Community & Social Care Cranbrook & Loxford Cluster Profile 2015
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mondays Tuesdays Wednesdays Thursdays Fridays
Di’s Diamonds November 2017 – REGULAR ACTIVITIES Contact [email protected] or phone 020 8220 6000 or 07724508967 Please let me know which events you are attending so I can make arrangements for people to meet up. All activities are open to residents of all 3 boroughs unless stated. Mondays Tuesdays Wednesdays Thursdays Fridays Monday Movers 1.30- RSPB Bird Walks 9.30- Latin in a Line 10-11am Belhus Woods Volunteers Tap Dancing 9.30-11.45am 3.00pm HAVERING 11.30am 8.30am-12.30pm Line Dancing 12-1pm ONLY Veterans Lunch Club 12- Coffee Shop at 2.30pm Nature Conservation in Friendly Fridays 10am-1pm St Chads Church 10.30am- HAVERING ONLY 2pm Redbridge 10am-2.30pm Wednesday Workout 1.30- Walking Netball 10-11am Nature Conservation in 3pm HAVERING ONLY Coffee Shop at St Chads Redbridge 10am-2.30pm Short mat bowls 2-4pm Church 10.30am-12.30pm Short mat bowls 2-4pm Dementia Walk & Talk 11am YMCA Social Club 1-3pm Widows & Widowers Club 7.30pm Disabled Yoga11.30am- Card Making 1-3pm 1.00pm 50+ Yoga 1.30-2.30pm YMCA Social Club 1-3pm Tea Dance 1.30-3.30pm Walking Football 2-3pm Knitting and Crochet Group 2:15-3:15 pm Monday Movers 1.30-3.00pm Designed specifically for people with reduced mobility, ideal for wheelchair users. All exercises are chair based and individually tailored to your needs. £3.00 per session. To book call 01708 476554. HAD, Whittaker Hall, 1a Woodhall Crescent, Hornchurch, Essex, RM11 3NN Di’s Diamonds November 2017 – REGULAR ACTIVITIES Contact [email protected] or phone 020 8220 6000 or 07724508967 Please let me know which events you are attending so I can make arrangements for people to meet up. -

REDBRIDGE PHARMACIES August Bank Holiday Pharmacy Trading Name Address1 Address2 Postcode Tel No POLYSYSTEM WARD OPEN CLOSED
REDBRIDGE PHARMACIES August Bank Holiday Pharmacy Trading Name Address1 Address2 PostCode Tel No POLYSYSTEM WARD OPEN CLOSED ALLANS CHEMIST 1207 High Road CHADWELL HEATH RM6 4AL 020 8598 8815 SEVEN KINGS CHADWELL CLOSED ALLENS PHARMACY 19 Electric Parade GEORGE LANE E18 2LY 020 8989 3353 WANSTEAD CHURCH END BEEHIVE PHARMACY 8 Beehive Lane GANTS HILL IG1 3RD 020 8554 3560 CRANBROOK CRANBROOK 09:00 16:00 BOOTS THE CHEMISTS LTD 177-185 High Road ILFORD IG1 1DG 020 8553 2116 LOXFORD CLEMENTSWOOD BOOTS THE CHEMISTS LTD 39 High Street BARKINGSIDE IG6 2AD 020 8550 2743 FAIRLOP FULLWELL BOOTS THE CHEMISTS LTD 117-119 High Road ILFORD IG1 1DE 020 8553 0607 LOXFORD CLEMENTSWOOD BOOTS THE CHEMISTS LTD 172 George Lane South Woodford E18 1AY 020 8989 2274 WANSTEAD CHURCH END CLOSED BOOTS THE CHEMISTS LTD 169 Manford Way Hainault IG7 4DN 020 8500 4570 FAIRLOP HAINAULT BOOTS THE CHEMISTS LTD 59-61 High Street Wanstead E11 2AE 020 8989 0511 WANSTEAD SNARESBROOK BORNO CHEMISTS LTD 69 Perrymans Farm Road BARKINGSIDE IG2 7LT 020 8554 3428 SEVEN KINGS ALDBOROUGH BORNO CHEMISTS LTD 15 Broadway Market Barkingside IG6 2JU 020 8500 6714 FAIRLOP FULLWELL BRITANNIA PHARMACY 53 Green Lane ILFORD IG1 1XG 0208 478 0484 LOXFORD CLEMENTSWOOD BRITANNIA PHARMACY Loxford Polyclinic 417 ILFORD LANE IG1 2SN 0208 478 4347 LOXFORD LOXFORD 08:00 20:00 BRITANNIA PHARMACY 414-416 Green Lane SEVEN KINGS IG3 9JX 0208 590 6477 LOXFORD MAYFIELD 10:00 18:00 BRITANNIA PHARMACY 223 Ilford Lane ILFORD IG1 2RZ 020 8478 1756 LOXFORD LOXFORD CLOSED BRITANNIA PHARMACY 265 Aldborough Road -

