Frail Or Hale: Skeletal Frailty Indices in Medieval London Skeletons
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Upper Mitcham Heritage
had actually started in the 14thC) but increased on an an on increased but 14thC) the in started actually had (which herbs aromatic and medicinal of cultivation the for 18thC the in known best became Mitcham Georgian period Medieval/Tudor villages. surrounding networks(tracks)leadingto centraltoroad then were whicheven (CricketGreen) andLowerGreen Green) (Fair –UpperGreen greens onthecurrent centred Settlements inthelateSaxonandearlyNormanperiods sea-bornefrom raiders. tothecityofLondon theapproaches toprotect area inhabitants mayhavebeenencouragedtosettleinthe the siteofathrivingSaxonsettlement.Itisthought Roman occupationofBritain,andbythe7thC,was the Mitcham wasidentifiedasasettlementlongbefore Roman/Saxon period for horses. coaching parties,withmanyinns stabling facilities fortravellersand Mitcham wasabusythoroughfare and systemhadbeenimproved Londoners. Theroad by Epsom hadbecomeaSpamuchfavoured commons andwatermeadows.Bythemid17thC village withopenfieldsinstripcultivation,extensive agricultural By the17thCMitchamwasaprosperous five separateoccasions. but importantenoughforQueenElizabethItovisiton estates orlandinMitcham–toomanytomentionhere, By theendof16thCmanynotablepeoplehad London. inTudor water–bothscarce airandpure fresh for to LondonandRoyalPalaces,itsreputation Alsoinitsfavourwascloseness good company. forits the 16thCMitchamwasbecomingrenowned attaining thehigherstatusoflandowners.Thusby seekingestatesinMitcham,as ameansof were theCityofLondon andbankersfrom merchants isevidencethatwealthy themid14thCthere From in theConquest. -
Alaris Capture Pro Software
THE ROYAL BURIALS OF THE HOUSE OF YORKAT WINDSOR. II. Princess Mary,May 1482, and Queen Elizabeth Woodville,June 1492.- ANNE F. SUTTON AND LIVIA VISSER—FUCHS Princess Mary, May 1482. Mary, the second daughter of Edward IV and Elizabeth Woodville, born August 1467, ' was not fifteen when she died at Greenwich' 1n May 1482, in the week before Whit Sunday. Little is known of be; life. The joint households of the infant Princesses Elizabeth and Mary had cost £400 a year when they were very young, and this amount was allowed to the queen by the king} As the second daughter she had been the subject of two marriage negotiations: she had been scheduled to succeed her-elder sister, Elizabeth, as the betrothed of Charles, the Dauphin of France, if Elizabeth died, and in 1481, shortly before her death, she was proposed as a bride for Frederick, King of Denmark. In his will of 1475 Edward IV had left her a portion of 10,000 marks provided she was ruled by her mother the queen in all matters.1 In 1478 she and her sister, Elizabeth, had attended the reburial of their grandfather, Richard, Duke of York,“ but in 1480 she apparently did not attend the Garter ceremonies of that year with her mother and sisters, Elizabeth and Cecily.’ There is confusion about the date of Mary’s death. Both the'Monday“ (20 May) and the Thursday’ (23 May) ‘before Whit Sunday’ are given by the surviving copies of the narrative of her burial,“ though they agree on the dates of her burial: 446 the Monday and Tuesday in Whitsun Week, 27-28 May.9 Edward IV was at Canterbury on 17 May, and back in London on 23 May, and may have seen his dying daughter between those dates. -

