Community Definitions of Violence and GBV
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mental Health in Donetsk and Luhansk Oblasts - 2018
Mental health in Donetsk and Luhansk oblasts - 2018 1 Content List of abbreviations....................................................................................................................................... 3 1. INTRODUCTION ...................................................................................................................................... 4 2. METHODOLOGY OF THE RESEARCH ....................................................................................................... 6 3. RESUME .................................................................................................................................................. 8 4. RECOMMENDATIONS BASED ON THE FINDINGS OF THE RESEARCH .................................................. 13 5. PREVALENCE OF MENTAL HEALTH PROBLEMS AMONG THE PEOPLE LIVING IN DONETSK AND LUHANSK OBLASTS ...................................................................................................................................... 16 А. Detecting the traumatic experience .................................................................................................... 16 B. Prevalence of symptoms of PTSD, depression, anxiety disorder, excess alcohol consumption. ........ 18 C. Prevalence of mental health problems among the inner circle of the respondents .......................... 27 D. Indicators of mental well-being .......................................................................................................... 27 6. ACCESS TO ASSISTANCE WHEN SUFFERING FROM -

Ukraine Humanitarian Snapshot
UKRAINE CROSSING POINTS - Snapshot: July 2021 Despite the 15.5 per cent increase in civilian movement across the “contact line” in July compared to June (97,000 vs. 82,000), the number of civilian crossings remains low, representing just 7.5 per cent of 1.3 million crossings recorded in July 2019. Since the movement across the “contact line” remains limited to certain categories of people, 212,471 individuals, manyof whom are likely residents of non-Government-controlled areas (NGCA), opted to transit through the Russian Federation via the crossing points (CPs) “Milove” (Luhanska oblast) and “Hoptivka” (Kharkivska oblast) to enter Government-controlled areas (GCA) in July. However, the limited capacity of these border crossing points and long processing times are reported to have resulted in people spending up to 24 hours to cross to GCA. OPERATIONAL UPDATES ENTRY/EXIT CROSSING POINTS (EECPs) MAP EECP KEY FIGURES (July 2021) On 22 July, the President signed a law cancelling administrative fines for crossing the uncontrolled section of the Ukrainian-Russian border to transit to GCA from NGCA.¹ Following the entry into force of this law, NGCA Legend Number of ‘contact line’ 'Contact line' as of August 2018 residents will no longer be required to pay these fines at “Milove” and “Hoptivka” crossing points while COVID-19 ≈ k crossings by people Planned EECP 97 restrictions are in place provided that their justification for crossing falls under certain humanitarian exemptions.² Non-operational EECP While the law provides the possibility for the State Border Guard Service to exempt a person from paying a fine on Number of ‘contact line’ other grounds, reportedly, it hasn't been applied consistently to date. -

GBV Sub-Cluster Joint Action Plan 2019
GBV Sub-Cluster Joint Action Plan 2019 Priorities Activities Priority 1. Coordination to strengthen protection of GBV survivors and foster multisectoral response 1.1.1 Joint multisectoral initiatives are implemented based on the unififed framework, coordination mechanisms are functional and coordinated (adjusted) 1.1.2 Mapping/updates of GBV services (health care, PSS, legal) available regularly 1.1. Coordination of GBV multisectoral response 1.1.3 Technical/expert support to work out and implement policies on GBV MSR with regard to international standards 1.1.4 Accountability to affected population is in place 1.2.1 Roundtables/workshops/trainings/other learning solutions for representatives of respective bodies including civil society/community/media continued to be organized 1.2 Strengthening capacities of GBV MSR respective 1.2.2 Advocacy initiatives/bilateral and multilateral meetings conducted regularly on GBV prevention bodies and c coordinators and response 1.2.3 Sensitizing the community to GBV issues, enabling zero tolerance to GBV 1.3.1 Information materials on GBV/referrals/available services continued to be developed, updated, published and distributed to vulnerable population and respective bodies 1.3 Awareness raising and information campaigns 1.3.2 Roundtable discussions for civil society/community/media representatives continued to be organized 1.3.3 16 Days of Activism against Gender-based Violence Priority 2. Life-saving services for GBV survivors are available with regard to Humanitarian-Development Nexus 2.1.1 Psychosocial -

