Prevalence of Periodontitis in Rural and Urban Population
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
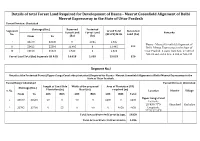
Details of Total Forest Land Required for Development of Dasna
Details of total Forest Land Required for Development of Dasna - Meerut Greenfield Alignment of Delhi Meerut Expressway in the State of Uttar Pradesh Forest Division: Ghaziabad Chainage (Km.) Reserved Protected Segments Grand Total Non-forest Forest Land Forest Land Remarks No. (RF+PF) in Ha Land (ha) From To (ha) (ha) I 33570 33630 0 1.035 1.035 Dasna - Meerut Greenfield Alignment of 320 II 53422 55396 11.495 0 11.495 Delhi Meerut Expressway in the State of III 23100 36520 2.523 0 2.523 Uttar Pradesh. It starts from Km. 27.500 of NH-24 and end at Km. 8.800 of NH-235 Forest Land Total (ha) Segments I,II & III 14.018 1.035 15.053 320 Segment No.I Details of the Protected Forest (Upper Ganga Canal side plantation) Required for Dasna - Meerut Greenfield Alignment of Delhi Meerut Expressway in the State of Uttar Pradesh. Forest Range: Ghaziabad Forest Division: Ghaziabad Length of Canal Side Width of the proposed Area of Plantation (PF) Chainage (Km.) S. No. Plantation (m) Road (m) required (m) Location District Village From To LHS RHS LHS RHS LHS RHS Total Upper Ganga Canal 1 33570 33630 60 0 90 0 5400 0 5400 Latitude: 28°43'0.77"N Ghaziabad Kushaliya 2 33705 33760 0 55 0 90 0 4950 4950 Longitude: 77°32'27.28"E Total Area of Protected Forest in Sqm. 10350 Total Area of Protected Forest in ha 1.035 Segment No.II Details of the Reserved Forest Land Required for Development of Dasna - Meerut Greenfield Alignment of Delhi Meerut Expressway in the State of Uttar Pradesh. -

Common Sheet of Containment Zone (1).Xlsx
CONTAINMENT ZONE INFORMATION OF DISTRICT GHAZIABAD Expected Desealing Date ( if next 14 NAME OF CONTAINMENT DATE OF Police Station Sl.No. Name of epi-centre days no another ZONE/ Hotspot Area SELLING positive will be found) KAVINAGAR H NO 840 VIVEKANAND NAGAR GZB 24-08-2020 07-09-2020 1 Vivekanand Nagar KAVINAGAR H NO 840 VIVEKANAND NAGAR GZB 25-08-2020 08-09-2020 KAVINAGAR CHIRANJEEV VIHAR SEC-02 22-08-2020 05-09-2020 2 Chiranjivi Vihar KAVINAGAR H.NO-07 SECTOR 09 CHIRANJEEV VIHAR 26-08-2020 09-09-2020 KAVINAGAR A-353 SANJAY NAGAR GZB 19-08-2020 02-09-2020 KAVINAGAR M-276 B, Sector 23, Sanjay Nagar, Ghaziabad 21-08-2020 04-09-2020 KAVINAGAR Guldhar IInd, Sec 23, Sanjay Nagar, Ghaziabad 21-08-2020 04-09-2020 KAVINAGAR CV 21 SEC-23 SANJAY NAGAR COLONY 22-08-2020 05-09-2020 KAVINAGAR CV 21 SEC-23 SANJAY NAGAR COLONY 22-08-2020 05-09-2020 KAVINAGAR CV 21 SEC-23 SANJAY NAGAR COLONY 22-08-2020 05-09-2020 