BCMA-Targeted Immunotherapy for Multiple Myeloma Bo Yu1, Tianbo Jiang2 and Delong Liu2*
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

BAFF-Neutralizing Interaction of Belimumab Related to Its Therapeutic Efficacy for Treating Systemic Lupus Erythematosus
ARTICLE DOI: 10.1038/s41467-018-03620-2 OPEN BAFF-neutralizing interaction of belimumab related to its therapeutic efficacy for treating systemic lupus erythematosus Woori Shin1, Hyun Tae Lee1, Heejin Lim1, Sang Hyung Lee1, Ji Young Son1, Jee Un Lee1, Ki-Young Yoo1, Seong Eon Ryu2, Jaejun Rhie1, Ju Yeon Lee1 & Yong-Seok Heo1 1234567890():,; BAFF, a member of the TNF superfamily, has been recognized as a good target for auto- immune diseases. Belimumab, an anti-BAFF monoclonal antibody, was approved by the FDA for use in treating systemic lupus erythematosus. However, the molecular basis of BAFF neutralization by belimumab remains unclear. Here our crystal structure of the BAFF–belimumab Fab complex shows the precise epitope and the BAFF-neutralizing mechanism of belimumab, and demonstrates that the therapeutic activity of belimumab involves not only antagonizing the BAFF–receptor interaction, but also disrupting the for- mation of the more active BAFF 60-mer to favor the induction of the less active BAFF trimer through interaction with the flap region of BAFF. In addition, the belimumab HCDR3 loop mimics the DxL(V/L) motif of BAFF receptors, thereby binding to BAFF in a similar manner as endogenous BAFF receptors. Our data thus provides insights for the design of new drugs targeting BAFF for the treatment of autoimmune diseases. 1 Department of Chemistry, Konkuk University, 120 Neungdong-ro, Gwangjin-gu, Seoul 05029, Republic of Korea. 2 Department of Bio Engineering, Hanyang University, 222 Wangsimni-ro, Seongdong-gu, Seoul 04763, Republic of Korea. These authors contributed equally: Woori Shin, Hyun Tae Lee, Heejin Lim, Sang Hyung Lee. -

Clinical Policy: Baricitinib (Olumiant) Reference Number: ERX.SPA.291 Effective Date: 07.24.18 Last Review Date: 11.18 Revision Log
Clinical Policy: Baricitinib (Olumiant) Reference Number: ERX.SPA.291 Effective Date: 07.24.18 Last Review Date: 11.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal information. Description Baricitinib (Olumiant®) is Janus kinase (JAK) inhibitor. FDA Approved Indication(s) Olumiant is indicated for the treatment of adult patients with moderately to severely active rheumatoid arthritis (RA) who have had an inadequate response to one or more tumor necrosis factor (TNF) antagonist therapies. Limitation(s) of use: Use of Olumiant in combination with other JAK inhibitors, biologic disease-modifying antirheumatic drugs (DMARDs), or with potent immunosuppressants such as azathioprine and cyclosporine is not recommended. Policy/Criteria Provider must submit documentation (such as office chart notes, lab results or other clinical information) supporting that member has met all approval criteria. It is the policy of health plans affiliated with Envolve Pharmacy Solutions™ that Olumiant is medically necessary when the following criteria are met: I. Initial Approval Criteria A. Rheumatoid Arthritis (must meet all): 1. Diagnosis of RA; 2. Prescribed by or in consultation with a rheumatologist; 3. Age ≥ 18 years; 4. Member meets one of the following (a or b): a. Failure of a ≥ 3 consecutive month trial of methotrexate (MTX) at up to maximally indicated doses, unless contraindicated or clinically significant adverse effects are experienced; b. If intolerance or contraindication to MTX (see Appendix D), failure of a ≥ 3 consecutive month trial of at least ONE conventional DMARD (e.g., sulfasalazine, leflunomide, hydroxychloroquine) at up to maximally indicated doses, unless contraindicated or clinically significant adverse effects are experienced; 5. -

