Root Cause Analysis for Fire Events at Nuclear Power Plants
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Fundamentals of Applied Smouldering Combustion
Western University Scholarship@Western Electronic Thesis and Dissertation Repository 6-20-2018 10:00 AM Fundamentals of Applied Smouldering Combustion Marco Zanoni The University of Western Ontario Supervisor Gerhard, Jason I. The University of Western Ontario Co-Supervisor Torero, Jose L. The University of Western Ontario Graduate Program in Civil and Environmental Engineering A thesis submitted in partial fulfillment of the equirr ements for the degree in Doctor of Philosophy © Marco Zanoni 2018 Follow this and additional works at: https://ir.lib.uwo.ca/etd Part of the Environmental Engineering Commons, and the Heat Transfer, Combustion Commons Recommended Citation Zanoni, Marco, "Fundamentals of Applied Smouldering Combustion" (2018). Electronic Thesis and Dissertation Repository. 5410. https://ir.lib.uwo.ca/etd/5410 This Dissertation/Thesis is brought to you for free and open access by Scholarship@Western. It has been accepted for inclusion in Electronic Thesis and Dissertation Repository by an authorized administrator of Scholarship@Western. For more information, please contact [email protected]. Abstract Smouldering combustion is defined as a flameless oxidation reaction occurring on the surface of the condensed phase (i.e., solid or liquid). Traditional research on smouldering was related to economic damages, fire risk, and death, due to the release of toxic gases and slow propagation rates. Recently, smouldering has been applied as an intentional, engineering technology (e.g., waste and contaminant destruction). Smouldering involves the transport of heat, mass, and momentum in the solid and fluid phases along with different chemical reactions. Therefore, numerical models are essential for the fundamental understanding of the process. Smouldering models either neglected heat transfer between phases (i.e., assumed local thermal equilibrium) or employed heat transfer correlations (i.e., under local thermal non- equilibrium conditions) not appropriate for smouldering. -
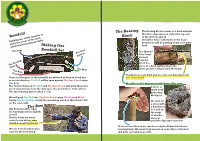
Bowdrill Block of the Drill Can Spin In
The Bearing The Bearing Block is made of a hard material that has a depression in it that the top end Bowdrill Block of the drill can spin in. It must be very comfortable in the hand Rubbing two sticks together to because we will be pushing down on it quite make fire is one of the mostMaking Our hard. quintessential bushcraft skills. Bowdrill Set The Bow In a Spruce/ The Coal Pine forest Catcher the best bearing block is a The Bearing piece of a dead sapling where the Block The Drill knots grow in a ring around the trunk. The Base Board The knots are very hard and we carve our depression into These are the parts of the bowdrill, we will look at them in detail but one of the knots. as an introduction: The Drill will be spun against The Base Board using The Bow. We lubricate the depression with Spruce/Pine resin. The friction between The Drill and The Base Board will grind them into A stone or wood dust and also heat the dust up to the point where it smoulders. shells work The smouldering dust is called a ‘coal’. as bearing blocks too. We will push The Drill into The Base Board using The Bearing Block. Finally The Coal Catcher holds the ground up wood so that doesn’t fall We look for on the cold earth. a stone with The Bow a depression Our Bow should be ridge in it and use (not springy) and be slightly the point curved. of another Shorter bows are much stone to easier to use but an arms grind the depression smooth. -