KAVINAGAR H.NO- CV 21 SEC- 23 SANJAY NAGAR 22-08-2020 05-09-2020 KAVINAGAR H.NO- CV 21 SEC- 23 SANJAY NAGAR 22-08-2020 05-09-2020 KAVINAGAR 1,39 g.f sanjay nagar sec 23 gzb 22-08-2020 05-09-2020 KAVINAGAR J-389, SANJAY NAGAR, GZB 26-08-2020 09-09-2020 KAVINAGAR H-1, GALI NO,- 03, SANJAY NAGAR GZB 26-08-2020 09-09-2020 KAVINAGAR SEC-23 SANJAY NAGAR GHAZIABAD 26-08-2020 09-09-2020 KAVINAGAR SANJAY NAGAR 26-08-2020 09-09-2020 KAVINAGAR 37-A JAGRITI VIHAR SEC-23 SANJAY NAGAR 26-08-2020 09-09-2020 3 Sector 23, Sanjay Nagar KAVINAGAR 37-A JAGRITI VIHAR SEC.23 SANJAY NAGAR 26-08-2020 09-09-2020 KAVINAGAR 100 JAGRITI VIHAR SEC-23 SANJAY NAGAR 26-08-2020 09-09-2020 KAVINAGAR NEW FRIENDS COLONY 26-08-2020 09-09-2020 KAVINAGAR H.NO G1 SECTOR -23 GHAZIABAD U.P 26-08-2020 09-09-2020 KAVINAGAR H-E 143 SEC-23 SANJAY NAGAR GHAZIABAD 28-08-2020 11-09-2020 KAVINAGAR G-195, SANJAY NAGAR 28-08-2020 11-09-2020 KAVINAGAR E 143 SEC-23 SANJAY NAGAR GHAZIABAD 28-08-2020 11-09-2020 KAVINAGAR H.1 GALI NO. -

Central Administrative Tribunal Principal Bench, New Delhi
Central Administrative Tribunal Principal Bench, New Delhi O.A. No.2988/2018 M.A. No.3000/2018 Monday, this the 13th day of August 2018 Hon’ble Mr. K.N. Shrivastava, Member (A) Hon’ble Mr. S.N. Terdal, Member (A) P.No.6392 Tractor Dvr. Group C Ashbir Singh s/o Shri Sumer Singh Aged 32 years r/o Village- Babugarh PO & PS Babugarh Tehsil-Hapur, Distt. Ghaziabad Uttar Pradesh – 245201 ..Applicant (Dr. K D S Dalal and Mr. Ranjit Singh, Advocates) Versus 1. Union of India through the Secretary Ministry of Defence South Block, New Delhi – 110 011 2. Director General Veterinary Services QMG’s Branch Integrated HQ of MoD (Army) West Block -3, R K Puram New Delhi 3. Commandant Enquine Breeding Stud Babugarh – 245201 Distt. Ghaziabad (UP) ..Respondents (Dr. L C Singhi, Advocate) O R D E R (ORAL) Mr. K.N. Shrivastava: The respondent No.3, vide Annexure A-3 (colly.) Advertisement Notice dated 11.03.2011, invited applications for the posts of Tractor Driver and Godown Overseer. It was indicated in the Notice that 5 posts of 2 Tractor Driver are to be filled up. The applicant applied for the post of Tractor Driver and participated in the selection process. He was declared successful. The respondent No.3, vide appointment letter dated 10.10.2011 (p.59), appointed the applicant to the post of Tractor Driver. His appointment was under the OBC quota. 2. The respondent No.3 conducted a preliminary inquiry in regard to the OBC status of the applicant. It came to the notice of respondent No.3 that the applicant belongs to Jat community of Uttar Pradesh, which does not come under the OBC list of Central Government, and thus, felt that the applicant has secured the said employment on the basis of ineligible caste certificate. -