(CONSULTING SERVICES – FIRMS SELECTION) UKRAINE ROAD SECTOR DEVELOPMENT PROJECT Loan No.: 8549-UA
REQUEST FOR EXPRESSIONS OF INTEREST (CONSULTING SERVICES – FIRMS SELECTION) UKRAINE ROAD SECTOR DEVELOPMENT PROJECT Loan No.: 8549-UA Assignment Title: Consultancy Services for design and bidding documents elaboration for repair (rehabilitation) of the road R-66 KPP “Demyno-Oleksandrivka”-Svatove-Lysychansk-Luhansk sections km 30+000 – km 86+600, km 93+400 – km 145+075 and the road N-26 Chuguyiv-Milove section: km 136+000 – km 148+000 and T-13-02 KPP “Tanyushivka”-Starobilsk-Bahmut section km 76+000 – km 121+400. Reference No.: CS-23 BACKGROUND The State Road Agency of Ukraine (Ukravtodor) has received financing from the World Bank (“Bank”) toward the cost of the Road Sector Development Project and intends to apply part of the proceeds for consulting services. PURPOSE OF ASSIGNMENT The key objective is to undertake engineering surveys, design, preparation of bidding documents and cost estimate for repair (rehabilitation) of the road R-66 KPP “Demyno-Oleksandrivka”-Svatove- Lysychansk-Luhansk sections km 30+000 – km 86+600 (56.6 km in length), km 93+400 – km 145+075 (51.7 km in length) and the road N-26 Chuguyiv-Milove section: km 136+000 – km 148+000 (12 km in length) and T-13-02 KPP “Tanyushivka”-Starobilsk-Bahmut section km 76+000 – km 121+400 (45.4 km in length). The main tasks are divided into phases with the continuation of the Consultant’s appointment to carry out a subsequent phase is dependent on the Consultant’s satisfactory performance in carrying out the services under the previous phase/s. • Phase I: development of the design -

Sievierodonetsk (Luhansk Oblast) 18 June 2015
General Coordination Meeting – Sievierodonetsk (Luhansk Oblast) 18 June 2015 Discussion Action Points/Decisions 1. Summary of steps taken based on decisions of the previous meeting by UN OCHA OCHA to follow up on the implications of new Temporary Order of entry/exit to NGCAs for humanitarian cargo UN OCHA summarized activities based on the decisions of the last General Coordination Meeting. The movement. issue of unaccompanied minors is being addressed both at oblast and national levels. WHO keeps checking if tuberculin was delivered to all raions of the oblast. For the moment, it is confirmed that Bilovodsk, Milove and Markivka raions and Lysychansk didn’t receive it. WHO and UN OCHA had the meetings with the authorities in Bilovodsk, Milove and Markivka raions. The maternity hospital in Bilovodsk serves three raions and many women come for delivery from NGCAs of the oblast. The authorities asked to support the hospital with hygiene kits both for women and for newborns. At the national level UN OCHA continues to provide support in the development of the Law on “humanitarian assistance”. It is expected that the draft is finalized by June 30 and then passed for discussion to the Parliament of Ukraine. As of today only 30% of required funding has been funded or pledged as part of Humanitarian Response Plan (HRP). The new Temporary Order on entry/exit to NGCAs has been adopted and came into force. For the moment no commercial cargoes are permitted to NGCAs due to security situation. 2. Update of the current humanitarian situation in Oblast from UN OCHA and LOMCA SES to share the estimated costs of transition center with the humanitarian partners for their participation in The number of officially registered IDPs is growing despite of difficulties in crossing the contact line. -

Annual Progress Report
EU Support to the East of Ukraine – Recovery, Peacebuilding and Governance Annual Progress Report August 2018 – September 2019 EU Support to the East of Ukraine – Recovery, Peacebuilding and Governance Annual Progress Report August 2018 – September 2019 Table of contents List of annexes 5 Abbreviations and acronyms 6 Executive summary 7 Background 12 COMPONENT 1 16 LOCAL GOVERNANCE AND DECENTRALISATION REFORM Result 1.1 Nationwide decentralisation reform is fully implemented in the newly established Amalgamated Territorial Communities (ATCs) in areas of Donetsk and Luhansk oblast under the 18 control of the Government Result 1.2 Access to quality administrative and social services is improved 26 Result 1.3 Government capacity for participatory strategic planning and transparent project 30 implementation is enhanced. COMPONENT 2 36 ECONOMIC RECOVERY AND MSMES DEVELOPMENT REFORM Result 2.1 Network of service providers is established, and market access improved 38 Result 2.2 Access to credit and financing is improved and more flexible in Complement to KFW 43 Result 2.3 Provision of technical and vocational training is of increasing quality.. 46 COMPONENT 3 52 COMMUNITY SECURITY AND SOCIAL COHESION Result 3.1. A network of citizen groups is established to promote social cohesion and sustainable 54 socio-economic development. Result 3.2 Citizen group initiatives are financially supported. 77 COMPONENT 4 79 SECTORAL REFORMS AND STRUCTURAL ADJUSTMENTS (HEALTH) Result 4.1 The regional health care system is effectively functioning at the regional -