Kids Sports Activities
KIDS SPORTS ACTIVITIES MONDAYS Time Class Age Venue Price Contact 4.30pm- Youth Fitness 11-16 yrs South Woodford Library £2.80 020 8708 9067 5.30pm & Gym (induction £11.40) www.visionrcl.org.uk 5pm-7pm Indoor Rowing 11-16 yrs Fairlop Rowing Club, £4 07932 636114 Fairlop Waters 6pm-7pm Learn to Swim 3 yrs+ Fullwell Cross £72 for 07941 674568 Leisure Centre 12 weeks [email protected] 6pm-7pm Boxing Under 11s Loxford Youth Centre £2.50 020 8708 0950 (non-contact) [email protected] 7pm-8pm Boxing 11 yrs+ Loxford Youth Centre £2.50 020 8708 0950 (non-contact) [email protected] 7pm-9.30pm Disability Youth 13-25 yrs Hainault Youth Centre £4 per month 020 8500 8071 Club session MONDAYS - FRIDAYS DAILY 3.30pm- Junior Gym 11-16 yrs Mayfield Leisure Centre £2.80 020 3887 0982 4.30pm (induction £12) & 4.30pm- 5.30pm TUESDAYS 3.15pm- Youth Club 11-19 yrs Hainault Youth Centre £4 per month 020 8500 8071 5.45pm session 4pm-5pm Youth Fitness 11-16 yrs Wanstead Leisure Centre £2.80 020 8989 1172 (induction £12) www.visionrcl.org.uk 4.30pm- Gladiator Fitness/ 11 yrs+ Ilford Sports Club £3.50 [email protected] 5.30pm Athletics & 1st session free Indoor Rowing 4pm-6pm Youth Fitness 11-16 yrs Fullwell Cross Leisure £2.50 020 8550 2366 Centre (induction £11.40) www.visionrcl.org.uk 5pm-6pm Youth Fitness 11-16 yrs Wanstead Leisure Centre £2.80 020 8989 1172 (induction £12) www.visionrcl.org.uk 5pm-7pm Table Tennis - 8-16 yrs Redbridge Sports & £6 or £10 per [email protected] Intermediates Leisure Centre week -

Buses from Gallions Reach Shopping Park
Gallions_Reach_Shopping_Park_DR_Spider.qxp 04/02/2021 19:37 Page 1 Buses from Gallions Reach Shopping Park 101 Wanstead Woodbine Place Wanstead Hail & Ride section Redbridge Falmouth Gardens 366 Blake Hall Road Redbridge Roding Lane South Redbridge Aldersbrook Road REDBRIDGE The Drive Forest Drive City of London Cemetery ILFORD Ilford Manor Park Ilford High Road Hainault Street Manor Park East Ham High Street North/ Ilford Romford Road Winston Way Primary School East Ham EAST HAM Sunnyside Road section Hail & Ride East Ham 262 Newham Town Hall Stratford Eton Road Bus Station STRATFORD East Ham Central Park Stratford Broadway South Park Drive N551 BARKING The yellow tinted area includes every bus Loxford Lane continues to East Ham High Street South Trafalgar Square Lonsdale Avenue stop up to one-and-a-half miles from Loxford Lane for Charing Cross West Ham Lane Gallions Reach Shopping Park. Main stops are shown in the white area outside. Barking St. Paul’s Cathedral Woolwich Manor Way Barking Town Centre Plaistow PLAISTOW Albatross Close Bank Barking Aldgate London Road/North Street Plaistow Woolwich Manor Way Tower Gateway Greengate Street Tollgate Road for Tower Hill Fleet Road The Highway Quay Road Newham University Hospital Beckton Tollgate Road 262 Prince Regent Lane District Park Kingsford Way Limehouse Beckton Showcase Cinema Limehouse Burdett Road East Beckton Beckton Triangle Tollgate Road Sainsbury’s Retail Park Poplar Prince Regent Lane Swallow Street All Saints Newham Way Canning Town Prince Regent Prince Regent Lane Keir Hardie -