Regional Office - U.P
Regional Office - U.P. Pollution Control Board, Ghaziabad S.No. Name And Address Of The Products Hazardous HW Generating Streams HW Generation In Total Quantity Of HW In MTA (10) Remark Unit Manufactured In Waste (HW) As Per MTA As Per Quantity Of MTA Generating HW Process As Sch. 1 Sch. 2 Sch. 1 Sch. 2 Generation Landfillable Recyclable Incinerable Per Schedule In MTA 1 1 2 3 4 5 6 7 8 9=7+810 11 Closed Unit 1 BHAGWATI PHOSPH&ELEC 12 12.5 0.9 0.9 0.9000 0.0000 0.0000 SELF ENTERPRISES, PL(Ni&Cr) CLOSED S-28, SITE-4, SBD JOB WORK BASIS 2 F.M. PARTS & BREAK DISC 15 15.3 0 0 0.0000 0.0000 0.0000 SELF COMPONENT (P0 LTD, 31 CLOSED A LONI RD I.A. MOHAN NGR. 3 REINZ TALBROS LTD. , GASKET 15 15.3 0 0 0.0000 0.0000 0.0000 CLOSED 19,LONI Rd.MOHAN NGR JOINTING 4 GOOD LUCK INDUSTRY, H.F. ACID 17 17.1 120 120 120.0000 0.0000 0.0000 SELF CLOED 122, A.I.A., MOHAN NGR. 10 MT/D OWN REASONS 5 PANKAJ CHEMICALS, 80, H.F. ACID 17 17.1 0 0 0.0000 0.0000 0.0000 CLOSED R.I.A., MOHAN NGR., 6 ARISTRO PRINTERS P PRINTING OF 21 21.1 0.6 0.6 0.0000 0.0000 0.6000 SELF LTD., E-64, S.S. OF G.T. PAPERS CLOSED ROAD. 7 ASIA CHEMICAL, G.T. PAINTS & 21 21.1 6 6 0.0000 6.0000 0.0000 SELF ROAD, VARNISH CLSOED 8 ADDI INDUSTRIES, C-227, FABRIC 24 24.2 6 6 6.0000 0.0000 0.0000 SELF B.S. -
District Census Handbook, Meerut, Part X-A, Series-21, Uttar Pradesh
CENSUS 1971 PART X-A Tcr\VN< & VILLAGE DIRECTORY SERIES 21 UTTAR PRADESH DISTRICT. DISTRICT MEERUT CENSUS HANDBOOK D. M. SINHA OF THE i};DIAN AD1IlNISTRATIVE SERVICE Director of Census Operatiorn Uttar Pradesh DISTRICT MEERUT I 10 I) 10 KMS b:.u.=.:.- -± - - 1--±=:;d o ". IL- f- i ,<-lS 01STRICT 1l0UNOARY TAHSIL BOUNDARY 'YIKAS ~HflND IIOUNDARY DISTRICT HEAOQUARTERS TAHSIL HEA.OQUA.RnR~ I""" ~ VtKIS KHA.Ha H~AOQU"'fHkS .~".'"' ,." 10111101 OF THE DIITRICT o ,v • ,.~\ ',., IN UTTAR PRIOEIH URBAN IUfA f/ c'~"'\f/ IJ . ~ - \, ,. "\ VILI.AGE WITH POPULATION MI]lI Olt "1011£ • ~~,' :'\ 0 IO::J 200 .(\,~S HIGHWAYS. NA1'IONAL, ,TATE l~iltUL_ )..'1:) r'; ~ OTHER IMPORTANT ROAD' ' ____ .- I R.A1L'hAV UI\IE WITH STAttON. BROAD (iIl.UC.EI, __ "i~ .... _ Nome of the A,,, in IPoPUIO\iOn No." No. of NARROW"A.UGEI~_ ,\. Tahsil K.' Villagfs Towns v;:-.... RIVER AND 5TRfAH I " ........ '" ~),. BlGHPII 1,0lll 561,066 154 CANAL WI1l11MPORTANT DISTRIBUiflfW \ I GHIZIIBAD 1.0581 718.91J III POlICf STATION P5 IIROHINI 895·1 4\M11 106 ron & nLEG.RA~H OFFICe. I PI MEERUI 7110 141.B14 119 RtH HOUSi TRAVELLERS' BUNGALOW, HC, I RH 5" HAmA 1.098.4 J90.))5 l06 HOSPITAL, PlSPENSARY,P, H, CENnE, ETC + HAPUR 1.0811 516.73B ll, DEGREE (OLlEG£, H. S, SCHOOL 8,0 TOTAL 5,944.0 3,%6.951 1,651 22 L_·--~~~~~-o~,--------~------------~~------~----~----~---, , 77 15 East of Gr"cw", 30 ~5 CONTENTS Pages Acknowledgements Introductory Note iii TOWN AND VILLA.GE DIRECTORY Town Directory Statement I-Status, Growth History and Functional Category of Towns 4-5 Statement II-Physical Aspects -

