lumbar Puncture in Traumatic Brain Injury
308 Indian Journal of Public Health Research & Development, April-June 2021, Vol. 12, No. 2 Role of Lumbar Puncture In Traumatic Brain Injury Ranjeet Kumar Jha1, Rachna Gupta2 1Assistant Professor, Department of Neurosurgery, 2Professor, Department of Surgery, Shyam Shah Medical College, Rewa Abstract Background: Cerebrospinal fluid (CSF) drainage via ventricular puncture is an established therapy of elevated intracranial pressure (ICP). In contrast, lumbar CSF removal is believed to be contraindicated with intracranial hypertension. Method: We investigated the safety and efficacy of lumbar CSF drainage to decrease refractory elevated ICP in a small cohort of patients with traumatic brain injury (TBI). A score (0–8 points) was used to assess computed tomography (CT) images for signs of herniation and for patency of the basal cisterns. All patients received lumbar CSF drainage either as a continuous drainage or as a single lumbar puncture (LP). Type and method of CSF drainage, mean ICP 24 h prior and after CSF removal, and adverse events were documented. Outcome was assessed after 3 months (with dichotomized Glasgow outcome scale). Results: Eight patients were evaluated retrospectively. n = 5 suffered a moderate, n = 2 a severe TBI (one Glasgow coma score not documented). The CT score was ≥5 in all patients prior to LP and decreased after puncture without clinical consequences in two patients. The amount of CSF removal did not correlate with score changes (P = 0.45). CSF drainage led to a significant reduction of mean ICP (from 22.3 to 13.9 mmHg, P = 0.002). Continuous drainage was more effective than a single LP. Three of eight patients reached a favorable outcome. -
Pediatric Index of Mortality 2 Score As an Outcome Predictor in Pediatric Intensive Care Unit in India
Research Article Pediatric index of mortality 2 score as an outcome predictor in pediatric Intensive Care Unit in India Jeyanthi Gandhi, Shanthi Sangareddi, Poovazhagi Varadarajan, Saradha Suresh Background and Aims: Pediatric index of mortality (PIM) 2 score is one of the severity Access this article online scoring systems being used for predicting outcome of patients admitted to intensive Website: www.ijccm.org care units (ICUs). The aim of the present study was to evaluate the usefulness of PIM2 DOI: 10.4103/0972-5229.120320 score in predicting mortality in a tertiary care pediatric ICU (PICU) and to assess the Quick Response Code: Abstract associated factors in predicting mortality such as presence of shock, need for assisted ventilation and Glasgow coma scale <8. Materials and Methods: This was a prospective observation study done at tertiary care PICU from May 2011 to July 2011. Consecutive 119 patients admitted to PICU (aged 1 month to 12 years) were enrolled in the study. PIM2 scoring was done for all patients. The outcome was recorded as death or discharge. The associated factors for mortality were analyzed with SPSS 17. Results: PIM2 score discriminated between death and survival at a 99.8 cut-off, with area under receiver operating characteristic curve 0.843 with 95% confi dence interval (CI) (0.765, 0.903). Most patients were referred late to this hospital, which explains higher death rate (46.2%), lesser length of hospital stay (mean 2.98 days) in the mortality group, and increased rate of mechanical ventilation (68.1%). Presence of shock was independently associated with mortality, as evidenced by binary logistic regression. -

Predictive Value of Scoring System in Severe Pediatric Head Injury
Medicina (Kaunas) 2007; 43(11) 861 Predictive value of scoring system in severe pediatric head injury Dovilė Evalda Grinkevičiūtė, Rimantas Kėvalas, Viktoras Šaferis1, Algimantas Matukevičius1, Vytautas Ragaišis2, Arimantas Tamašauskas1 Department of Children’s Diseases, 1Institute for Biomedical Research, 2Department of Neurosurgery, Kaunas University of Medicine, Lithuania Key words: pediatric head trauma; Glasgow Coma Scale, Pediatric Trauma Score; Glasgow Outcome Scale, Pediatric Index of Mortality 2. Summary. Objectives. To determine the threshold values of Pediatric Index of Mortality 2 (PIM 2) score, Pediatric Trauma Score (PTS), and Glasgow Coma Scale (GCS) score for mortality in children after severe head injury and to evaluate changes in outcomes of children after severe head injury on discharge and after 6 months. Material and methods. All children with severe head injury admitted to the Pediatric Intensive Care Unit of Kaunas University of Medicine Hospital, Lithuania, from January 2004 to June 2006 were prospectively included in the study. The severity of head injury was categorized according to the GCS score ≤8. As initial assessment tools, the PTS, postresuscitation GCS, and PIM 2 scores were calculated for each patient. Outcome was assessed according to Glasgow Outcome Scale on discharge and after 6 months. Results. The study population consisted of 59 children with severe head injury. The group consisted of 37 (62.7%) boys and 22(37.3%) girls; the mean age was 10.6±6.02. The mean GCS, PTS, and PIM 2 scores were 5.9±1.8, 4.8±2.7, and 14.0±19.5, respectively. In terms of overall outcome, 46 (78.0%) patients survived and 13 (22.0%) died. -
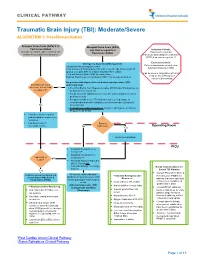
Traumatic Brain Injury (TBI): Moderate/Severe ALGORITHM 1: Post-Resuscitation
CLINICAL PATHWAY Traumatic Brain Injury (TBI): Moderate/Severe ALGORITHM 1: Post-Resuscitation Glasgow Coma Scale (GCS) 9-12 Glasgow Coma Scale (GCS) Post resuscitation less than or equal to 8 Inclusion Criteria: (Consider for children under 2 years old with Post-resuscitation Patient with traumatic concern for acute abusive head trauma) brain injury and Glasgow Coma Scale (GCS) less than or equal to 12 Exclusion Criteria: Emergency Department Management Patients found down without clear Trauma and Neurosurgery Consult traumatic brain injury (TBI) Head Computed Tomography (CT) scan- if not already obtained (STAT upload) or a quick MRI as a viable (radiation-free) option (Can be used in conjunction with Post 2 IVs with Normal Saline (NS) as maintenance Cardiac Arrest Pathway if Modified Rapid sequence intubation (RSI) if not already performed considered beneficial) For patients with signs of elevated intracranial pressure (ICP) Monitor GCS. GCS empirically treat decrease to less than Yes • 3% (0.5 mEq/mL Na+) Hypertonic saline (HTS) bolus 5mL/kg/dose via or equal to 8? peripheral IV or central line • For patients with ongoing seizures use the status epilepticus clinical pathway (below). • For patients with severe TBI who have not received a dose of levetiracetam at another institution, give levetiracetam 20mg/kg IV No (max 2 grams) • If transporting to Operating Room: Consider mild hyperventilation to PCO2 of 32-35 mmHg • Consider comfort sedation and standard neuroprotective measures. • Complete frequent Surgery neurologic exams. No Indicated?