Buses from Ilfordbuses from Ilford
Buses from Ilford Buses from Ilford 462 167 150 N86 123 continues to continues to continues to Chigwell Row continues to continues to Limes Farm Estate Loughton Harold Hill Wood Green 179 Tottenham Chingford Hainault Chigwell Hainault Harold Hill Police Station The Lowe Rise The Lowe Dagnam Park Drive 296 Tottenham Chingford Elmbridge Chigwell Hainault Romford Harold Hill Hale Green Road Fire Station Hilldene Avenue 364 Blackhorse Whitehall Forest Road Hainault Hainault Romford Rainham Straight Road Road Road for Fairlop Waters Road for Liberty Shopping Centre Road South Boulder Park Ballards Road Walthamstow Woodford Fairlop Fencepiece Road New North Romford Dagenham Gallows Bell Wells Murtwell Drive Road Bus Garage East Corner Hail & Ride section Forest Road Woodford Fullwell Cross Fencepiece Road Eastern Avenue Reede Road Gidea Park Wood Street Green for Leisure Centre New North Road West Main Road 128 169 86 Waterwork’s South Barkingside Claybury Fencepiece Road Rose Lane Estate Clayhall Parsloes Romford Corner Woodford High Street Broadway for Redbridge for Hurstleigh Avenue Sports Centre Gardens Hail & 396 Charlie Brown’s Ride Longwood Clayhall Fullwell Cross King George Billet Road Fullwell Avenue Becontree Romford Roundabout section Gardens Avenue for Leisure Centre Hospital Martins Corner for Liberty Shopping Centre 145 366 Leytonstone Redbridge Barkingside High Street Newbury Park Fullwell Cross Bennett’s Romford Stadium Roding for Leisure Centre Castle Lane Lane South Hail & Green Man Ride Redbridge Woodford Avenue Cranbrook -

Wanstead Flats
WANSTEAD FLATS Individual Site Plan Date 08/01/2020 Version Number V4 Review Date Author Fiona Martin/Geoff Sinclair Land Area 187 ha Compartment Number 38 Designations Epping Forest Land (1878 Act) Site of Special Scientific Interest (SSSI) Registered Park and Garden Archaeological Priority Area Site of Metropolitan Importance Locally Important Geological Site Green Belt Wanstead Flats Wanstead Flats INDIVIDUAL SITE PLAN SUMMARY Wanstead Flats forms the largest of the thirty-eight management compartments that comprise Epping Forest. It is an area of open acid grassland, sports pitches, heath, scrub, woodland, scattered trees and waterbodies, located at the southern end of Epping Forest; owned and managed by the City of London Corporation (COL). Wanstead Flats has a number of statutory designations and is a hugely important resource for the people of northeast London, both for its provision of sporting facilities and also for the opportunity to experience a natural environment within urban surroundings. It is one of the few breeding sites for Skylark (Alauda arvensis) in London and is a notable stop-off for migrating birds. It has a long and well-documented history, from the historical right of commoners to graze cattle and the inception of Epping Forest as a legal entity in 1878, through to World War II and modern times. Significant predicted housing growth is planned in the local area with consequent additional visitor pressure. This Individual Site Plan lists current management considerations but also presents a strategic work programme to ensure a sustainable future for the conservation and heritage interest of Wanstead Flats, along with its immense recreational value. -