Merton Priory Team Ministry Parish Profile
PARISH PROFILE TEAM RECTOR www.christchurchsw19.org.uk www.holytrinity-southwimbledon.org.uk www.stjohnsw19.org.uk MERTON PRIORY TEAM MINISTRY Contents MERTON PRIORY TEAM MINISTRY OUR NEW TEAM RECTOR WHAT WE CAN OFFER CHURCH PROFILES: HOLY TRINITY AND ST PETER, SOUTH WIMBLEDON CHRIST CHURCH, COLLIERS WOOD ST JOHN THE DIVINE, MERTON CHURCH SCHOOLS: HOLY TRINITY C of E PRIMARY SCHOOL THE PRIORY C of E PRIMARY SCHOOL DEANERY NEXT STEPS PARISH MAP FINANCIAL INFORMATION 2 MERTON PRIORY TEAM MINISTRY MERTON PRIORY TEAM MINISTRY Merton Priory Team Ministry came into existence in 2009 through the amalgamation of the parishes of Holy Trinity and St Peter South Wimbledon, St John the Divine Merton, and Christ Church Colliers Wood into a single parish. The churches have been inspired by a common vision to work together and encourage each other to offer a more effective service to the neighbourhood. The parish covers a varied area of residential housing in the centre of the London Borough of Merton. The parish has a total population of 33,000. There is a wide diversity of social and ethnic groups and a spread of ages. In recent years the proportion of families with school age children has grown, as reflected in recent primary school expansions. Housing is a mix of private owner-occupied, private rented and social housing. There are three high streets in the parish, numerous small businesses, retail outlets, restaurants, three residents’ associations, five parks and six primary schools. The area has great transport links: stations on the Northern Line and District Line of the underground are in the parish, as well as two mainline stations, Wimbledon and Haydons Road and the Wimbledon terminus of Croydon Tramlink. -
365 March/April 2003 a NEOLITHIC FLAKED FLINT AXE from WALLINGTON Jonathan Cotton the Axe figured Here Was Passed to the Writer for Recording in May 2002
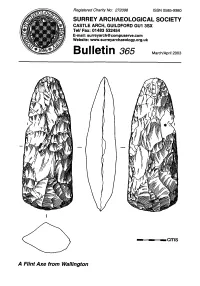
Registered Charity No: 272098 ISSN 0585-9980 SURREY ARCHAEOLOGICAL SOCIETY CASTLE ARCH, GUILDFORD GUI 3SX Tel/ Fax: 01483 532454 E-mail: [email protected] / Website: www.surreyarchaeology.org.uk 365 March/April 2003 A NEOLITHIC FLAKED FLINT AXE FROM WALLINGTON Jonathan Cotton The axe figured here was passed to the writer for recording In May 2002. It had been found by John Erwood some ten months prior to this, during the construction of a rear extension to his house at 12 Leechcroft Road, Walllngton (TQ 2835 6513). The axe was located while digging a small soakaway 1.2m square connected with the building work. It had been placed edgeways In the ground with Its blade orientated to the east at a depth of 500mm from the surface; It lay some 200mm Into 'disturbed clay' beneath 400mm of topsoll. The geology hereabouts comprises the sands and clays of the Woolwich and Reading beds and small patches of sandy yellow-brown clay still adhere to several of the flake facets. The finder also noticed some animal bones at the same time as the discovery of the axe, though not apparently In direct association. It Is possible that these were of recent date. The axe was located In one corner of the soakaway and the act of prising It out of the section with a metal pickaxe slightly damaged the edge lying uppermost. (The position of the modern damage Is marked by an asterisk on the drawing.) Given Its recorded depth It Is conceivable that It was originally deposited In a shallow pit, though none was detected by the finder. -

