Adverse Effects After Medical, Commercial, Or Self-Administered Colon Cleansing Procedures
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Complementary and Alternative Medicine
MEDICAL POLICY Complementary and Alternative Medicine Effective Date: 01/01/2021 Section: MED Policy No: 437 Medical Policy Committee Approved Date: 10/2020 01/1/2021 Medical Officer Date See Policy CPT/HCPCS CODE section below for any prior authorization requirements SCOPE: Providence Health Plan, Providence Health Assurance, Providence Plan Partners, and Ayin Health Solutions as applicable (referred to individually as “Company” and collectively as “Companies”). APPLIES TO: All lines of business BENEFIT APPLICATION Medicaid Members Oregon: Services requested for Oregon Health Plan (OHP) members follow the OHP Prioritized List and Oregon Administrative Rules (OARs) as the primary resource for coverage determinations. Medical policy criteria below may be applied when there are no criteria available in the OARs and the OHP Prioritized List. POLICY CRITERIA Notes: • Member benefits, which address coverage or non-coverage of specific complementary and alternative medicine treatments, may vary. Member benefit contract language takes precedent over medical policy. • Services in this policy may exist in other Medical Policies. See Cross References for guidance. Complementary and alternative medicine treatments are considered investigational and are not covered as a treatment of any condition. Treatments of this nature include but are not limited to the following: A. Autogenous lymphocytic factor B. Colon hydrotherapy, irrigation, cleansing and lavage Page 1 of 13 MED437 MEDICAL POLICY Complementary and Alternative Medicine C. Intravenous infusion including: 1. Hydrogen peroxide 2. Micronutrient (Myers’ cocktail) for indications that are not Lyme disease 3. Vitamin C for indications that are not Lyme disease D. Manual and soft tissue therapies including: 1. Active release techniques® 2. Craniosacral therapy (CST) 3. -

The Ruscombe Mansion Community Health Center
The Ruscoommbbee MMaannssiioonn Community Health Center [email protected] www.Ruscombe.org Vol. 4, Issue 4 4801 Yellowwood Ave., Baltimore, MD 21209 April 10, 2009 in the Coldspring Newtown Editor: Laura Cortner 410-367-7300 Founder and Executive Director: Zohara M. Hieronimus Expand Your Mind, Stretch Your Body Spring Cleaning: Have You Considered Colon Hydrotherapy? To be announced - Mirror, Mirror - Journaling for Body Image with Nancy Evans and Dana Knighten. In an atmos- When scrubbing the surfaces of phere of mutual acceptance, respect, and confidentiality, we your outer world, don’t neglect the will use journaling and artmaking techniques to listen to and cleansing of your inner world, too! deepen our relationship with our authentic selves. Colon hydrotherapy, also known 410.461.7440, [email protected]. as colon irrigation, colon therapy May 29 - 31, 2009 5th Annual Eden Life Journeys Reiki and colon detoxification, can flush and Wellness Retreat organized by Brenda Doetzer- and irrigate your inner world with Pearlstone Conference and Retreat Center in Reisterstown, the infusion of water into the large Presentations by Ruscombe founder Zohara Meyerhoff intestine for colon detoxification. Hieronimus, and herbalist Sara Eisenberg, 410-242-6130, Contact Colon Hydrotherapist Katrina Mahomes to find [email protected] www.EdenLifeJourneys.com out if this treatment is right for you. June 23-24 Level I & June 25-29 Level II -Mining Your Our colon cleansing is done in a very quiet and relaxed Metaphors with Gina Campbell. A systematic process for atmosphere. Privacy is maintained at all times, and because working with your client’s metaphors to promote decision- it is a closed system there is no odor or mess. -