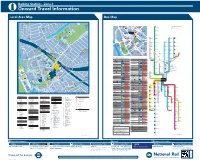
Buses from Barking
Barking Station – Zone 4 i Onward Travel Information Local Area Map Bus Map 1 Buses from Barking 74 400 LAVENDER PLACE FORSYTHIA CLOSE 2 56 Uphall School 5 BANKSIDE ROAD Playing Field 397 WISTERIA CLOSE 1 SOUTHBOURNE GARDENS 22 54 4 3 Y R O A D 2 55 Loxford 4 HARVE 37 Hall 70 LOXFORD LANE 16 24 Barking Abbey 36 The Lake Comprehensive School 23 B MEDWAY CLOSE U 169 1 T 415 T 1 FAN 1 S Other buses from Barking 12 SB Clayhall ROAD B 64 LAVENDER PLACE N U AZALEA CLOSE 11 EB R 1 3 NORMA SH for Hurstleigh Gardens 32 R Y 2 ST. LEONARDS GARDENS r 1 e RTHE Schoolday services: R t Barking Park ING NO RN R O RK E A PITTMAN GDNS a L A A JASMINE CLOSE 86 IEF WE N Loxford D W B D A N E R O A D R 48 W O Q Polyclinic rd A 687 towards Dagenham Park School o D A 13 f D x A VE Lo A WB O K 16 Barking Park R 44 24 1 F E UPHALL ROAD E R Fullwell Avenue S A X O N R O A D Tennis Courts I I 11 N 14 72 L E N G 10 S 15 E N 34 ROAD TULI D R O 18 I R D G A P G A R D E N S A S H L L M A I A H O R C G T 54 N A R T. -

Oliver Gill Statutory Proposal to Transfer
Children’s Services 91 Ray Lodge Road, Woodford Green, London, IG8 7PG Telephone: 020 8708 2240 Email: [email protected] Please ask for: Oliver Gill Statutory Proposal to transfer The Constance Bridgeman Centre to a new site at Loxford Youth Centre, Loxford Lane, Ilford, IG1 2NS. Notice is given that the London Borough of Redbridge intends to make a prescribed alteration to The Constance Bridgeman Centre, East Wing, NCC Redbridge Campus, Chadwell Heath Lane, Romford, RM6 4XT, from 1 September 2021. Contact Details Name and address of Local Authority publishing the proposal: London Borough of Redbridge, Lynton House, 255-259 High Road, Ilford IG1 1NN Name, address and category of school that is the subject of the proposal: The Constance Bridgeman Centre (Community), East Wing, NCC Redbridge Campus, Chadwell Heath Lane, Romford, RM6 4XT Contact details during statutory representation period: This consultation begins on Monday 19 April 2021 and concludes on Monday 17 May 2021. Any person may object to or make comments on the proposals by sending representations to: SEND Commissioning, The Constance Bridgeman Centre, East Wing, NCC Redbridge Campus, Chadwell Heath Lane, Romford, RM6 4XT Email: [email protected] Web: https://engagement.redbridge.gov.uk/ A virtual public consultation event will be held online, on Monday 10 May at 18:30. The link for this event is: https://teams.microsoft.com/l/meetup- join/19%3ameeting_OGVjNTFmZjMtZGM5OS00ZWE1LTk0NTEtMDI4ZDQ2Njc5MW Yw%40thread.v2/0?context=%7b%22Tid%22%3a%222a8b2c16-2e9e-4dce-a97b- a0b34e803a22%22%2c%22Oid%22%3a%22e3c3abfc-69ab-430d-8d97- 4506d3acec34%22%2c%22IsBroadcastMeeting%22%3atrue%7d&btype=a&role=a All interested parties are welcome to attend this event, where presentations by London Borough of Redbridge staff will be followed by the opportunity to ask questions and/or provide direct feedback. -

