Strengthening Primary Healthcare System in Iraq (D2-03) Phase-1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Housing Land & Property Issues
HOUSING LAND & PROPERTY ISSUES AMONG IDPs SETTLED IN BASRA, DOHUK, ERBIL & BAGHDAD QUICK ASSESSMENT REPORT – DRAFT 13 November 2014 The purpose of the rapid Housing, Land and Property (HLP) survey, initiated by UN-Habitat among internally displaced people (IDPs) currently living in five key Iraqi cities, is to collect indicative data on land tenure status of the displaced and improving our understanding of issues related to the possible return of IDPs to their former properties. The data collection was undertaken between September and November 2014 by UN-Habitat staff in collaboration with local partners and community representatives, on the basis of a purposely-developed questionnaire. The present report focuses on information captured from 774 IDPs households currently living in Basra, Dohuk, Erbil, Baghdad, respectively the capitals of the Basra, Dohuk, Erbil and Baghdad governorates.1 The surveys were conducted in IDPs camp, planned and unplanned urban areas, hotels and churches. These locations were selected for the presence of large numbers of displaced, accessibility by local partners and took into consideration the geographic and ethnical diversity of respondents. KEY SURVEY FINDINGS Provenance of IDPs : The large majority of the IDPs interviewed for this survey has abandoned properties in the northern Governorate of Ninawa, namely the towns of Al-Hamdaniya, Mosul and Tilkef; followed by the Governorates of Anbar, Diyala, Salah El-den, Kirkuk, Baghdad and Al-Hilla. Figure 1 below provides a breakdown by Governorate. It should be noted that many of those that fled the sectarian clashes affecting the Governorate of Ninawa are Christian minorities, some of which had sought refuge in the Nineveh plains 2 and for whom the present location is therefore not their first displacement. -

The Evolution of Modern Healthcare and Health Education in Iraq Majeed Hamad Ameen 1 Aamir Jalal Al Mosawi 2 Adnan Anoze 3
Review Article The Evolution of Modern Healthcare and Health Education In Iraq Majeed Hamad Ameen 1 Aamir Jalal Al Mosawi 2 Adnan Anoze 3 The N Iraqi J Med, April 2011; 7(1):72-80 he1 aim of this paper is to provide a mandate under British control with the name description of the evolution of modern "State of Iraq". Emir (Prince) Faisal, leader of Thealth care and medical and health the Arab revolt against the Ottoman sultan education in Iraq based largely on official during the Great War, and member of the governmental papers and documents. Hashemite family from Mecca, became the first king of the new state. He obtained the throne The healthcare and health services were partly by the influence of T. E. Lawrence. seriously bad during the Ottoman reign. The Although the monarch was legitimized and few hospitals established didn t meet the public proclaimed King by a plebiscite in 1921, nominal demands. After the World War I, Iraq passed independence was only achieved in 1932, when from the failing Ottoman Empire to the British the British Mandate officially ended.(1-3) control Many of these hospitals were damaged during the First World War. During the British occupation the British army directorate of The formation of National governance in health affairs provided health service to people Iraq with establishment of the Hashemite in Basra most probably in attempt to reduce the Kingdom in the 23rd of August 1921 was exposure of the British army to the diseases in associated with beginning of the evolution of the region. -

Wash Needs in Schools Iraq
COMPARATIVE OVERVIEW WASH NEEDS IN SCHOOLS OF KEY INDICATORS Note: Findings derived from WFP data are December 2019 IRAQ presented in turquoise boxes. Methodology Water Hygiene Sanitation 1 3 2 REACH Number of HH surveys conducted by Number of schools assessed by WFP Drinking water from a water source is available Drinking water from a water source is available Drinking water comes from an improved water source The water quality is perceived to be acceptable The main water source is at the school's premises Has access to handwashing facilities Has access to handwashing facilities of which is having water and soap available of which is functional of which is having soap Has access to improved sanitation facilities number of Average functional student toilets per school building number of toilets Average for students number of Average students per toilet Has access to student toilets separated by gender Has access to student toilets separated by gender Has unusable toilets Is having a good structural condition of student toilets Is having a good hygienic condition of student toilets Al-Falluja 115 88% 100% 78% 93% 100% 97% 100% 9,1 82% 0% Al-Ramadi 80 83% 98% 81% 98% 100% 100% 100% 8,6 93% 0% Al-Anbar Ana 74 31 44% 65% 87% 49% 72% 94% 94% 64% 66% 62% 94% 5,8 5,4 36 90% 90% 23% 100% 71% Heet 87 72% 100% 60% 100% 93% 97% 100% 9,0 88% 0% Shat Al-Arab 98 12% 92% 83% 11% 7,2 91 77% 56% 46% Al-Basrah Al-Khidhir 70 50% 66% 76% 11% 5,8 69 79% 74% 32% Al-Muthanna Al-Kufa 120 21% 46% 71% 99% 100% 23% 99% 6.5 71% 27% Al-Najaf Al-Najaf 94 2% 95% 98% -