English Monks Suppression of the Monasteries
ENGLISH MONKS and the SUPPRESSION OF THE MONASTERIES ENGLISH MONKS and the SUPPRESSION OF THE MONASTERIES by GEOFFREY BAS KER VILLE M.A. (I) JONA THAN CAPE THIRTY BEDFORD SQUARE LONDON FIRST PUBLISHED I937 JONATHAN CAPE LTD. JO BEDFORD SQUARE, LONDON AND 91 WELLINGTON STREET WEST, TORONTO PRINTED IN GREAT BRITAIN IN THE CITY OF OXFORD AT THE ALDEN PRESS PAPER MADE BY JOHN DICKINSON & CO. LTD. BOUND BY A. W. BAIN & CO. LTD. CONTENTS PREFACE 7 INTRODUCTION 9 I MONASTIC DUTIES AND ACTIVITIES I 9 II LAY INTERFERENCE IN MONASTIC AFFAIRS 45 III ECCLESIASTICAL INTERFERENCE IN MONASTIC AFFAIRS 72 IV PRECEDENTS FOR SUPPRESSION I 308- I 534 96 V THE ROYAL VISITATION OF THE MONASTERIES 1535 120 VI SUPPRESSION OF THE SMALLER MONASTERIES AND THE PILGRIMAGE OF GRACE 1536-1537 144 VII FROM THE PILGRIMAGE OF GRACE TO THE FINAL SUPPRESSION 153 7- I 540 169 VIII NUNS 205 IX THE FRIARS 2 2 7 X THE FATE OF THE DISPOSSESSED RELIGIOUS 246 EPILOGUE 273 APPENDIX 293 INDEX 301 5 PREFACE THE four hundredth anniversary of the suppression of the English monasteries would seem a fit occasion on which to attempt a summary of the latest views on a thorny subject. This book cannot be expected to please everybody, and it makes no attempt to conciliate those who prefer sentiment to truth, or who allow their reading of historical events to be distorted by present-day controversies, whether ecclesiastical or political. In that respect it tries to live up to the dictum of Samuel Butler that 'he excels most who hits the golden mean most exactly in the middle'. -

Read Ebook {PDF EPUB} Preparatory to Anglo-Saxon England Being the Collected Papers of Frank Merry Stenton by F.M
Read Ebook {PDF EPUB} Preparatory to Anglo-Saxon England Being the Collected Papers of Frank Merry Stenton by F.M. Stenton Preparatory to Anglo-Saxon England: Being the Collected Papers of Frank Merry Stenton by F.M. Stenton. Our systems have detected unusual traffic activity from your network. Please complete this reCAPTCHA to demonstrate that it's you making the requests and not a robot. If you are having trouble seeing or completing this challenge, this page may help. If you continue to experience issues, you can contact JSTOR support. Block Reference: #c8fec890-ce23-11eb-8350-515676f23684 VID: #(null) IP: 116.202.236.252 Date and time: Tue, 15 Jun 2021 21:51:05 GMT. Preparatory to Anglo-Saxon England: Being the Collected Papers of Frank Merry Stenton by F.M. Stenton. Our systems have detected unusual traffic activity from your network. Please complete this reCAPTCHA to demonstrate that it's you making the requests and not a robot. If you are having trouble seeing or completing this challenge, this page may help. If you continue to experience issues, you can contact JSTOR support. Block Reference: #c91a18c0-ce23-11eb-9d99-5b572480f815 VID: #(null) IP: 116.202.236.252 Date and time: Tue, 15 Jun 2021 21:51:05 GMT. Abbot of Peterborough. Abbot , meaning father, is an ecclesiastical title given to the male head of a monastery in various traditions, including Christianity. The office may also be given as an honorary title to a clergyman who is not the head of a monastery. The female equivalent is abbess. An abbey is a complex of buildings used by members of a religious order under the governance of an abbot or abbess. -

River Wandle at Merton Abbey, 2000 Mike Seaborne, Colour Coupler Print River Wandle Near Merton Abbey, 2018 John Chase, Pigment Print
Secret Rivers Large Print 1 Section 1 Secrets of the Thames 2 Display case 1. Middle Bronze Age skull 1260-900 BC Over 250 ancient human skeletal remains have been found along the Thames in London. The majority are prehistoric skulls. London’s rivers provided a focus for human activity including burials. These were susceptible to flooding and the bones washed out. The water current affects bones in different ways; skulls roll and often travel quite some distance. This skull has polishing and scraping, frontal tooth loss and stones wedged in the ear canal, all signs of river movement. Found on the foreshore at Mortlake 3 2. ‘Commentaries on London Mudlarking’, 2016 Roman nicolo glass intaglio This journal, created by Johnny Mudlark, is an illustrated record of his experiences and observations whilst mudlarking along the Thames. A permit is required to search the foreshore and finds must be reported to the Portable Antiquities Scheme. These pages of the journal show the discovery of the intaglio, which was originally set within a finger ring. The dolphin motif suggests a strong connection to the water. Found on the foreshore in the City of London Lent by Johnny Mudlark 4 3. Gilded copper-alloy mount 8th – 9th century Early Medieval Irish finds, such as this mount from a house-shaped shrine, are unusual in London. It was found at the site of a Viking river crossing at Putney. The Vikings travelled extensively using seas and rivers. Was this gilded mount traded or taken during a raid and brought to London? Found on the foreshore at Putney Lent by Bob Wells 5 4. -