Donbas, Ukraine: Organizations and Activities
Geneva Centre for Security Sector Governance Civil Society in Donbas, Ukraine: Organizations and Activities Volodymyr Lukichov Tymofiy Nikitiuk Liudmyla Kravchenko Luhansk oblast DONBAS DONBAS Stanytsia Donetsk Luhanska Zolote oblast Mayorske Luhansk Donetsk Maryinka Novotroitske RUSSIA Hnutove Mariupol Sea of Azov About DCAF DCAF - Geneva Centre for Security Sector Governance is dedicated to improving the se- curity of people and the States they live in within a framework of democratic governance, the rule of law, and respect for human rights. DCAF contributes to making peace and de- velopment more sustainable by assisting partner states and international actors supporting them to improve the governance of their security sector through inclusive and participatory reforms. It creates innovative knowledge products, promotes norms and good practices, provides legal and policy advice and supports capacity building of both state- and non-state security sector stakeholders. Active in over 70 countries, DCAF is internationally recognized as one of the world’s leading centres of excellence for security sector governance (SSG) and security sector reform (SSR). DCAF is guided by the principles of neutrality, impartiality, local ownership, inclusive participation, and gender equality. www.dcaf.ch. Publisher DCAF - Geneva Centre for Security Sector Governance P.O.Box 1360 CH-1211 Geneva 1 Switzerland [email protected] +41 (0) 22 730 9400 Authors: Volodymyr Lukichov, Tymofiy Nikitiuk, Liudmyla Kravchenko Copy-editor: dr Grazvydas Jasutis, Richard Steyne -

1 Introduction
State Service of Geodesy, Cartography and Cadastre State Scientific Production Enterprise “Kartographia” TOPONYMIC GUIDELINES For map and other editors For international use Ukraine Kyiv “Kartographia” 2011 TOPONYMIC GUIDELINES FOR MAP AND OTHER EDITORS, FOR INTERNATIONAL USE UKRAINE State Service of Geodesy, Cartography and Cadastre State Scientific Production Enterprise “Kartographia” ----------------------------------------------------------------------------------- Prepared by Nina Syvak, Valerii Ponomarenko, Olha Khodzinska, Iryna Lakeichuk Scientific Consultant Iryna Rudenko Reviewed by Nataliia Kizilowa Translated by Olha Khodzinska Editor Lesia Veklych ------------------------------------------------------------------------------------ © Kartographia, 2011 ISBN 978-966-475-839-7 TABLE OF CONTENTS 1 Introduction ................................................................ 5 2 The Ukrainian Language............................................ 5 2.1 General Remarks.............................................. 5 2.2 The Ukrainian Alphabet and Romanization of the Ukrainian Alphabet ............................... 6 2.3 Pronunciation of Ukrainian Geographical Names............................................................... 9 2.4 Stress .............................................................. 11 3 Spelling Rules for the Ukrainian Geographical Names....................................................................... 11 4 Spelling of Generic Terms ....................................... 13 5 Place Names in Minority Languages -

I Impact O T of Th Oblasts E Conf S on Th Infr Lict in He
15 September 2014 Kiev IMPACT OF THE CONFLICT IN LUHANSK AND DONETSK OBLASTS ON THE SOCIAL AND ECONOMIC INFRASTRUCTURE SUMMARY This paper presents a summary of the damage assessment in areas affected by the armed conflict of Luhansk and Donets oblasts in the period since the beginning of the conflict until 14 September 2014. As of 14 September 2014, 1,968 facilities (including social infrastructure, residential houses, and enterprises) were reported to receive the damage, amounting to a monetary loss of total UAH 5.958 bn hryvnias, or US$ 440 mln (estimated, without account of unconfirmed damages in the residential sector, disruption of contracts, and lost profits of business enterprises). Among those reported 995 facilities are located in Luhansk oblast (UAH 1.094 million), and 783 facilities are in Donetsk oblast (UAH 3.964 billion). 190 facilities, with an estimated loss of UAH 900 m, belong to railway infrastructure situated in the territory of both oblasts. As can be seen in the consolidated table (page 6 and 7), 1230 housing buildings were damaged (667 in Luhansk and 563 in Donetsk oblasts), and this affected the shelter of 6,618 families (including 1,844 in Luhansk oblast and 4,774 in Donetsk oblast). Due to different limitations in determining the exact number of affected families, the real number of affected families is, most likely, of a greater scale than presented in this report. Indirectly (by worsened access to public services) the conflict in Donbass affected the majority of the 6,6 million population of the Donetsk and Luhansk oblasts. It is worth noting, that the report indicates another 1873 housing buildings damaged during the conflict, however no verification (geographical/address localization) was possible by the team of data collectors, and this number remained outside the main analysis in this paper. -