Immunosuppressant Drugs Therapy with COVID-19
Immunosuppressant Drugs Therapy with COVID-19: Associated Risks, Drug-Drug Interactions & Contraindications Debjyoti Talukdar1, Diane Ignacio2, and Madan Mohan Gupta2 1Teerthanker Mahaveer University 2The University of the West Indies at St Augustine September 24, 2020 Abstract Immunosuppressant drugs like Etanercept, Mycophenolate mofetil, Sirolimus, Cyclosporine and Rituximab can weaken the immune system and make patients susceptible to SARS nCoV-2 virus. These drugs make immunocompromised persons more vulnerable to complications associated with COVID-19. Moreover, it can also increase the mortality and morbidity, as a weakened immune system can lead to longer duration of infection. This study discusses the guidelines on immunosuppressant drugs and its associated risk factors with COVID-19, issued by the U.S CDC (Centers for Disease Control and Prevention), WHO (World Health Organisation), U.S FDA (Food and Drug Administration) and other accredited global health organisa- tions. Moreover, it also includes information about pharmaceutical properties, mechanism of action, COVID-19 associated risk factors, adverse drug reactions, contraindications and drug-drug interactions. Our study will help government partners and international health organisations to better understand COVID-19 health risks associated with immunosuppressants. Increased public awareness about effective drug therapy for autoimmune diseases, cancer treatment, immunocompromised and organ transplant patients will help lower the mortality and morbidity associated with the disease amid COVID-19 pandemic. 1. INTRODUCTION As per the U.S Department of Health and Human Services and U.S FDA, immunosuppressant drugs can cause susceptibility to viruses leading to infection with increase in morbidity of the disease. It can cause severe risk of illness from COVID-19 due to a weakened immune system. -

Benlysta® (Belimumab)
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2021 P 1227-6 Program Prior Authorization/Notification Medication Benlysta® (belimumab)* *This program applies to the subcutaneous formulation of belimumab P&T Approval Date 9/2017, 9/2018, 9/2019, 9/2020, 2/2021, 7/2021 Effective Date 10/1/2021; Oxford only: 10/1/2021 1. Background: Benlysta® is a B-lymphocyte stimulator (BLyS)-specific inhibitor indicated for the treatment of patients aged 5 years and older with active, autoantibody-positive, systemic lupus erythematosus (SLE) who are receiving standard therapy and adult patients with active lupus nephritis who are receiving standard therapy. Limitations of Use: The efficacy of Benlysta has not been evaluated in patients with severe active central nervous system lupus. Benlysta has not been studied in combination with other biologics. Use of Benlysta is not recommended in these situations. 2. Coverage Criteria: A. Systemic Lupus Erythematosus 1. Initial Authorization a. Benlysta will be approved based on all of the following criteria: (1) Diagnosis of systemic lupus erythematosus -AND- (2) Laboratory testing has documented the presence of autoantibodies [e.g., ANA, Anti-dsDNA, Anti-Sm, Anti-Ro/SSA, Anti-La/SSB] -AND- (3) Patient is currently receiving standard immunosuppressive therapy [e.g., hydroxychloroquine, chloroquine, prednisone, azathioprine, methotrexate] -AND- (4) Patient does not have severe active central nervous system lupus -AND- (5) Patient is not receiving Benlysta in combination with either of the following: (a) Biologic DMARD [e.g., Enbrel (etanercept), Humira (adalimumab), Cimzia (certolizumab), Kineret (anakinra)] © 2021 UnitedHealthcare Services, Inc. 1 (b) Lupkynis (voclosporin) Authorization will be issued for 12 months. -

Attachment: Extract from Clinical Evaluation: Etanercept
AusPAR Attachment 2 Extract from the Clinical Evaluation Report for etanercept Proprietary Product Name: Erelzi Sponsor: Novartis Pharmaceuticals Australia Pty Ltd First round report: June 2017 Second round report: August 2017 Therapeutic Goods Administration About the Therapeutic Goods Administration (TGA) · The Therapeutic Goods Administration (TGA) is part of the Australian Government Department of Health and is responsible for regulating medicines and medical devices. · The TGA administers the Therapeutic Goods Act 1989 (the Act), applying a risk management approach designed to ensure therapeutic goods supplied in Australia meet acceptable standards of quality, safety and efficacy (performance) when necessary. · The work of the TGA is based on applying scientific and clinical expertise to decision- making, to ensure that the benefits to consumers outweigh any risks associated with the use of medicines and medical devices. · The TGA relies on the public, healthcare professionals and industry to report problems with medicines or medical devices. TGA investigates reports received by it to determine any necessary regulatory action. · To report a problem with a medicine or medical device, please see the information on the TGA website <https://www.tga.gov.au>. About AusPARs · An Australian Public Assessment Report (AusPAR) provides information about the evaluation of a prescription medicine and the considerations that led the TGA to approve or not approve a prescription medicine submission. · AusPARs are prepared and published by the TGA. · An AusPAR is prepared for submissions that relate to new chemical entities, generic medicines, major variations and extensions of indications. · An AusPAR is a static document; it provides information that relates to a submission at a particular point in time. -