Planning Your Own Detox Diet
GreenGgree Eatz – Healthy Eating for a Green Planet! Planning Your Own Detox Diet A kick-start to a healthier lifestyle Jane Richards 2013 0 All rights reserved.Copyright 2013 by Jane Richards. Contents What is a Natural Detox Diet? ....................................................................................................................................2 Is a Natural Detox right for me? .............................................................................................................................2 What is the best Detox? .........................................................................................................................................3 Best Supplements for a Detox ....................................................................................................................................4 Detox Support for your Liver and Bowel ................................................................................................................4 Flushing out the Toxins ...........................................................................................................................................4 Designing a Detox for You ......................................................................................................................................4 Best and Worst Foods for a Detox Diet ......................................................................................................................6 Worst Foods for a Detox Diet .................................................................................................................................6 -

Colon Cleanse Kit Instructions
1.800.476.0016 GLOBAL HEALING CENTER [email protected] COLON CLEANSE KIT INSTRUCTIONS Eating During the Colon Cleanse There are 2 dietary options for you to choose while performing the colon cleanse. Option 1: Eating fruit only. (For more advanced cleansing) Option 2: Following a healthy food diet. (For the average person) OPTION 1: FRUIT-ONLY DIET • Eat only fruit for 6 days. • Eat whenever you are hungry, every hour if you want. • Eat only one type of fruit per meal. • Eat as much fruit as you like per meal. (Example: Eating 6 bananas for a meal) When performing a colon cleanse, it’s ideal to feed the body The Colon Cleanse Kit Is a 6-Day adequate amounts of fresh organic or locally grown fruit. It is Program best to eat only fruit during the cleanse. Not only does fruit supply the body with the right kind of energy to draw out unwanted substances, it also ensures the small intestine and SUPPLIES CHECKLIST the colon remain well hydrated so it’s an ideal environment to support the cleansing and toxin elimination process. Fresh fruit 4-6 gallons of distilled or purified water supports the elimination process by providing water, oxygen, ----------------------------------------------------------- live fiber, pectin, and many vital nutrients. The following is a list 8 ounces of Apple Cider Vinegar (preferably organic, raw) of great intestinal cleansing fruits: ----------------------------------------------------------- 3 lemons (preferably organic or locally grown) • Apples ----------------------------------------------------------- -

Overcoming Sinus Problems.Pages
Overcoming Sinus Problems ! The ancient cultures knew there was a definite connection between what was happening in the digestive track and colon and what was happening in the respiratory tract. In traditional Chinese Medicine, the large intestine (colon) meridian is paired with the lung !(respiratory) meridian. In other words, what affects one, affects the other. In India, Ayurvedic medicine suggests that lung and respiratory problems are a result of poor digestion. More recently, Dwight Byers, who heads up the International Institute of Reflexology, teaches that if the valve between the small and large intestines is not working properly, material from the large intestine can migrate back to the small intestine, irritating it, which sets up a strong of chemical reactions resulting in the !production of histamines and finally allergy and respiratory problems. If you have only been working from the chest up to the remedy your sinus problems, maybe it’s time to look a little lower and focus on what you can do to help promote good !digestion and health for the small and large intestines. Foods ! What and how we eat can have a profound effect on digestion and colon health. If you have respiratory problems, it’s best to avoid dairy products, especially milk, cheese, and ice cream. Dairy products tend to cause us to produce excess mucous, which can make respiratory problems worse. Also, stay away from sugar as much as possible. Sugar can increase the risk of Crohn’s disease and ulcerative colitis; it can increase the growth of yeast; it can interfere with the absorption of protein, cause food allergies, increase fluid retention, increase the risk of gastric cancer, cause indigestion, feed cancer plus a host of !other things too numerous to mention. -
Diseases of the Digestive System
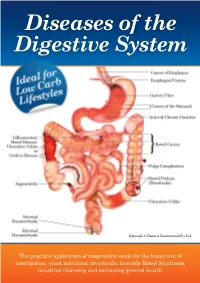
Diseases of the Digestive System Copyright © Denmar International Pty Ltd The practical application of magnesium oxide for the treatment of constipation, yeast infections, diverticula, Irritable Bowel Syndrome, intestinal cleansing and enhancing general health. “Relying on the wisdom and holistic approach of Traditional Chinese Medicine, Western Natural Therapies, and a 6000 year unbroken history of Herbal Medicine, I offer a healing system that focuses on the cause of disease, not merely the suppression of symptoms. My goal is to discover the individuality of your health problem, treat its cause, and stimulate your body to heal itself as soon as possible”. Dennis Vander Kraats B.A., N.D.,Dip.Acup., D.B.M. Is your health care practitioner government registered? Australian Health Practitioner Regulation Agency Government Registration Number: CMR00017122128 Chinese Medicine Practitioner Fellow: Australian Acupuncture & Chinese Medicine Association Ltd (AACMA) Member: Australian Traditional Medicine Society (ATMS) National Herbalist Association Australia (NHAA) Naturopath Personal History Dennis Vander Kraats was born in Toronto, Canada and grew up with a passion for distance running. He represented Canada nationally and internationally on a number of occasions, including the 1979 World Cross Country Championships. His success in athletics earned him a scholarship from the prestigious University of Notre Dame (USA). After arriving in Australia, Dennis and his wife Marion successfully operated a health food store and this stimulated Dennis’s desire to further his knowledge of natural therapies. After eight more years of study, Dennis graduated from the Melbourne College of Naturopathy and Homoeopathy, the Nanjing College of Acupuncture, and the Australian Acupuncture College (Victorian University of Technology) to become a qualified Naturopath and Acupuncturist. -