Protection Cluster Factsheet – March 2021
UKRAINE MARCH 2021 PROTECTION HIGHLIGHTS • Security situation and civilians: The security situation along the contact line continues to be tense. The International NGO Safety Organization reported PROTECTION CLUSTER CONTACTS 533 security incidents, which is at the same level as in February, following the Raquel Trabazo, Protection Cluster escalation of hostilities at the beginning of the year. In March, partners Coordinator, [email protected] recorded 8 civilian casualties (three persons died and five injured), six of Kateryna Martynenko, Child Protection them caused by ERW incidents. The number of damages to civilian housing Sub-Cluster Coordinator further increased with 27 houses damaged as a result of shelling. [email protected] • Freedom of Movement: Two Entry Exit Crossing Points (EECP) are Olena Kochemyrovska, GBV Sub-Cluster Coordinator [email protected] operational on both sides (Stanytsia Luhanska and Novotroitske). On 19 March, free COVID-19 testing became available at the EECP Stanytsia Martin Oubrecht, Mine Action Sub- Cluster Coordinator Luhanska. However, the number of medical staff is not sufficient to cover [email protected] existing needs: every day around 850 persons were crossing the EECP while Akbar Nazriev Age and Disability TWG less than 100 persons could be tested. People have to stay in lines for several Coordinator [email protected] hours to get tested. Protection partners advocate to prioritize vulnerable Volodymyr Khorbaladze, Housing, Land people for free testing. and Property TWG Coordinator Due to the limited operation of the checkpoints, the residents of non- [email protected] government controlled areas (NGCA) are compelled to travel to GCA through the Russian Federation. -

Humanitarian Snapshot 20190410
UKRAINE Humanitarian Snapshot As of 10 April 2019 The latest re-commitment to the ceasefire that came into force on 8 March 2019 brought limited respite from violence. An overall decrease in the number of reported security incidents was observed, with 29 per cent less incidents compared to the previous month. Meanwhile, the number of conflict-related casualties among civilians remained high with 9 injured and 4 killed, as reported by OHCHR. Critical civilian infrastructure frequently came under fire, which caused severe damage and interruption of water and electricity supplies. A number of times the ‘windows of silence’ were agreed to make necessary repairs of the damaged facilities. However, civilian workers came under small-arms fire while conducting emergency repairs of impacted power lines in Marinka (Donetska oblast, GCA) and damaged water pipelines in the area between Berezove (Donetska oblast, GCA) and Olenivka (Donetska oblast, NGCA). While no casualties were reported due to these incidents, the repair works were suspended and further delayed, as the workers were forced to evacuate to safe areas. On 21-22 March, some unexploded ordnances (UXOs) were found in the vicinity of two education facilities in Donetsk (Donetska oblast, NGCA). No casualties were reported as part of these incidents, however, mine contamination in the vicinity of education facilities remains a security threat for students and teachers in eastern Ukraine. CIVILIAN CASUALTIES SECURITY HOTSPOTS 2019 HRP: REQUIREMENTS AND FUNDING** casualties reported Mines and -
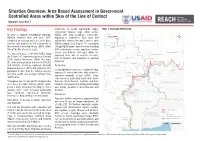
Situation Overview: Area Based Assessment in Government Controlled Areas Within 5Km of the Line of Contact Ukraine, July 2017
Situation Overview: Area Based Assessment in Government Controlled Areas within 5km of the Line of Contact Ukraine, July 2017 Key Findings restrictions on goods significantly reduce Map 1: Assessed Settlements connectivity between large urban centres In order to support humanitarian planning, NGCA and GCA periphery settlements. KHARKIVSKA REACH, between May and June 2017, Adjusting to restrictions, GCA cities and LUHANSKA ² conducted an assessment of access to basic settlements formed new basic service units LUHANSK GCA services and markets in 100 settlements in (BSUs) along the LoC (Map 3). The separation DONETSKA ZAPORIZKA RUSSIAN Government Controlled Areas (GCA) within of large NGCA urban centres from surrounding FEDERATION 5km of the line of contact (LoC). GCA settlements creates significant service EAST LUHANSK The assessed area, a 5km-wide buffer along access and delivery challenges within the assessed area, due to security concerns, SIEVIERODONETSK the 500km LoC, represents an area of nearly SLOVIANSK 2,000 square kilometres. Within the area, lack of transport and departure of qualified POPASNA personnel. KRAMATORSK the estimated population is between 150,000 BAKHMUT 1 STANYTSIA and 200,000 , including registered internally Protection BAKHMUT DONETSK GCA POPASNA LUHANSKA displaced persons (IDPs) and returnees. The Local populations experience regular shelling, LUHANSK population is older than the national average KOSTIANTYNIVKA exposure to mines and other risks related to TORETSK as many youths and younger families have ALCHEVSK explosive remnants of war (ERW). These TORETSK fled the area. concerns were particularly reported in South AVDIIVKA HORLIVKA Throughout the 27 cities and 73 villages in the Donetsk, West Donetsk, Avdiivka and East 2 LUHANSK NGCA area, there is regular military activity , which Luhansk.