Test Report No
4417 Test Report No. AJFS2011010056FF Date: NOV.27, 2020 Page 1 of 4 ZHEJIANG ANJI RONGYI FURNITURE CO., LTD TANGPU INDUSTRY ZONE ANJI COUNTY ZHEJIANG The following sample(s) information was / were submitted and identified on behalf of the client. SGS is not responsible for the authenticity, integrity and results of the data and information and / or the validity of the conclusion arising therefrom. Results apply to the sample as received. Sample Description: MESH SGS Ref No.: AJHL2011500981OT Style/Item No.: / Test Requested: The Furniture and Furnishings (Fire) (Safety) Regulations 1988 S.I. No.1324 (amended 1989,1993 and 2010), Schedule 4, Part I, Cigarette test for cover fabrics and Schedule 5, Part I, Match test for cover fabrics. As specified in above standard(s) and incorporated with using ignition source 0 and 1 of BS 5852: Part 1:1979. Test Results: -- See attached sheet – Conclusion: The tested sample Meets the Requirements of Schedule 4 Part I and Schedule 5 Part I In Statutory Instrument 1988 No.1324 (Amended 1989, 1993 and 2010) the Furniture and Furnishings (Fire) (Safety) Regulations. Test Period: Sample Receiving Date : NOV.23, 2020 Test Performing Date : NOV.23, 2020 TO NOV.27, 2020 Signed for and on behalf of SGS-CSTC Co., Ltd. Anji Branch Allen Zou Lab Manager Test Report No. AJFS2011010056FF Date: NOV.27, 2020 Page 2 of 4 Test Conducted The Furniture and Furnishings (Fire) (Safety) Regulations 1988 S.I. No. 1324 (amended 1989, 1993 and 2010), Schedule 4 Part I and Schedule 5 Part I, Cigarette test and Match test for cover fabric. -

Fire Growth and Smoke Spread Model for Fire Safety System Design: Experimental Verification
Fire Growth and Smoke Spread Model for Fire Safety System Design: Experimental Verification M LUQ* and Y HE Center for Environmental Safety and Risk Engineering Victoria University of Technology 14428 MCMC, Melbourne, VIC 8001, Australia ABSTRACT A one-zone model (NRC C) and a two-zone model (CFAST) have been tested against experiments and used in the fire research community. However, the selection of either ofthem as a sub-model for a fire safety system model needs further verification against the experimental results under a variety of fire scenarios. In the present study, the performance of the above two models is evaluated with respect to accuracy, efficiency and simplicity. This study indicates that significant discrepancies exist between the experimental results and the results from both the CFAST model and the NRCC model. The CFAST model generally over-predicts the upper layer temperatures in the burn room but provides reasonable predictions in the adjacent enclosures. The CFAST model over-predicts CO concentrations when the air-handling system is turned on; the model under-predicts CO when the system is off. The NRCC model correlates the burning characteristics of the fuel with the burn room conditions. The results give a good agreement with the experimental results in the burn room for some fire scenarios but discrepancies exist for others. However, the NRCC fire model is applicable to the bum room only. It was found that the room-averaged temperatures for the bum room obtained from the CFAST model were in a good agreement with the experimental results and the NRCC model results. -

View Article
I THE LIBRARY r!f:~~·~~~·~~~ (I"'"',)) ...~. ,I!'!n .. - FIRE RESE.l\RGI STATION ~~.~~ ~~ ~~ I " 'I'1 . BOREHAM WOOD .11:: b \0 \; vf~~ . HERlS, .,.' CONFIDll'TIAL F.R. Note No. 48/1952., This report has not been published. and December, 1952. should be considered as confidential advance, information. No reference should be made to it in any publioation without, the written oonsent of the Direotor, Fire Research Station, Bareham Wood, Herts.' (Telephone: ELStree 1341 an~1797). ' DEI?.ARn!l!NT OF SCImTIFIC .AND nmUSTRIAL RF.SEARCH .AND FIRE OFFIClS' COMMITTEE JOINT FIRE RESEARCH ORGANIZATION SMOULDERING IN DUSTS AND FIBROUS MATERIALS PART V BEECH SAWDUST WITH AN INCIDliNT AIR IlRAUGHT by K.N. Palmer and M.D. Perry SUMMARY The effeot of an inoident airflow upon the smouldering of beech sawdust has been investigated in detail. The sawdust was fonned into small t:t~ains, as in earlier experiments tinder still-air oonditions, aild.placed in a small wind tunnel; smouldering was then' initiated by a small gas flame '~d the time of' travel over unit distance (smouldering time) was detennined. A'log'arithmio relationship was found betweeathe ~oulderingti.me arid, incident air velooity; the eff'edts of" variations in train size, sawdust particle size, and moisture content upon this relationship were comparatively slight. The' reduotion in the minimum depth of sawdust neoessary for suabadned smouldering was also invest~gated and it was shown that this depth could be reduced easily to .Leaa than 3 IIlIIlo by an inoident draught. ' , Some f'urther experdmenbs , desoribed in an AppenCi.ix, showed that flaming, could be produced in wood shavings or newspaper in contact with the smouldering sawdust and that only gentle airflows are neceasary, From these ,results it is concluded that an outbreak of fire could be a direot consequence, . -