Work and the Adolescent in Medieval England (AD 900-1550): the Osteological Evidence
Work and the adolescent in medieval England (AD 900-1550): the osteological evidence Article Accepted Version Lewis, M. (2016) Work and the adolescent in medieval England (AD 900-1550): the osteological evidence. Medieval Archaeology, 60 (1). pp. 138-171. ISSN 0076-6097 doi: https://doi.org/10.1080/00766097.2016.1147787 Available at http://centaur.reading.ac.uk/50828/ It is advisable to refer to the publisher’s version if you intend to cite from the work. See Guidance on citing . To link to this article DOI: http://dx.doi.org/10.1080/00766097.2016.1147787 Publisher: Taylor & Francis All outputs in CentAUR are protected by Intellectual Property Rights law, including copyright law. Copyright and IPR is retained by the creators or other copyright holders. Terms and conditions for use of this material are defined in the End User Agreement . www.reading.ac.uk/centaur CentAUR Central Archive at the University of Reading Reading’s research outputs online Work and the Adolescent in Medieval England (AD 900-1550). The osteological evidence. By Mary Lewis, University of Reading1 ABSTRACT WHAT WAS IT LIKE TO BE A TEENAGER IN MEDIEVAL ENGLAND? Despite the fact that medieval society often singled young apprentices and workers out for comment, their study has been largely neglected in medieval archaeology. The skeletal remains of 4940 adolescents (6.6-25 years) from 151 sites in medieval England was compiled from a combination of primary data collection and secondary data from published and unpublished skeletal reports and on-line databases. The aim was to explore whether apprentices could be identified in the archaeological record and if so, at what age they started work and what impact occupation had on their health. -

Amery Mills, Merton
Amery Mills, Merton The site of these mills was on the final part of the curved course of the Wandle where it turns to run eastwards alongside Merton High Street, and about 100 yards west of Merton Bridge. Just to the south-east was the site of Merton Priory, usually called Merton Abbey. The priory was established in about 1117 by Gilbert Norman, and he arranged for an existing mill thereabouts to be resited [1]. This was probably one of the two mills at Merton included in the Domesday survey. The next reference to the premises found was on 4 November 1534, when two mills on the site, called Amery Mills, were leased by the incumbent prior to William Moraunt for the term of 27 years [1]. Following the surrender of the priory property to Henry VIII in about 1540, the mills became separated from those estates. In 1558 John Pennon was granted a 27-year lease of the mills, but remained there until about 1600. Edward Ferrars acquired the property on 19 May 1609, and it later passed to Richard Burrell, who sold the mills to Sir Francis Clerke. Sir Francis also acquired the priory estates, and thus the mills became once more part of those estates [2]. On 19 June 1624 he conveyed all his estates at Merton to Rowland Wilson, a London vintner. Wilson died in 1654, and by his will proved on 1 June 1654 he bequeathed the properties to his wife Mary [3]. They subsequently passed to her grandson Ellis Crispe, who in 1668 sold them to Thomas Pepys [2]. -