Colon Hydrotherapy
Colon Hydrotherapy What is colon hydrotherapy? Colon hydrotherapy, also known as colon cleansing or colonic irrigation, is often practised as a form of alternative medicine. The claimed purpose of the procedure is to remove toxin, lose weight, prevent diseases, relieve constipation, promote general health and well-being. Description of the procedure It is known that such procedure commonly involved the use of “Colonic Irrigation Systems” which are medical devices originally intended for bowel preparation before radiological or endoscopic procedures. The client generally lies down and water is pumped through the rectum via a tube. Fluids and waste are expelled through another tube. A large volume of fluid, up to 60 litres would be introduced into the colon via the rectum. The procedure may be repeated several times. Purported mechanism of action It is claimed that with the introduction of filtered and temperature regulated water into the colon through the anus, the waste could be softened and loosened, resulting in evacuation through natural bowel movement. The purported health benefit is claimed to be achieved by removing waste and toxins from the body. However, there is a lack of evidence from the medical literature that colon cleansing can produce these effects. Potential risks and complications • Complications associated with the procedure may include abdominal pain, nausea and vomiting, diarrhoea and dehydration. It may also result in electrolyte disturbances causing symptoms like nausea, fatigue, etc. Severe complications include bowel perforation, renal failure, pelvic abscess and air embolism. • The use of improperly sterilised equipment may lead to transmission of infection. Outbreak of amoebiasis with fatalities associated with colon hydrotherapy has been reported. -