Seat Details
Aided Group and Institute wise Vacant Seats - 2020 for Round 4 Group - A Course Code Course Name No. of Seats 1 B R ENGINEERING INSTITUTE, BICHPURI, AGRA (RAJA BALWANT SINGHPOLYTECHNIC, BICHPURI , AGRA ) CIVIL ENGINEERING (ENVIRONMENT & POLLUTION CONTROL) 33 ELECTRICAL ENGINEERING (INDUSTRIAL CONTROL) 20 2 CHANDAULI POLYTECHNIC, CHANDAULI CIVIL ENGINEERING 3 ELECTRICAL ENGINEERING 3 ELECTRONICS ENGINEERING 16 MECHANICAL ENGINEERING (PRODUCTION) 4 3 D J POLYTECHNIC, BARAUT, BAGHPAT CIVIL ENGINEERING 43 ELECTRICAL ENGINEERING 27 MECHANICAL ENGINEERING (PRODUCTION) 39 4 D N POLYTECHNIC, MEERUT CIVIL ENGINEERING 17 ELECTRICAL ENGINEERING 10 MECHANICAL ENGINEERING (PRODUCTION) 10 5 FIROZE GANDHI POLYTECHNIC, RAIBARELI ELECTRONICS ENGINEERING 13 INSTRUMENTATION AND CONTROL 43 MECHANICAL ENGINEERING (PRODUCTION) 5 6 GANDHI POLYTECHNIC, MUZAFFAR NAGAR CIVIL ENGINEERING 21 ELECTRICAL ENGINEERING 11 MECHANICAL ENGINEERING (AUTOMOBILE) 28 MECHANICAL ENGINEERING (PRODUCTION) 21 7 HANDIA POLYTECHNIC HANDIA, PRAYAGRAJ CIVIL ENGINEERING 9 ELECTRICAL ENGINEERING 6 MECHANICAL ENGINEERING (PRODUCTION) 14 8 HEWETT POLYTECHNIC, LUCKNOW CIVIL ENGINEERING 10 ELECTRICAL ENGINEERING 5 MECHANICAL ENGINEERING (PRODUCTION) 7 9 INSTITUTE OF TOOLROOM TRAINNING,AMAUSI INDUSTRIAL AREA, NADARGANJ, KANPUR ROAD, LUCKNOW DIPLOMA IN TOOL AND MOULD MAKING (4 Yr. Course) 66 10 JANTA POLYTECHNIC, JAHANGIRABAD, BULANDSHAHAR ELECTRONICS ENGINEERING 45 11 JAWAHAR LAL NEHRU POLYTECHNIC, MAHMOODABAD, SITAPUR CIVIL ENGINEERING 7 ELECTRONICS ENGINEERING 26 DAIRY ENGINEERING 58 12 -

List of Class Wise Ulbs of Uttar Pradesh
List of Class wise ULBs of Uttar Pradesh Classification Nos. Name of Town I Class 50 Moradabad, Meerut, Ghazia bad, Aligarh, Agra, Bareilly , Lucknow , Kanpur , Jhansi, Allahabad , (100,000 & above Population) Gorakhpur & Varanasi (all Nagar Nigam) Saharanpur, Muzaffarnagar, Sambhal, Chandausi, Rampur, Amroha, Hapur, Modinagar, Loni, Bulandshahr , Hathras, Mathura, Firozabad, Etah, Badaun, Pilibhit, Shahjahanpur, Lakhimpur, Sitapur, Hardoi , Unnao, Raebareli, Farrukkhabad, Etawah, Orai, Lalitpur, Banda, Fatehpur, Faizabad, Sultanpur, Bahraich, Gonda, Basti , Deoria, Maunath Bhanjan, Ballia, Jaunpur & Mirzapur (all Nagar Palika Parishad) II Class 56 