Redbridge Pharmacies Open for May 2018 Bank Holidays
Redbridge Pharmacies Open for May 2018 Bank Holidays Opening Times Opening Times Pharmacy Name Address Tel. No. Monday 7th May Monday 28th May LLOYDS PHARMACY King George Avenue, Newbury Park, IG2 7SH 020 8550 5189 10 AM-4 PM 10 AM-4 PM Boots 172 George Lane, South Woodford, E18 1AY 020 8989 2274 10 AM-4 PM 10 AM-4 PM Britannia Pharmacy 265 Aldborough Road South, Seven Kings, IG3 8JB 020 8590 2353 8 AM- 8 PM 8 AM-8 PM Wanstead Pharmacy 75-77 High Street, Wanstead, E11 2AE 020 8989 0597 10 AM-2 PM 10 AM-2 PM Boots 59-61 High Street, Wanstead, E11 2AE 020 8989 0511 10 AM-5 PM 10 AM-5 PM Gold's Pharmacy 24 Seven Ways Parade, Woodford Avenue,IG2 6JX 020 8550 1050 9:30 AM-10 PM 9:30 AM-10 PM Boots 177-185 High Road, Ilford, IG1 1DG 020 8553 2116 9 AM-6 PM 9 AM-6 PM Fairlop Pharmacy 87 High Street, Barkingside, IG6 2AH 020 8551 3017 12 PM-Midnight 12 PM-Midnight Ocean Healthcare 12 High Road, South Woodford, E18 2QL 020 8989 5960 9 AM-10 PM 9 AM-10 PM Beehive Pharmacy 8 Beehive Lane, Ilford, IG1 3RD 020 8554 3560 9 AM-5 PM 9 AM-5 PM Tesco Store 796 Cranbrook Road, Barkingside, IG6 1HY 020 8218 7849 9 AM-6 PM 9 AM-6 PM Tesco Stores Southend Road, Woodford Green, IG8 8GE 0345 677 9733 9 AM-6 PM 9 AM-6 PM Tesco Pharmacy 822 High Road, Chadwell Heath, RM6 4HY 020 3801 3932 9 AM-6 PM 9 AM- 6 PM Britannia Pharmacy 414-416 Green Lane, Seven Kings, IG3 9JX 020 8590 6477 10 AM-6 PM 10 AM-6 PM Boots 117 High Road, Ilford, Essex, IG1 1DE 020 8553 0607 11 AM-5 PM 11 AM-5 PM Britannia Pharmacy Loxford Polyclinic, 417 Ilford Lane, Ilford, IG1 2SN 0208 478 4347 8 AM-8 PM 8 AM-8 PM These hours have been verified; however it is still advisable to check that the pharmacy is open first. -

Buses from Ilford East
Buses from Ilford East Clayhall The Glade HAINAULT 150 169 Fullwell Avenue Hainault Hainault Chigwell The Lowe Row 128 Fencepiece Road Claybury Broadway Fullwell Cross Clayhall Avenue Key Barkingside High Street/Freemantle Road Ø— Connections with London Underground Redbridge BARKINGSIDE Î Roding Way South/ Barkingside Magistrate’s Court Connections with Docklands Light Railway Falmouth Gardens u Connections with London Overground Hail & Ride Barkingside R section Connections with National Rail Falmouth Gardens Cranbrook Road Vista Drive Horns Road Princes Road 366 Gantshill Crescent Horns Road Aldwych Avenue REDBRIDGE Redbridge Lane East GANTS Horns Road Hamilton Avenue Redbridge HILL Eastern Avenue Horns Road Emmott Avenue The yellow tinted area includes every bus stop A The Drive Leytonstone Wanstead Gants Hill Horns Road Perrymans Farm Road up to one-and-a-half miles from Ilford East. Red discs show the bus stop you need for your chosen bus Main stops are shown in the white area outside. service. The disc !A appears on the top of the bus stop in the 145 Leytonstone Redbridge Ley Street Eastern Avenue 1 2 3 Green Man Eastern Avenue Valentine’s Mansion and Park 4 5 6 street (see map of town centre in centre of diagram). Roundabout The Drive Cranbrook Primary School Cranbrook Road Ley Street Parklands Close H&R Bethell Avenue Route 366 operates as Hail & Ride on the sections of LEYTONSTONE The Drive Ley Street Perth Road roads markedH&R on the map. St Andrew’s Church Valentine’s Ley Street Benton Road HAROLD Buses stop at any safe point along the road. The Drive Park Seymour Gardens Please indicate clearly to the driver when you wish to BENTON ROAD HILL N86 Harold Hill board or alight. -