Fire Fighting Controlled Burn-Offs
This Best Practice Guide is being reviewed. The future of Best Practice Guides will be decided during 2015. Best practice guidelines for Fire Fighting Controlled Burn-Offs V ision, knowledge, performance competenz.org.nz He Mihi Nga pakiaka ki te Rawhiti. Roots to the East. Nga pakiaka ki te Raki. Roots to the North. Nga pakiaka ki te Uru. Roots to the West. Nga pakiaka ki te Tonga. Roots to the South. Nau mai, Haere mai We greet you and welcome you. ki te Waonui~ o Tane To the forest world of Tane. Whaia te huarahi, Pursue the path, o te Aka Matua, of the climbing vine, i runga, I te poutama on the stairway, o te matauranga.~ of learning. Kia rongo ai koe So that you will feel, te mahana o te rangimarie.~ the inner warmth of peace. Ka kaha ai koe, Then you will be able, ki te tu~ whakaiti, to stand humbler, ki te tu~ whakahi.~ Yet stand proud. Kia Kaha, kia manawanui~ Be strong, be steadfast. Tena koutou katoa. First edition December 2000 Revised edition January 2005 These Best Practice Guidelines are to be used as a guide to certain fire-fighting and controlled burnoff procedures and techniques. They do not supersede legislation in any jurisdiction or the recommendations of equipment manufacturers. FITEC believes that the information in the guidelines is accurate and reliable; however, FITEC notes that conditions vary greatly from one geographical area to another; that a greater variety of equipment and techniques are currently in use; and other (or additional) measures may be appropriate in a given situation. -

The-Firewood-Poem (Congreve)
The Firewood Poem - Lady Celia Congreve Published in the Times: March 2nd 1930 These hardwoods burn well and slowly, Holly logs will burn like wax, Ash, beech, hawthorn oak and holly. You could burn them green. Softwoods flare up quick and fine, Elm logs burn like smouldering flax, Birch, fir, hazel, larch and pine. With no flame to be seen. Elm and willow you'll regret, Beech logs for winter time, Chestnut green and sycamore wet. Yew logs as well sir. Green elder logs it is a crime, Beechwood fires are bright and clear, For any man to sell sir. If the logs are kept a year. Chestnut's only good, they say, Pear logs and apple logs, If for long 'tis laid away. They will scent your room. But Ash new or Ash old, And cherry logs across the dogs, Is fit for a queen with crown of gold. They smell like flowers of broom. But Ash logs smooth and grey, Birch and fir logs bum too fast, Buy them green or old, sir. Blaze up bright and do not last. And buy up all that come your way, It is by the Irish said, They're worth their weight in gold sir. Hawthorn bakes the sweetest bread. Elm wood bums like churchyard mould, Logs to Burn, Logs to burn, Logs to burn, E'en the very flames are cold. Logs to save the coal a turn. But Ash green or Ash brown, Here's a word to make you wise, Is fit for a queen with golden crown. -