Erbil Governorate Profile Overview2 May 2015
ERBIL GOVERNORATE PROFILE OVERVIEW2 MAY 2015 41,313 IDP FAMILIES 2,592 IDP families 6% IDP camps 1 total population: 6,598 individuals 247,878 IDP INDIVIDUALS planned: 13,732 individuals Syrian refugee camps 110, 378 SYRIAN REFUGEE 8,756 IDP families DISPLACEMENT OVER TIME INDIVIDUALS 21% 41,313 Darashakran 45,000 SUM OF IDPFAMILIES 38% OF ALL IDPS ARE UNDER 14 35,758 Basirma 40,000 Kawergosk 32,324 33,181 26,681 IDP families 32,604 65% 35,000 31,324 1,575 IDP families 28,424 26,087 GOVERNORATE OF ORIGIN Baharka 4% 30,000 Ankawa 2 26,014 Harsham 1,709 IDP families 25,000 19,734 4% 20,000 IDPs in I 23% 27% all ra f q Qushtapa 15,000 o % 10,000 3,328 9 Debaga 3,643 3,245 5,000 - 17% 33% 99% MOST COMMON SHELTER TYPE INTENTIONS Anbar Diyala Erbil Ninewa Salah al Din Soran 100% WAVES OF DISPLACEMENT Shaqlawa 94% 2% Makhmur 47% 53% 17% 9%14% Koisnjaq 57% 43% Rented Host Families Informal settle- Erbil 90% 10% housing 70% 8,5% ments 7% Gov Total 88% 11% Iraq 89% 8% TOP PRIORITY NEEDS 0% 20% 40% 60% 80% 100% 29% 40% 1 1 2 3 4 Return to Area of Past Displacement Return4 to place of origin 90% Waiting on one or several factors Locally integrate in current location Access Food Water Health Shelter Moving and integrating in a different location outside of Iraq Pre June 14 June July 14 to income Resettle in a third location 14-Aug Post September14 1. -