Some Aspects of the History of Barnwell Priory: 1092-1300
SOME ASPECTS OF THE HISTORY OF BARNWELL PRIORY: 1092-1300 JACQUELINE HARMON A dissertation submitted for the degree of Doctor of Philosophy UNIVERSITY OF EAST ANGLIA SCHOOL OF HISTORY SEPTEMBER 2016 Contents Abstract iii Acknowledgements iv Abbreviations v-vi Maps vii Tables viii Figures viiii 1. Introduction 1 2. Historiography 6 3. Harleian 3601: The Liber Memorandorum 29 The Barnwell Observances 58 Record Keeping at Ely 74 Chronicles of local houses contemporary with the Liber 76 4. Scribal Activity at Barnwell 80 Evidence for a Library and a Scriptorium 80 Books associated with the Priory 86 The ‘Barnwell Chronicle’ 91 The Role of the Librarian/Precentor 93 Manuscript production at Barnwell 102 5. Picot the Sheriff and the First Foundation 111 Origins and Identity 113 Picot, Pigot and Variations 115 The Heraldic Evidence 119 Genealogy and Connections 123 Domesday 127 Picot and Cambridge 138 The Manor of Bourn 139 Relations with Ely 144 The Foundation of St Giles 151 Picot’s Legacy 154 i 6. The Peverels and their Descendants 161 The Peverel Legend 163 The Question of Co-Identity 168 Miles Christi 171 The Second Foundation 171 The Descent of the Barony and the Advowson of Burton Coggles 172 Conclusion 178 7. Barnwell Priory in Context 180 Cultural Exchange in the Tenth and Eleventh Centuries 180 The Rule of St Augustine 183 Gregorian Reform and the Eremetical Influence 186 The Effects of the Norman Conquest 190 The Arrival of the Canons Regular in England 192 The Early Houses 199 The Hierarchy of English Augustinian Houses 207 The Priory Site 209 Godesone and the Relocation of the Priory 212 Hermitages and Priories 214 8. -

Reports of Community Forums
Morden Community Forum Item 8 (a) 15 June 2010 Chair’s Report 18 residents attended, as well as 6 other councillors and officers of the council and its partners. Apologies were received from Mr Terrett and Councillor Karin Forbes 1. The Chairman, Councillor Maurice Groves, welcomed everyone to the meeting, and encouraged residents to bring more people to the meetings. He was looking to discuss a wider vision for Morden over the coming year. As examples of possible topics for discussion, he suggested a visit from a member of the Royal Institution for Town Planning, health services, carers, and heritage. 2. Action points from the previous meeting Elspeth Clarke said that it had been Field A at Morden Park that had been badly rutted because of heavy vehicles or early mowing. follow up the suggested bus lane in London Road with Transport for London (TfL). 3. Police update Inspector Matt Boyd said that there were a number of rumours current about possible cuts to Safer Neighbourhood Teams (SNT). These were only rumours at present. He suggested that if residents wanted answers to questions on policing matters at future meetings they should channel them through Bartle Sawbridge ([email protected] 020 8545 4400). The Borough Commander, Chief Superintendent Chris Bourlet was on secondment to another post for six months. His temporary replacement was Superintendent Nick Wolfenden. There had been a crime reduction in four of the wards covered by the forum, but increases of 2.9% in Ravensbury and 4.7% in St Helier. Morden now had 6111 members of CommunitySafe, the largest number in the borough. -

REBIRTH, REFORM and RESILIENCE Universities in Transition 1300-1700
REBIRTH, REFORM AND RESILIENCE Universities in Transition 1300-1700 Edited by James M. Kittelson and Pamela J. Transue $25.00 REBIRTH, REFORM, AND RESILIENCE Universities in Transition, 1300-1700 Edited by James M. Kittelson and Pamela]. Transue In his Introduction to this collection of original essays, Professor Kittelson notes that the university is one of the few institutions that medieval Latin Christendom contributed directly to modern Western civilization. An export wherever else it is found, it is unique to Western culture. All cultures, to be sure, have had their intellec tuals—those men and women whose task it has been to learn, to know, and to teach. But only in Latin Christendom were scholars—the company of masters and students—found gathered together into the universitas whose entire purpose was to develop and disseminate knowledge in a continu ous and systematic fashion with little regard for the consequences of their activities. The studies in this volume treat the history of the universities from the late Middle Ages through the Reformation; that is, from the time of their secure founding, through the period in which they were posed the challenges of humanism and con fessionalism, but before the explosion of knowl edge that marked the emergence of modern science and the advent of the Enlightenment. The essays and their authors are: "University and Society on the Threshold of Modern Times: The German Connection," by Heiko A. Ober man; "The Importance of the Reformation for the Universities: Culture and Confessions in the Criti cal Years," by Lewis W. Spitz; "Science and the Medieval University," by Edward Grant; "The Role of English Thought in the Transformation of University Education in the Late Middle Ages," by William J.