The Basis for Fire Safety Substantiating Fire Protection in Buildings
The Basis for Fire Safety Substantiating fire protection in buildings Fire Safety Professorship René Hagen and Louis Witloks The Basis for Fire Safety Substantiating fire protection in buildings 1 Publication Details Authors René Hagen and Louis Witloks, Fire Safety professorship of the Instituut Fysieke Veiligheid, in close cooperation with various research groups of Brandweer Nederland, the organisation of Dutch fire services. Photographs Cover photo: Jan Beets Inside photos: René Hagen, Martin de Jongh, Rob Jastrzebski, Jeroen Schokker, Wikimedia and Instituut Fysieke Veiligheid Translation Esperanto WBT Support This publication was also made possible by Underwriters Laboratories and European Fire Safety Alliance (EuroFSA). The knowledge document entitled ‘The Basis for Fire Safety’ was originally written on the basis of the Dutch situation, but in practice, it was soon found to be applicable to situations outside the Netherlands as well. The approach to fire safety as described and elaborated in this document can be applied universally. It describes the backgrounds and provides a substantiation of fire protection measures and facilities. And they also apply internationally, since fire development and fire growth are not specific to just one country. When using this publication for situations outside the Netherlands, please remember that the statistical details stated only concern the Netherlands. Where regulations are referred to, as is specifically the case in chapter 6, this is Dutch legislation. However, the book is definitely suitable for international use as its main focus is on the backgrounds and substantiation of fire safety measures and facilities which are based on fire development, the spread of smoke, the behaviour of constructions and people's behaviour when fleeing a building, instead of on statutory requirements. -
Selecting Design Fires
Selecting design fires Staffansson, Leif 2010 Link to publication Citation for published version (APA): Staffansson, L. (2010). Selecting design fires. Department of Fire Safety Engineering and Systems Safety, Lund University. Total number of authors: 1 General rights Unless other specific re-use rights are stated the following general rights apply: Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal Read more about Creative commons licenses: https://creativecommons.org/licenses/ Take down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. LUND UNIVERSITY PO Box 117 221 00 Lund +46 46-222 00 00 Selecting design fires Leif Staffansson Department of Fire Safety Engineering and Systems Safety Lund University, Sweden Brandteknik och Riskhantering Lunds tekniska högskola Lunds universitet Report 7032 Lund 2010 Selecting design fires Leif Staffansson Lund 2010 Selecting design fires Leif Staffansson Report 7032 ISSN: 1402-3504 ISRN: LUTVDG/TVBB--7032--SE Number of pages: 105 Illustrations: Leif Staffansson Keywords Design fires, fire characteristics, heat release rate, deterministic analysis. -

Self-Sustaining Smouldering Combustion As a Waste Treatment Process Treatment Process
ProvisionalChapter chapter 6 Self-sustaining Smouldering Combustion as a Waste Treatment Process Treatment Process Luis Yermán Luis Yermán Additional information is available at the end of the chapter Additional information is available at the end of the chapter http://dx.doi.org/10.5772/64451 Abstract This chapter reviews the utilization of self-sustaining smouldering combustion as a treatment for solid or liquid waste, embedded in a porous matrix. Smouldering has been identified as an attractive solution to treat waste with high moisture content. The fundamental aspects of this technology, such as the experimental setup and the ignition mechanism, are described here. The operational parameters determine the physical properties of the media, and will dictate the self-sustainability of the process. A discussion on how the operational parameters affect the smouldering performance is also presented. The performance of smouldering is usually assessed by the peak temperatures and the velocity of propaga‐ tion of the smouldering front through the material. The potential sources for energy recovery are described. Importantly, as oxidation and pyrolysis coexist during smouldering, it was shown with potential for the recovery of pyrolysis products, such as pyrolysis oil. Finally, a brief insight on the gas emissions, and the perspectives regarding the technoeconomic viability in full-scale are also discussed. Keywords: smouldering combustion, self-sustaining, waste treatment, energy recov‐ ery, review 1. Introduction Smouldering is a complex process that involves heat and mass transfer in porous media, heterogeneous reactions at the solid/gas pore interface, thermochemistry and chemical kinetics [1]. It has been historically studied from a fire safety perspective because it represents a fire © 2016 The Author(s). -