Deoband, Gangoh, Shamli, Kairana, Khatauli, Kiratpur, Chandpur, Najibabad, Bijnor, Nagina, Sherkot, (50,000 - 99,999 Population) Hasanpur, Mawana, Baraut, Muradnagar, Pilkhuwa, Dadri, Sikandrabad, Jahangirabad, Khurja, Vrindavan, Sikohabad,Tundla, Kasganj, Mainpuri, Sahaswan, Ujhani, Beheri, Faridpur, Bisalpur, Tilhar, Gola Gokarannath, Laharpur, Shahabad, Gangaghat, Kannauj, Chhibramau, Auraiya, Konch, Jalaun, Mauranipur, Rath, Mahoba, Pratapgarh, Nawabganj, Tanda, Nanpara, Balrampur, Mubarakpur, Azamgarh, Ghazipur, Mughalsarai & Bhadohi (all Nagar Palika Parishad) Obra, Renukoot & Pipri (all Nagar Panchayat) III Class 167 Nakur, Kandhla, Afzalgarh, Seohara, Dhampur, Nehtaur, Noorpur, Thakurdwara, Bilari, Bahjoi, Tanda, Bilaspur, (20,000 - 49,999 Population) Suar, Milak, Bachhraon, Dhanaura, Sardhana, Bagpat, Garmukteshwer, Anupshahar, Gulathi, Siana, Dibai, Shikarpur, Atrauli, Khair, Sikandra -
Meerut Zone, Opposite Ccs University, Mangal Pandey Nagar, Meerut
OFFICE OF THE CHIEF COMMISSIONER, CUSTOMS, CENTRAL GOODS AND SERVICES TAX:: MEERUT ZONE, OPPOSITE CCS UNIVERSITY, MANGAL PANDEY NAGAR, MEERUT Designation of CPIOs & Appellate Authorities in CBEC Website under RTI ACT 2005 :: MEERUT ZONE REPORT FOR THE QUARTER ENDING March – 2018 A. Chief Commissioner/ Director General/ Director Notified Office/ Location Officer Name & Designation of the S. No. of Chief Name & Designation of the CPIO Jurisdiction for Appellate Authority Commissionerate payment of fees Shri R. K. Gupta, Shri Roshan Lal, Assistant Commissioner, Joint Commissioner O/o the Chief Commissioner, O/o the Chief Commissioner, Assistant Information pertaining Opp. CCS University, Mangal Opp. CCS University, Mangal Chief to the Office of the 1 Meerut Zone Pandey Nagar, Meerut - 250004 Pandey Nagar, Meerut - 250004 Accounts Chief Commissioner, Ph No: 0121-2792745 Ph No: 0121-2600605 Officer, Meerut Zone, Meerut. Fax No: 0121-2761472 Fax No:0121-2769707 Central Email: [email protected] Email: [email protected] GST, [email protected] [email protected] Meerut B. Commissioner/ Addl. Director General Notified S. Commission Name & Designation of the officer for Name & Designation of the CPIO Jurisdiction No. erate Appellate Authority payment of fees Areas falling Shri Kamlesh Singh Shri Roshan Lal Joint Commissioner under the Assistant Chief Assistant Commissioner Districts of Accounts O/o the Commissioner, Office of the Commissioner of Central Meerut, Officer, Office Central GST Commissionerate Goods & Services Tax, Baghpat, of the Central GST Meerut, Opp. CCS University, Commissionerate: Meerut, Opposite: Muzaffarnagar, Commissioner Meerut Mangal Pandey Nagar, Meerut. Saharanpur, 1 Chaudhary Charan Singh University, of Central Commissione Fax No: 0121-2792773 Shamli, Goods & Mangal Pandey Nagar, Meerut- rate Amroha, Services Tax, 250004 Moradabad, Commissionera Bijnore and te: Meerut Ph No: 0121-2600605 Rampur in the Fax No:0121-2769707 State of Uttar Pradesh. -