Iraq: Medical and Healthcare Provision
Country Policy and Information Note Iraq: Medical and healthcare provision Version 2.0 January 2021 Preface Purpose This note provides country of origin information (COI) and analysis of COI for use by Home Office decision makers handling particular types of protection and human rights claims (as set out in the Introduction section). It is not intended to be an exhaustive survey of a particular subject or theme. It is split into two main sections: (1) analysis and assessment of COI and other evidence; and (2) COI. These are explained in more detail below. Country of origin information The country information in this note has been carefully selected in accordance with the general principles of COI research as set out in the Common EU [European Union] Guidelines for Processing Country of Origin Information (COI), dated April 2008, and the Austrian Centre for Country of Origin and Asylum Research and Documentation’s (ACCORD), Researching Country Origin Information – Training Manual, 2013. Namely, taking into account the COI’s relevance, reliability, accuracy, balance, currency, transparency and traceability. The structure and content of the country information section follows a terms of reference which sets out the general and specific topics relevant to this note. All information included in the note was published or made publicly available on or before the ‘cut-off’ date(s) in the country information section. Any event taking place or report/article published after these date(s) is not included. All information is publicly accessible or can be made publicly available, and is from generally reliable sources. Sources and the information they provide are carefully considered before inclusion. -
20141214 04 IOM DTM Repor
TURKEY Zakho Amedi Total Families: 27,209 TURKEY Zakho Amedi TURKEY Total Families: 113,999 DAHUK Mergasur DAHUK Mergasur Dahuk Sumel 1 Sumel Dahuk 1 Soran Individual : 163,254 Soran Individuals : 683,994 DTM Al-Shikhan Akre Al-Shikhan Akre Tel afar Choman Telafar Choman Tilkaif Tilkaif Shaqlawa Shaqlawa Al-Hamdaniya Rania Al-Hamdaniya Rania Sinjar Pshdar Sinjar Pshdar ERBIL ERBIL DASHBOARD Erbil Erbil Mosul Koisnjaq Mosul Koisnjaq NINEWA Dokan NINEWA Dokan Makhmur Sharbazher Penjwin Makhmur Sharbazher Penjwin Dabes Dabes IRAQ IDP CRISIS Al-Ba'aj SULAYMANIYAH Al-Ba'aj SULAYMANIYAH Hatra Al-Shirqat Kirkuk Hatra Al-Shirqat Kirkuk Sulaymaniya Sulaymaniya KIRKUK KIRKUK Al-Hawiga Chamchamal Al-Hawiga Chamchamal DarbandihkanHalabja SYRIA Darbandihkan SYRIA Daquq Daquq Halabja SHELTER GROUP Kalar Kalar Baiji Baiji Tooz Tooz BY DISPLACEMENT FLOW Ra'ua Tikrit SYRIA Ra'ua Tikrit Kifri Kifri January to December 9, 2014 SALAH AL-DIN Haditha Haditha SALAH AL-DIN Samarra Al-Daur Khanaqin Samarra Al-Daur Khanaqin Al-Ka'im Al-Ka'im Al-Thethar Al-Khalis Al-Thethar Al-Khalis % OF FAMILIES BY SHELTER TYPE AS OF: DIYALA DIYALA Ana Balad Ana Balad IRAN Al-Muqdadiya IRAN Al-Muqdadiya IRAN Heet Al-Fares Heet Al-Fares Tar m ia Tarm ia Ba'quba Ba'quba Adhamia Baladrooz Adhamia Baladrooz Kadhimia Kadhimia JANUARY TO MAY CRISIS KarkhAl Resafa Ramadi Ramadi KarkhAl Resafa 1 Abu Ghraib Abu Ghraib BAGHDADMada'in BAGHDADMada'in ANBAR Falluja ANBAR Falluja Mahmoudiya Mahmoudiya Badra Badra 2% 1% Al-Azezia Al-Azezia Al-Suwaira Al-Suwaira Al-Musayab Al-Musayab 21% Al-Mahawil -

Mosul Response Dashboard 20 Aug 2017
UNHCR Mosul Emergency Response Since October 2016 23 August 2017 UNHCR Co-coordinated Clusters: 1,089,564 displaced since 17 October 2016 Camp/Site Plots Tents Complete + of whom 838,608 are NFI Kits WƌŽƚĞĐƟŽŶ ƐƟůůĐƵƌƌĞŶƚůLJĚŝƐƉůĂĐĞĚ & ;ŽͲĐŽŽƌĚŝŶĂƚĞĚďLJhE,ZΘZͿ Targets:44,000 60,000 87,500 ƐƐŝƐƚĞĚďLJhE,Z KĐĐƵƉŝĞĚ DistribƵted 8,931 10,586 SŚĞůƚĞƌΘE&/ 8,931 3,360 (Co-coordinated ďLJhE,ZΘEZͿ 454,098 144,703 20,576 16,849 ( 17,294 16,398 ŝŶĚŝǀŝĚƵĂůƐ ŝŶĚŝǀŝĚƵĂůƐ Developed Plots Available assisted assisted Camp ŽŽƌĚŝŶĂƟŽŶΘ 34,671 73,554 ĂŵƉDĂŶĂŐĞŵĞŶƚ in camps ŽƵƚŽĨĐĂŵƉƐ 6,187 34,220 /ŶĐůƵĚĞƐĐŽŶŇŝĐƚͲĂīĞĐƚĞĚ EĞǁƌĞƋƵŝƌĞŵĞŶƚƐ EĞǁƌĞƋƵŝƌĞŵĞŶƚƐ ! ;ŽͲĐŽŽƌĚŝŶĂƚĞĚďLJhE,ZΘ/KDͿ ƉŽƉƵůĂƟŽŶǁŚŽǁĞƌĞ ŶĞǀĞƌĚŝƐƉůĂĐĞĚ in 2017 in 2017 Derkar dhZ<z Batifa 20km UNHCR Protection Monitoring for Mosul Response Zakho Amadiya Amedi Soran Mergasur Dahuk Ü 47,478 HHs Assessed Sumel Dahuk ^zZ/EZ 212,978 IndividƵals ZWh>/ DAHUK Akre Choman Mosul Dam Lake Shikhan Soran Choman Amalla ISLADIC Mosul Dam Nargizlia 1 B Nargizlia 2 ZEPUBLIC Tilkaif B Telafar Zelikan (n(new) OF IZAN QaymawaQ (Zelikan) B Shaqlawa 58,954 60,881 48,170 44,973 NINEWA HamdaniyaHdHamdaddaa iyaiyyay Al Hol HasanshamHaasasanshams U2 campp MosulMosuMosMooosssuulul HasanshamHasansham U3 Rania BartellaBartelllalaB B Pshdar Mosul BBBHhM2Hasanshamaanshnnssh M2 KhazerKhazehaha M1 Plots in UNHCR Constructed Camps Sinjar BChamakorChamakor As Salamiyah S y Erbil Hammamammama Al-AlilAlil 2 Al Salamiyah 2 DUKAN Occupied Plots Developed Plots Undeveloped Plots BB B RESERVOIR HammamHammH AAlAl-Alil Alil Erbil B Al ^alamiyaŚ -