Fire Drill Procedure 35 Purpose Procedure Conducting a Fire Drill Conducting a Silent Fire Drill Observations Debriefing
FIRE MARSHAL’S MANUAL A Resource for Healthcare Fire Marshal’s Fire Marshal‟s Manual Alberta Health Services Fire and Life Safety Version 3.0 Revised October 2013 Capital Management, Protective Services Overview A safe environment is an integral part of our patient focused quality health care system. AHS Protective Services is responsible for Fire and Life Safety (FLS) within our facilities throughout the province. Our mandate is to meet or exceed the guidelines and requirements of the Alberta Building and Fire Codes. A Fire Marshal and an Emergency Response Plan is mandatory for each facility and this manual is designed to provide guidance and education to designated Fire Marshal‟s. Protective Services Fire and Life Safety will provide Governance, Education and be a Resource to address and advise any fire safety concerns. Fire Marshal‟s Manual Alberta Health Services Fire and Life Safety Version 3.0 Revised October 2013 Capital Management, Protective Services Table of Contents Definitions 4 Section 1: Introduction Healthcare Fire Marshal Responsibilities 6 Owner/Operator Responsibilities 7 Employee Responsibilities 8 General Fire Safety Rules 9 Section 2: Emergency Codes 11 Section 3: Fire Inspection of the Facility Conducting Inspections 16 Semi-Annual Building Inspections Common Hazards Documentation Monthly Inspection of Portable Fire Extinguishers 18 Monthly Inspection of Fire Hoses 18 Self-contained Emergency Lighting Units (Battery Packs) 19 Monthly Inspection of Fire Separation Doors 19 Monthly Inspections of Fixed Kitchen Systems -

The Smouldering of Peat
THE SMOULDERING OF PEAT A thesis submitted to the University of Manchester for the degree of Doctor of Philosophy in the Faculty of Engineering and Physical Sciences 2013 Kathleen Scott School of Mathematics Contents Abstract 5 Declaration 6 Copyright Statement 7 Acknowledgements 8 1 Introduction and Background 11 1.1 OverviewofWildfires .............................. 11 1.2 PeatCharacteristicsandPeatfires . .... 13 1.3 The Physics and Chemistry of Combustion . ... 17 1.4 Characteristics of Smouldering Combustion . ....... 19 1.5 CombustionInstabilities . ... 21 1.6 Other forms of Smouldering Combustion . .... 23 1.7 TheCurrentContributions . .. 25 2 Literature Review 27 2.1 Experimental Studies of Peat Combustion . ..... 27 2.2 KineticSchemes ................................. 34 2.3 ReactionRateLaws ............................... 37 2.4 Models of Smouldering Combustion . ... 39 2.5 Instabilities and Low Lewis Number Combustion . ...... 42 3 The Mathematical Model 45 3.1 TheProblem ................................... 45 3.2 TheModel..................................... 46 2 3.3 Non-dimensionalising the Model . .... 49 4 Spherically Symmetrical Combustion 55 4.1 Introduction.................................... 55 4.2 Solid Consumption Tending to 0 . 58 4.2.1 AnalyticalSolutions. 59 4.2.2 Superadiabatic Numerical Solution . ... 63 4.2.3 Adiabatic Numerical Solution . 67 4.3 Incomplete Solid Combustion . .. 71 4.3.1 AnalyticalSolutions. 72 4.3.2 Superadiabatic Numerical Solution . ... 74 4.3.3 Adiabatic Numerical Solution . 75 4.3.4 Cylindrically Symmetrical Numerical Solution . ...... 77 4.4 Conclusions .................................... 79 5 Combustion with an Imposed Gas Velocity 80 5.1 Introduction.................................... 80 5.2 The Travelling Wave Model . 81 5.2.1 Identifying a Travelling Wave Solution . ... 81 5.2.2 Profiles of the Travelling Wave Solution . ... 86 5.3 TheEffectsofHeatLoss ............................ 89 5.4 TheEffectsofGasVelocity.