Heart Failure and Drug-Induced Lupus
Unusual toxicities with TNF inhibition: Heart failure and drug-induced lupus J.J. Cush John J. Cush, MD, Chief, Rheumatology ABSTRACT demyelinating disease, cytopenias, auto- and Clinical Immunology, Presbyterian Serious and unexpected adverse events, immune disorders, and heart failure. Hospital of Dallas, Clinical Professor of such as heart failure and drug-induced Other essays in this volume address the Internal Medicine, The University of Texas lupus, have been reported in patients subject of infection (10), demyelination Southwestern Medical School, Dallas, Texas, USA. receiving TNF inhibitor therapy. These (11), and lymphoma (12). This review events generally are easily recogniz- will focus on heart failure and lupus- Please address correspondence to: John J. Cush, MD, Presbyterian Hospital able, although they cannot be predicted like disease, which are rarely seen in of Dallas, 8200 Walnut Hill Lane, Dallas, nor avoided, other than by drug avoid- association with TNF inhibitor therapy Texax 75231-4496, USA. ance altogether. Many patients have and are currently without explanation. Clin Exp Rheumatol 2004; 22 (Suppl. 35): great benefit from anti-TNF therapies. S141-S147. Their intelligent use requires a firm Sources of data © Copyright CLINICAL AND EXPERIMENTAL understanding of these rare toxicities, As a consequence of drug approval, RHEUMATOLOGY 2004. so as to minimize the morbidity associ- manufacturers have a responsibility to ated with their uncommon occurrence. collect safety data actively and report Key words: TNF inhibitors, conges- these data to the appropriate agencies. tive heart failure, drug-induced lupus, Introduction For example, in the USA a manufactur- rheumatoid arthritis. The introduction of biologic agents to er must submit periodic safety reports specifically inhibit the pro-inflammato- to the FDA twice yearly (March and ry cytokine, tumor necrosis factor (TNF), September). -

New Biological Therapies: Introduction to the Basis of the Risk of Infection
New biological therapies: introduction to the basis of the risk of infection Mario FERNÁNDEZ RUIZ, MD, PhD Unit of Infectious Diseases Hospital Universitario “12 de Octubre”, Madrid ESCMIDInstituto de Investigación eLibraryHospital “12 de Octubre” (i+12) © by author Transparency Declaration Over the last 24 months I have received honoraria for talks on behalf of • Astellas Pharma • Gillead Sciences • Roche • Sanofi • Qiagen Infections and biologicals: a real concern? (two-hour symposium): New biological therapies: introduction to the ESCMIDbasis of the risk of infection eLibrary © by author Paul Ehrlich (1854-1915) • “side-chain” theory (1897) • receptor-ligand concept (1900) • “magic bullet” theory • foundation for specific chemotherapy (1906) • Nobel Prize in Physiology and Medicine (1908) (together with Metchnikoff) Infections and biologicals: a real concern? (two-hour symposium): New biological therapies: introduction to the ESCMIDbasis of the risk of infection eLibrary © by author 1981: B-1 antibody (tositumomab) anti-CD20 monoclonal antibody 1997: FDA approval of rituximab for the treatment of relapsed or refractory CD20-positive NHL 2001: FDA approval of imatinib for the treatment of chronic myelogenous leukemia Infections and biologicals: a real concern? (two-hour symposium): New biological therapies: introduction to the ESCMIDbasis of the risk of infection eLibrary © by author Functional classification of targeted (biological) agents • Agents targeting soluble immune effector molecules • Agents targeting cell surface receptors -