Poverty Rates
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Mapping Poverty inIraq Mapping Poverty Where are Iraq’s Poor: Poor: Iraq’s are Where Acknowledgements This work was led by Tara Vishwanath (Lead Economist, GPVDR) with a core team comprising Dhiraj Sharma (ETC, GPVDR), Nandini Krishnan (Senior Economist, GPVDR), and Brian Blankespoor (Environment Specialist, DECCT). We are grateful to Dr. Mehdi Al-Alak (Chair of the Poverty Reduction Strategy High Committee and Deputy Minister of Planning), Ms. Najla Ali Murad (Executive General Manager of the Poverty Reduction Strategy), Mr. Serwan Mohamed (Director, KRSO), and Mr. Qusay Raoof Abdulfatah (Liv- ing Conditions Statistics Director, CSO) for their commitment and dedication to the project. We also acknowledge the contribution on the draft report of the members of Poverty Technical High Committee of the Government of Iraq, representatives from academic institutions, the Ministry of Planning, Education and Social Affairs, and colleagues from the Central Statistics Office and the Kurdistan Region Statistics during the Beirut workshop in October 2014. We are thankful to our peer reviewers - Kenneth Simler (Senior Economist, GPVDR) and Nobuo Yoshida (Senior Economist, GPVDR) – for their valuable comments. Finally, we acknowledge the support of TACBF Trust Fund for financing a significant part of the work and the support and encouragement of Ferid Belhaj (Country Director, MNC02), Robert Bou Jaoude (Country Manager, MNCIQ), and Pilar -

Iraq's Displacement Crisis
CEASEFIRE centre for civilian rights Lahib Higel Iraq’s Displacement Crisis: Security and protection © Ceasefire Centre for Civilian Rights and Minority Rights Group International March 2016 Cover photo: This report has been produced as part of the Ceasefire project, a multi-year pro- gramme supported by the European Union to implement a system of civilian-led An Iraqi boy watches as internally- displaced Iraq families return to their monitoring of human rights abuses in Iraq, focusing in particular on the rights of homes in the western Melhaniyeh vulnerable civilians including vulnerable women, internally-displaced persons (IDPs), neighbourhood of Baghdad in stateless persons, and ethnic or religious minorities, and to assess the feasibility of September 2008. Some 150 Shi’a and Sunni families returned after an extending civilian-led monitoring to other country situations. earlier wave of displacement some two years before when sectarian This report has been produced with the financial assistance of the European Union violence escalated and families fled and the Department of Foreign Affairs, Trade and Development Canada. The con- to neighbourhoods where their sect was in the majority. tents of this report are the sole responsibility of the publishers and can under no circumstances be regarded as reflecting the position of the European Union. © Ahmad Al-Rubaye /AFP / Getty Ceasefire Centre for Civilian Rights The Ceasefire Centre for Civilian Rights is a new initiative to develop ‘civilian-led monitoring’ of violations of international humanitarian law or human rights, to pursue legal and political accountability for those responsible for such violations, and to develop the practice of civilian rights. -
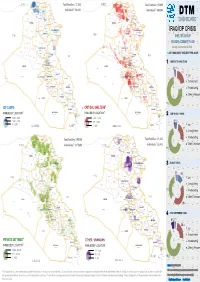
Protracted Displacement in Iraq: District of Origin Profiles
PROTRACTED DISPLACEMENT IN IRAQ: DISTRICT OF ORIGIN PROFILES AUGUST 2021 IOM IRAQ The opinions expressed in the report are those of the authors and do not necessarily reflect the views of the International Organization for Migration (IOM). The designations employed and the presentation of material throughout the report do not imply the expression of any opinion whatsoever on the part of IOM concerning the legal status of any country, territory, city or area, or of its authorities, or concerning its frontiers or boundaries. IOM is committed to the principle that humane and orderly migration benefits migrants and society. As an intergovernmental organization, IOM acts with its partners in the international community to: assist in meeting the operational challenges of migration; advance understanding of migration issues; encourage social and economic development through migration; and uphold the human dignity and well-being of migrants. The information contained in this report is for general information purposes only. Names and boundaries on DTM information products do not imply official endorsement or acceptance by IOM. The information in the DTM portal and in this report is the result of data collected by IOM field teams and complements information provided and generated by governmental and other entities in Iraq. IOM Iraq endeavors to keep this information as up to date and accurate as possible, but makes no claim —expressed or implied— on the completeness, accuracy and suitability of the information provided through this report. Challenges that should be taken into account when using DTM data in Iraq include the fluidity of the displaced population movements along with repeated emergencies and limited or no access to parts of the country. -