Planning Proposals for Water Supply of U.P. Sub Region of Ncr
PLANNING PROPOSALS FOR WATER SUPPLY OF U.P. SUB REGION OF NCR A DISSERTATION Submitted in partial fulfilment of the requirements for the award of the degree of MASTER OF URBAN AND RURAL PLANNING By MATINDER KUMAR DEPARTMENT OF ARCHITECTURE & PLANNING INDIAN INSTITUTE OF TECHNOLOGY ROORKEE ROORKEE - 247 667 (INDIA) JUNE, 2007 CANDIDATE'S DECLARATION I hereby certify that the work, which is being presented in the dissertation, entitled "PLANNING PROPOSALS FOR WATER SUPPLY OF U.P. SUB REGION OF NCR", in partial fulfillment of the requirement for the award of the Degree of MASTER OF URBAN AND RURAL PLANNING submitted in the Department of Architecture and Planning, Indian Institute of Technology - Roorkee, is an authentic record of my own work carried out during the period from May 2006 to June 2007 under the supervision of Prof. R. K. Jain, Associate Professor, Department of Architecture and Planning, Indian Institute of Technology - Roorkee. The matter embodied in this dissertation has not been submitted by me for the award of any other Degree. Place: Roorkee ktrAihnkt Dated: June 2c12007 (Matinder Kumar) This is to certify that the above statement made by the candidate Mr. Matinder Kumar is correct to the best of my knowledge. Place: Roorkee Dated: June, 2007 (Prof. R. K. Jain) Associate Professor Department of Architecture and Planning Indian Institute of Technology - Roorkee Roorkee — 247667, India ACKNOWLEDGEMENT I take this opportunity to express my deep sense of gratitude to my respected guide Prof. R. K. Jain, Department of Architecture and Planning, Indian Institute of Technology Roorkee (Uttrakhand) for his constant encouragement, support and expert guidance throughout this work starting from choosing the topic. -

Future of Settlement On
MAP ---- WATER TREATMENT PLANTS- DELHI ---- FUTURE SOURCES OF RAW WATER FOR DELHI CONTENTS ---- SEWAGE TREATMENT PLANTS- DELHI ---- DRAINAGE SYSTEM IN DELHI Modified Planning & Implementation of NCR: ---- LANDFILL SITES - DELHI ---- NATIONAL CAPITAL REGION PROPOSED SETTLEMENT ---- STRATEGY FOR THE DEVELOPMENT OF POWER PATTERN 2021 SECTOR 1. INITIAL PLANNING OF NOIDA. ---- LIST OF PROPOSED POLICY BOXES 2. POWERS OF SOME OF THE SECTIONS OF NCR ACT ---- NATIONAL CAPITAL REGION REGIONAL -2001 : ONLY IN BRIEF CONSTITUENT AREAS 3. WHAT