(CS-ⅣA-Be), a Novel IL-6R Antagonist, Inhibits IL-6/STAT3
Author Manuscript Published OnlineFirst on February 29, 2016; DOI: 10.1158/1535-7163.MCT-15-0551 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Chikusetsusaponin Ⅳa butyl ester (CS-Ⅳa-Be), a novel IL-6R antagonist, inhibits IL-6/STAT3 signaling pathway and induces cancer cell apoptosis Jie Yang 1, 2, Shihui Qian 2, Xueting Cai 1, 2, Wuguang Lu 1, 2, Chunping Hu 1, 2, * Xiaoyan Sun1, 2, Yang Yang1, 2, Qiang Yu 3, S. Paul Gao 4, Peng Cao 1, 2 1. Affiliated Hospital of Integrated Traditional Chinese and Western Medicine, Nanjing University of Chinese Medicine, Nanjing 210028, China 2. Laboratory of Cellular and Molecular Biology, Jiangsu Province Academy of Traditional Chinese Medicine, Nanjing 210028, China 3. Shanghai Institute of Materia Medical, Chinese Academy of Sciences, Shanghai, 201203, China 4. Human Oncology and Pathogenesis Program, Memorial Sloan-Kettering Cancer Center, New York, NY10065, USA Running title: CS-Ⅳa-Be, a novel IL-6R antagonist, inhibits IL-6/STAT3 Keywords: Chikusetsusaponin Ⅳ a butyl ester (CS- Ⅳ a-Be), STAT3, IL-6R, antagonist, cancer Grant support: P. Cao received Jiangsu Province Funds for Distinguished Young Scientists (BK20140049) grant, J. Yang received National Natural Science Foundation of China (No. 81403151) grant, and X.Y. Sun received National Natural Science Foundation of China (No. 81202576) grant. Corresponding author: Peng Cao Institute: Laboratory of Cellular and Molecular Biology, Jiangsu Province Academy of Traditional Chinese Medicine, Nanjing 210028, Jiangsu, China Mailing address: 100#, Shizi Street, Hongshan Road, Nanjing, Jiangsu, China Tel: +86-25-85608666 Fax: +86-25-85608666 Email address: [email protected] The first co-authors: Jie Yang and Shihui Qian The authors disclose no potential conflicts of interest. -
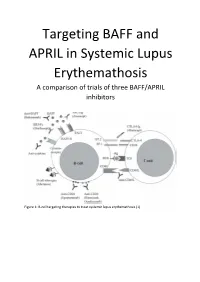
Targeting BAFF and APRIL in Systemic Lupus Erythemathosis a Comparison of Trials of Three BAFF/APRIL Inhibitors
Targeting BAFF and APRIL in Systemic Lupus Erythemathosis A comparison of trials of three BAFF/APRIL inhibitors Figure 1: B-cell targeting therapies to treat systemic lupus erythemathosis (1) Abstract: Systemic Lupus Erythemathosis (SLE) is a complex autoimmune disease. Diagnosis and prognosis are difficult and have a lot of confounders. Progress of the disease is thus followed by a number of measures, such as damage indices like SELENA/SLEDAI and BILAG, B-cell numbers, immunoglobulin levels, in particular autoantibodies such as anti-dsDNA antibodies, and complement C3 and C4 levels. B-cell proliferation and activation are overstimulated in SLE, particularly through the BAFF/APRIL stimulated pathways. A number of BAFF/APRIL targeting biologicals have been approved for use in treatment of SLE or are currently in clinical trials. Three of these are highlighted here: Belimumab, Blisibimod and Atacicept. Belimumab, a fully humanized anti-BAFF antibody, is already approved by the USFDA. In clinical studies it has been show to lower the damage index, B-cell numbers and immunoglobulin levels, it increases complement levels and may reduce the need for steroids. Blisibimod, a synthetic peptibody, is in stage II trials. Like Belimumab, Blisbimod lowers the damage index and B-cell numbers, increases complement levels and may reduce the need for steroids. Ataticept, a fusion protein, is in stage III trials. Atacicept also lowers the damage index, B-cell numbers and immunoglobulin levels, increases complement and may reduce the need for steroids. The differences are relatively small and to determine the most promising of these treatments close attention has to be paid to the data from trials. -