FDA Philippines - Prohibited Items
FDA Philippines - Prohibited Items A & J Baguio Products Pure Honey Bee A & W Change Lip Gloss Professional A & W Waterproof Mascara Long Lash-Run Resistant A Bonne’ Milk Power Lightening Lotion + Collagen Double Moisturizing & Lightening A&W Smooth Natural Powder (1) A. Girl® Matte Flat Velvet Lipstick A.C Caitlyn Jenner Powder Plus Foundation Studio Mc08 Aaliyah'S Choco-Yema Spread Aaliyah'S Roasted Peanut Butter, Smooth Original Aaliyah'S Rocky Roasted Peanut Butter Spread, Rocky Nuts Aamarah’S Beauty Products Choco Berry Milk Super Keratin Conditioner With Aloe Vera Extract Ab Delicacies Breadsticks Ab Delicacies Fish Cracker Ab Delicacies Peanut Ab Delicacies Pork Chicharon Abby’S Delicious Yema Abc Crispy Peanut And Cashew Abrigana Fish Crackers Snack Attack Absolute Nine Slim Ac Makeup Tokyo Oval Eyebrow Pencil N Ac Makeup Tokyo Eyebrow Pencil Dark Brown Acd Marshmallows Acd Spices Flavorings,Cheese Powder Ace Edible Oil Ace Food Products Serapina Aceite De Alcanfor 25Ml Achuete Powder Acne Cure Clarifying Cleanser With Tea Tree Oil Acnecure Pimple Soap Active White Underarm Whitening Soap Ad Lif Herbal Juice, Graviola Barley,Moringa Oleifera Fruits And Vegetables Ade Food Products Korean Kimchi Chinese Cabbage Ade’S Native Products Buko Pie Adelgazin Plus Adorable Cream Bar Chocolate Flavor Ads Fashion Blusher (A8408) (3) Advanced Formula L-Glutathione White Charm Food Supplement Capsule Advanced Joint Support Instaflex Advanced Featuring Uc-Ii® Collagen Dietary Supplement Aekyung 2080 Kids Toothpaste Strawberry African Slim African Mango Extract African Viagra 4500Mg Ageless Bounty Resveratrol 1000Mg Advance Agriko 5 In 1 Tea Juice Extract Agriko 5 In 1 Turmeric Tea Powder With Brown Sugar Agriko 5 In 1 Turmeric Tea Powder With Brown Sugar Agua (Cleansing Solution) 60Ml Agua Boo Purified Drinking Water Agua Oxigenada F.E.U. -

Complaint Exhibits
Case 3:11-cv-01715-VLB Document 1-1 Filed 11/07/11 Page 1 of 6 EXHIBIT A Case 3:11-cv-01715-VLB Document 1-1 Filed 11/07/11 Page 2 of 6 Channel 8 Health News - Diet Trends: A look at America's Top Diets Advertorial Thursday, September 30, 2010 Acai Berry Diet Exposed: Miracle Diet or Scam? Thursday, September 30, 2010 As part of a new series: "Diet Trends: A look at America's Top Diets" we examine consumer tips for dieting during a recession » RELATED VIDEOS Acai Berry: Fox35 Special Report ( Chicago ) - Acai berries are the latest weight loss fad. These so called Super Foods that you take as a supplement to lose weight have been getting a lot of international attention. And like you have probably already seen; they are all Acai Health Benefits. America's #1 Superfood. Look younger and over the internet in blogs and success stories of Live Longer and Healthier. people who have apparently used the pills and lost a ton of weight. The Real Dangers of having a Toxic Colon But we here at Channel 8 are a little skeptical and aren‘t sure that we‘ve seen any real proof Julie investigates the that these pills work for weight loss. So we Acai Berry diet to find out decided to put these products to the test. What for herself if this super better way to find out the truth than to conduct diet works. our own study? Julie Ayers, our Health and Diet columnist, recently put the Acai Diet to the test. -

The Amazing Liver Cleanse
THE AMAZING LLLIIIVVVEEERRR CCCLLLEEEAAANNNSSSEEE A Powerful Approach To Improve Your Health And Vitality AAAnnndddrrreeeaaasss MMMooorrriiitttzzz © 2002 by Andreas Moritz. All rights reserved. No part of this book may be reproduced, stored in a retrieval system, or transmitted by any means, electronic, mechanical, photocopying, recording, or otherwise, without written permission from the author. ISBN: 1-4033-2996-6 (e-book) ISBN: 1-4033-2997-4 (Paperback) This book is printed on acid free paper. 1stBooks - rev. 08/15/02 Cover Design and Artwork by Andreas Moritz [The picture on the cover is part of Ener-Chi Art (see http://www.ener-chi.com), designed to restore balanced Chi flow in all organs and systems of the body. This particular picture is for improving liver function.] First edition 1998 Second edition (revised) 1999 Third edition (extended and revised) 2002 iii iv Also by Andreas Moritz … The Key To Health and Rejuvenation Freedom From Judgment It’s Time to Wake Up Ener-Chi Art v vi Andreas Moritz 1stBooks vii viii The Amazing Liver Cleanse A Powerful Approach To Improve Your Health And Vitality ix x For Reasons of Legality The author of this book does not advocate the use of any particular form of health care but believes that the facts, figures, and knowledge presented herein should be available to every person concerned with improving his or her state of health. Although the author has attempted to give a profound understanding of the topics discussed and to ensure accuracy and completeness of any information that originates from any other source than his own, he and the publisher assume no responsibility for errors, inaccuracies, omissions, or any inconsistency herein. -