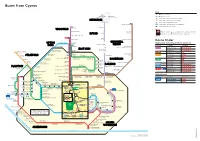
Buses from Cyprus
REDBRIDGE WANSTEAD ILFORD UPTON CHADWELL PARK HEATH EAST HAM STRATFORD DAGENHAM BARKING PLAISTOW NORTH WOOLWICH SILVERTOWN Buses from Cyprus Key 101 Day buses in black 366 Redbridge Redbridge N551 Night buses in blue Roding Lane South Falmouth Gardens —O Connections with London Underground REDBRIDGE o Connections with London Overground Hail & Ride Redbridge section R Connections with National Rail 173 King George Hospital D Connections with Docklands Light Railway 101 B Connections with river boats The Drive WANSTEAD Wanstead Aldersbrook Road Little Heath Red discs show the bus stop you need for your chosen bus Ilford Barley Lane service. The disc appears on the top of the bus stop in the ILFORD street (see map of town centre in centre of diagram). City of London Cemetery 24 hour 474 service Ilford Manor Park Town Centre Chadwell Heath Lane Route finder Plashet Grove Manor Park CHADWELL UPTON Hail & Ride section Day buses including 24-hour services Broadway Sunnyside Road HEATH PARK Upton Park 300 Bus route Towards Bus stops East Ham Chadwell Heath EAST HAM High Road, Whalebone Lane South 101 Gallions Reach BHKMN Upton Park Boleyn East Ham Eton Road Wanstead DLPQW Stratford West Ham United F.C. High Street North 262 Bus Station 173 King George Hospital D East Ham Becontree Heath Stratford Boundary Road Morrisons East Beckton BH STRATFORD Wilson Road 376 Newham Park Avenue South Park Drive 262 Broadway Town Hall Nelson Street Stratford C +J East Ham Barking Road Park Avenue Boundary Road High Street South, Tilbury Road Plaistow Altmore -
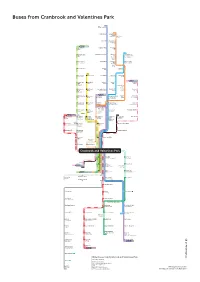
Buses from Cranbrook and Valentines Park
Buses from Cranbrook and Valentines Park EM 167 E AD R Loughton RO S O ’S N E G OR AD E RO . G T 462 S REW’S D Roding Road Limes Farm AN E. Estate . T AV S ELL R Coppereld Hail & Ride H O BET section A Valentines D Park VAUGHAN GARDENS Valley Hill Manor Road RD St. Winifred’s R E Church T ©P1ndar S S E N COWLEY ROAD HOLCOMBE H E C D 123 O R DON GARDENSENS R A EN RD Wood Green Loughton Way Grange G T AR Hill H L H GA E C AG S EL DN N G A E C FF R S R LI 150 EN C A RD D D Turnpike Lane Buckhurst Hill Manford Chigwell Row A E N G R R H Way for Hainault Forest DS IVE B AN IS Manford Country Park GHL D R I N O Primary H S S E NS N V E O School D N S D The Lake E K G N S CA R D ES ROAD E N N Lordship Lane Roding Lane Manford Manford Way E R GA D E P A The Roundway Way Manford Cross R NTI G D S O A R Hainault H N LE E G A E N L VA Health G D A IL E S T R R N H&R1 Centre V S O N A E E K O G C M T D U D Bruce Grove Chigwell Hainault A Y G R N R S E H A E Rise The Lowe N G GR Y S I I G V E R H&R2 S E A U .