TO DO? ---- NATIONAL CAPITAL REGION REGIONAL -2021 : 4. COMPREHENSIVE PLANNING WILL INCLUDE THE CONSTITUENT AREAS FOLLOWING ACTIVITIES: (104 ITEMS) + SOME ITEMS ---- NATIONAL CAPITAL REGION PHYSIOGRAPHY AND MORE SLOPE 5. SOME IMPORTANT POLICY DECISIONS. ---- NATIONAL CAPITAL REGION LITHOLOGY ---- PHYSICAL GROWTH OF DELHI 1803-1959 & SEVEN- SEVENTEEN DELHIS ---- NATIONAL CAPITAL REGION GEOMORPHIC 6. NAMES OF NCR CITIES/TOWNS FOR THE YEAR 2011 AND ---- NATIONAL CAPITAL REGION GROUND WATER 2021 PROSPECTS I. Haryana ---- POLICY ZONES II. Rajasthan ---- EXISTING SETTLEMENT PATTERN 2001 III. Uttar Pradesh ---- EXISTING TRANSPORT NETWORK (Roads) 2002 7. PROJECTED POPULATION OF NCR CITIES / TOWNS FOR ---- EXISTING TRANSPORT NETWORK (Rail) 2002 THE YEAR 2031 ---- PROPOSED TRANSPORT NETWORK (ROADS) 2021 I. Haryana ---- PROPOSED TRANSPORT NETWORK (RAIL) 2021 II. Rajasthan ---- GROUND WATER RECHARGEABLE AREAS III. Uttar Pradesh ---- MASTER PLAN FOR NOIDA - 2021 ---- MASTER PLAN FOR GREATER NOIDA - 2021 MODIFIED PLANNING & IMPLEMENTATION OF: NCR 1. PRESENT AREA = 30242 SQ.KM. 2. PROPOSED AREA BY 2031 = ___SQ.KM. AFTER ADDING NEW DISTRICTS. 3. PRESENT POPULATION (2017) = ___ M UPS CAMPUS BLOCK-A, PREET VIHAR, 4. PREDICTED POPULATION (2031) = ___ M DELHI-92 (M) 09811018374 E-mail: [email protected] R.G.GUPTA www.rgplan.org, www.rgedu.org, www.uict.org City/Policy Planner NATIONAL CAPITAL REGION TO PREPARATION, ENFORCEMENT AND 5. -

Village Dasna P.S. Masuri, Gzb Mehrajuddin 9015499637 Village Shahpur, Dasna Gzb Mahi W/O Bhupende R 7011715175 Zafar Colony
CONTAINMENT ZONE INFORMATION OF DISTRICT GHAZIABAD Police Station Numb NAME OF Name of epi-centre PATIENT MOB. NO NO.OF CASES DATE OF SELLING Expected er of CONTAINMENT NAME Desealing Date ( Contai ZONE/ Hotspot if next 14 days nment Area no another Zone positive will be found) MASURI 1 DASNA ZONE VILLAGE DASNA P.S. MASURI, GZB MEHRAJUDDIN 9015499637 1 10-06-2020 20/10/2020 VILLAGE SHAHPUR, DASNA GZB MAHI W/O 7011715175 1 10-06-2020 20/10/2020 BHUPENDE R MASURI 2 MASURI ZAFAR COLONY NTPC ROAD MASURI FIZA CARE 9810565607 1 10-06-2020 20/10/2020 GZB GYASUDDI N MASURI 3 INDRA GARHI H.No - C-40 sadhbhawana nagar, madhu 8920007206 1 28/9/2020 10-11-2020 dasna, ghaziabad sharma FLAT NO 38, ROYAL GARDEN ARUN 9999145990 1 10-05-2020 19/10/2020 GANGAPURAM, GZB. KUMAR VILLAGE INDERGARHI NEAR PRIMARY DINESH S/O 9891843628 1 10-06-2020 20/10/2020 SCHOOL GZB PINTU MURADNAGA 4 MORTA VILLAGE SHAHPUR MORTA NEAR MONU 9899920787 1 10-09-2020 23/10/2020 R CANARA BANK GHAZIABAD SHARMA S/O SHIV MURADNAGA 5 DUHAI H.NO. 64 GARDEN ENCLAVE-II DUHAI REKHAKUMAR W/O 9560080539 1 10-08-2020 22/10/2020 R GZB