Colon Hydrotherapy an Update
COLON HYDROTHERAPY AN UPDATE HEALTH TECHNOLOGY ASSESSMENT SECTION MEDICAL DEVELOPMENT DIVISION MINISTRY OF HEALTH MALAYSIA 012/2009 i DISCLAIMER Technology review is a brief report, prepared on an urgent basis, which draws on restricted reviews from analysis of pertinent literature, on expert opinion and / or regulatory status where appropriate. It is subjected to an external review process. While effort has been made to do so, this document may not fully reflect all scientific research available. Additionally, other relevant scientific findings may have been reported since completion of this review. Please contact: [email protected], if you would like further information. Health Technology Assessment Section (MaHTAS), Medical Development Division Ministry of Health Malaysia Level 4, Block E1, Precinct 1 Government Office Complex 62590 Putrajaya Tel: 603 88831246 Fax: 603 8883 1230 Available at the following website: http://www.moh.gov.my ii Prepared by: Dr Junainah Sabirin Principal Assistant Director Health Technology Assessment Section (MaHTAS) Ministry of Health Malaysia En Sahaludin Sharif Assistant Medical Officer Health Technology Assessment Section (MaHTAS) Ministry of Health Reviewed by: Datin Dr Rugayah Bakri Deputy Director Health Technology Assessment Section (MaHTAS) Ministry of Health Malaysia External reviewer: Dr Wan Khamizar Wan Khazim Consultant Colorectal Surgeon Hospital Sultanah Bahiyah Alor Setar, Kedah DISCLOSURE The authors of this report have no competing interest in this subject and the preparation of this report is totally funded by the Ministry of Health, Malaysia iii EXECUTIVE SUMMARY Introduction Colon cleansing (colon therapy) encompasses a number of alternative medical therapies intended to remove faecal waste and unidentified toxins from the colon and the intestinal tract. -

There Are Risks Inherent in Most, If Not All, Medical Treatments, Whether Given by an Allopathic Doctor Or an Alternative
“Ideal” practice helps this FP thrive ample, the first case study involved a 31-year- As a young solo doctor who often feels like old with Crohn’s disease—a specific contra- a black sheep in the larger family physician indication for colon therapy. Therapists certi- community, I very much appreciated Dr. fied by the Global Professional Association for Susman’s editorial, “The rebirth of the solo Colon Therapy (http://GPACT.org) are taught family doc” (J Fam Pract. 2011;60:510). Were to give extensive health background ques- it not for the support of the Ideal Medical tionnaires before administering colon hydro- Practice (IMP) community, I do not think I therapy, so it is difficult to determine whether would be in clinical medicine at all, as I know the therapist or the patient was at fault for fail- I could not be happy on the hamster wheel of ure to disclose her health status. Other case traditional high-volume primary care prac- reports the authors cited described isolated tice. IMP has provided the guidance and events that either involved people who already support that enabled me to open a solo full- had severe health problems or could not be at- spectrum integrative family medicine prac- tributed to colon hydrotherapy with certainty. tice in Rochester, NY, right out of residency. While there is no denying the paucity of Because of the skills and knowledge I studies on the potential benefits of colonic have developed through such resources as irrigation, it is unfortunate that the authors monthly conference calls, e-mail listservs, chose to omit the few studies that have been Web forums, and a national conference, my conducted.