An Update on the Current State of Management and Clinical Trials for Iga Nephropathy
Journal of Clinical Medicine Review An Update on the Current State of Management and Clinical Trials for IgA Nephropathy Chee Kay Cheung 1,2 , Arun Rajasekaran 3 , Jonathan Barratt 1,2,† and Dana V. Rizk 3,*,† 1 Department of Cardiovascular Sciences, University of Leicester, Leicester LE1 7RH, UK; [email protected] (C.K.C.); [email protected] (J.B.) 2 John Walls Renal Unit, University Hospitals of Leicester NHS Trust, Leicester LE5 4PW, UK 3 Division of Nephrology, Department of Medicine, University of Alabama at Birmingham, ZRB 614, 1720 2nd Avenue South, Birmingham, AL 35294, USA; [email protected] * Correspondence: [email protected] † Both authors contributed equally to this work. Abstract: IgA nephropathy remains the most common primary glomerular disease worldwide. It affects children and adults of all ages, and is a leading cause of end-stage kidney disease, making it a considerable public health issue in many countries. Despite being initially described over 50 years ago, there are still no disease specific treatments, with current management for most patients being focused on lifestyle measures and renin-angiotensin-aldosterone system blockade. However, significant advances in the understanding of its pathogenesis have been made particularly over the past decade, leading to great interest in developing new therapeutic strategies, and a significant rise in the number of interventional clinical trials being performed. In this review, we will summarise the current state of management of IgAN, and then describe major areas of interest where new therapies are at their most advanced stages of development, that include the gut mucosal immune system, B cell signalling, the complement system and non-immune modulators. -

The Future of B-Cell Activating Factor Antagonists in the Treatment of Systemic Lupus Erythematosus
pISSN: 2093-940X, eISSN: 2233-4718 Journal of Rheumatic Diseases Vol. 24, No. 2, April, 2017 https://doi.org/10.4078/jrd.2017.24.2.65 Review Article The Future of B-cell Activating Factor Antagonists in the Treatment of Systemic Lupus Erythematosus William Stohl Division of Rheumatology, Department of Medicine, University of Southern California Keck School of Medicine, Los Angeles, CA, USA To review B-cell activating factor (BAFF)-antagonist therapy in systemic lupus erythematosus (SLE), literature was searched us- ing the search words and phrases, “BAFF”, “B lymphocyte stimulator (BLyS)”, “a proliferation-inducing ligand (APRIL)”, “B-cell maturation antigen (BCMA)”, “transmembrane activator and calcium-modulating and cyclophilin ligand interactor (TACI)”, “BLyS receptor 3 (BR3)”, “belimumab”, “atacicept”, “blisibimod”, “tabalumab”, and “lupus clinical trial”. In addition, papers from the author’s personal library were searched. BAFF-antagonist therapy in SLE has a checkered past, with four late-stage clin- ical trials meeting their primary endpoints and four failing to do so. Additional late-stage clinical trials are enrolling subjects to address some of the remaining unresolved questions, and novel approaches are proposed to improve results. The BAFF-centric pathway is a proven therapeutic target in SLE. As the only pathway in the past 50+ years to have yielded an United States Food and Drug Administration-approved drug for SLE, it occupies a unique place in the armamentarium of the practicing rheumatologist. The challenges facing clinicians and investigators are how to better tweak the BAFF-centric pathway and im- prove on the successes realized. (J Rheum Dis 2017;24:65-73) Key Words. -

BAFF Suppresses IL-15 Expression in B Cells
BAFF Suppresses IL-15 Expression in B Cells Ning Ma, Chen Xing, He Xiao, Youdi He, Gencheng Han, Guojiang Chen, Chunmei Hou, Bernadette Marrero, Yujuan Wang, Shengquan Zhang, Beifen Shen, Yan Li and Renxi This information is current as Wang of September 28, 2021. J Immunol 2014; 192:4192-4201; Prepublished online 26 March 2014; doi: 10.4049/jimmunol.1302132 http://www.jimmunol.org/content/192/9/4192 Downloaded from Supplementary http://www.jimmunol.org/content/suppl/2014/03/26/jimmunol.130213 Material 2.DCSupplemental http://www.jimmunol.org/ References This article cites 39 articles, 14 of which you can access for free at: http://www.jimmunol.org/content/192/9/4192.full#ref-list-1 Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision by guest on September 28, 2021 • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology BAFF Suppresses IL-15 Expression in B Cells Ning Ma,*,†,1 Chen Xing,*,1 He Xiao,*,1 Youdi He,‡ Gencheng Han,* Guojiang Chen,* Chunmei Hou,* Bernadette Marrero,x Yujuan Wang,{ Shengquan Zhang,‖ Beifen Shen,* Yan Li,* and Renxi Wang* Clinical trials have shown that BAFF inhibitors do not reduce memory B cell levels but can reduce the number of mature B cells.