ASHISH H.NO. 63, VILLAGE DUHAI, MEERUT RAKESH 7838413938 1 10-05-2020 19/10/2020 ROAD, GZB. TYAGI DEVANAND H.NO-85 MADHU VIHAR KHORA SHAH SON OF MADHU 1 9716453734 28-09-2020 11-10-2020 6 COLONY SEC-1 VAISHALI GZB DWARIKA VIHAR SAH 65 Madhu Vihar KHODA GZB 1 SIZARA DEVI 9319942744 28-09-2020 11-10-2020 2/80, GANG VIHAR, KHODA GANGA RADHA 7 COLONY GZB 2/80, GANG VIHAR, 1 9582322966 30-09-2020 14-10-2020 VIHAR MEHTA KHODA COLONY GZB G-222, DEEPAK VIHAR, KHORA DEEPAK 8 COLONY G-222, DEEPAK VIHAR, 1 SHANKER 9027993561 30-09-2020 14-10-2020 VIHAR KHORA COLONY RC-422 AZAD VIHAR KHODA 1 RAHUL JAIN 7011168893 10-06-2020 20-10-2020 COLONY GZB 9 AZAD VIHAR Rahul Jain RC 422, Azad Vihar, Khoda Colony 1 Son Lt. -

District Census Handbook, Ghaziabad, Part XIII-B, Series-22, Uttar Pradesh
CENSUS 1981 :illrr XIII - it ~/SERIES-22 ~T~q~ ~;=JlIUf~' ..... ~~< S(~ ~1~ 01"'TAR PRADESH Part XIII· B PRIMARY CENSUS ABSTRACT fir~T M~t mfijftlliltq ififqvrifT DISTRICT ~(l~(fCfif GHAZIABAD DISTRICT CENSUS HANDBOOK <:Cff;i ;rt(:'f,.. llrofR ~m~if<fi' ~~ .,film, iifiitlOlilT ~~, .-w, m I t. W€dIGl<t1 i-ii 2. Sf (l!fIrl!A' v-vi 3. ~fll1~ 4. ~~~ ix-xi S. ~~.u (~:!f~T CfiT qf"{"R .xiii-xv .6. f\iftVIT srr~ iiRq'1Jf;;r~ trTf{'(;:'lf ~W 10-17 7. atVJ;r.qd' ~l!T t ft;r{( smrfq<fi ijf"lljql;j lij I,{ 18-25 B. otl«f.qd' ~rfu'q) ~ fi;r~ 3lNfq<fl \J(1'l uI1Hfl <: 26-33 9. VTlftlJff~ \1Tlfrllifi i;f;;lf1JTrrr~T1: (6'Q:qr~T ~ iXT;ff allT ;rlT"{f ~ crri it; ~,) 33-207 1. ~m~ (i) ~ ifTiff~ (i i) ~'11 tift CfOrijlfifi \I:'ift 36-37 (iii) ~T"llJf smrf1fili ijf<t.1 01 .. mrt 40-55 (iV) i'f'if~ 5I'rqfllcw iif'iilT"T1Tm ~m ".I(qlr~iIi'T) 56-59 (v) ifTf~m ;;1T~!fiT <fi'T qftf~ 61-73 (vi) ~ srrqf~ifi GJ'ifif1lT;;rm"{ <UiifT1,(o'ifil1\'1'T it~~ aft< m~'{ ano iift'o) 74-75 (viiI 'tT3I'T-I' (lfi'm:rT ~~ ar~ ~'T;:pf'{) afto i>ft'o CfiT qf<NiiSi! 71 ,(viii) ;r1T'tP:r srrqf!{lfi 'iif1'l'J1lTifnn, (~~ ~~) 78-79 (ix) ~ ~1 ~m rfi'T qfUlIlGt 81 {x} 0{'1f"{"\'zr srr<TIqcp ijfi'flTORmf"{ (~IT'{ i'(1f'(q'Tf~1 82-83 (xO ~'l1T,{ ;rfl~qlf~1 'liT qf"U~ 84-87 (xii) i'f'q:f\'1f 5I'Tqfqcp ~;;qor;;rm ("q~ i~ «to ito) ~8-89 (xiii) i4f~ !,m «1'0 efto 'fiT qf~f~ 91 (xiv) ;;~ srrv.rf11ifi \J('iflfOTifmr, l~~'{ ;:rlr{tt Ir~CflI} 92-93 (xv) ~~1q.:(1T't i'f'~tqIFr.1Cfl"T Cfl"T qfdlllSt! 94-95 {~vi) illTtnt 'SIT nlfifi iif';lfar;;T~rrt (3flfi"if~ *,~I' 1!'tT'liflT'{) 96-97 (xvii) arrR'~ ~ ~if4ft 'tiT qfUlU'~ 99 (xviii) ;:r~ SfT1I'flAi ;;r",.,o,<tlijf'{ (<'I'TfI'TO{4f'{~) 100-101 (Xix) ~1';;tJ'{ ~ <tiT qftf~c 102-103 (XX) if1T~ srT~ ~rmrr, (qm;n iJ1T'( ~'!f) 104-105 {XXi) tRf~r;;q'{ ~ 'fiT qf'~:f'Q{q; 107 (XJtii) il~ ~fl{lfi '5I'~;rm'{ (~O{~ Q) 108-109 (XXiii) f~1' ij''l'{ ~er lfi'T q'f"U~e 111 2.