Medical and Healthcare Provision
Country Policy and Information Note Iraq: Medical and healthcare provision Version 2.0 January 2021 Preface Purpose This note provides country of origin information (COI) and analysis of COI for use by Home Office decision makers handling particular types of protection and human rights claims (as set out in the Introduction section). It is not intended to be an exhaustive survey of a particular subject or theme. It is split into two main sections: (1) analysis and assessment of COI and other evidence; and (2) COI. These are explained in more detail below. Country of origin information The country information in this note has been carefully selected in accordance with the general principles of COI research as set out in the Common EU [European Union] Guidelines for Processing Country of Origin Information (COI), dated April 2008, and the Austrian Centre for Country of Origin and Asylum Research and Documentation’s (ACCORD), Researching Country Origin Information – Training Manual, 2013. Namely, taking into account the COI’s relevance, reliability, accuracy, balance, currency, transparency and traceability. The structure and content of the country information section follows a terms of reference which sets out the general and specific topics relevant to this note. All information included in the note was published or made publicly available on or before the ‘cut-off’ date(s) in the country information section. Any event taking place or report/article published after these date(s) is not included. All information is publicly accessible or can be made publicly available, and is from generally reliable sources. Sources and the information they provide are carefully considered before inclusion. -

Iraq Healthcare and Humanitarian Reports
Iraq Healthcare and Humanitarian Reports: Compiled by Ben Meyer, June 2007 IRIN: Iraq: Educational standards plummet (16 May 2007) http://www.reliefweb.int/rw/RWB.NSF/db900SID/EVOD- 739HE6?OpenDocument&rc=3&emid=ACOS-635P5D An IRIN report on the educational situation in Iraq. It quotes a staff member at Baghdad University who states, "Violence and lack of resources have undermined the education sector in Iraq. No student will graduate this year with sufficient competence to perform his or her job, and pupils will end the year with less than 60 percent of the knowledge that was supposed to have been imparted to them." Additionally, he states, "Medics, pharmacists, biologists and dentists are desperately seeking training in hospitals because what they have learnt so far does not give them enough confidence to treat patients.” IRIN: Iraq: Child mortality soars because of violence, poor health care (15 May 2007) http://www.reliefweb.int/rw/RWB.NSF/db900SID/TBRL- 738KPC?OpenDocument&rc=3&emid=ACOS-635P5D An IRIN report summarizing the findings of Save the Children report on the humanitarian situation in Iraq. The report states that, “50 Iraqi children died per 1,000 live births in 1990. Today, the rate is 125 per 1,000 births, more than double.” Additionally, “122,000 Iraqi children died in 2005 before reaching their fifth birthday. More than half of these deaths were among newborn babies in the first month of life.” The report states also that 30% of child deaths are caused by pneumonia and diarrhea, making them among the top killers of children in Iraq.