Methods of Disinfecting Stethoscopes: Systematic Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Chemical Disinfectants for Biohazardous Materials (3/21)
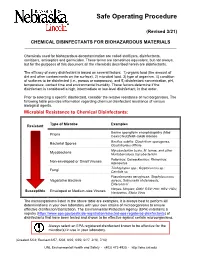
Safe Operating Procedure (Revised 3/21) CHEMICAL DISINFECTANTS FOR BIOHAZARDOUS MATERIALS ____________________________________________________________________________ Chemicals used for biohazardous decontamination are called sterilizers, disinfectants, sanitizers, antiseptics and germicides. These terms are sometimes equivalent, but not always, but for the purposes of this document all the chemicals described herein are disinfectants. The efficacy of every disinfectant is based on several factors: 1) organic load (the amount of dirt and other contaminants on the surface), 2) microbial load, 3) type of organism, 4) condition of surfaces to be disinfected (i.e., porous or nonporous), and 5) disinfectant concentration, pH, temperature, contact time and environmental humidity. These factors determine if the disinfectant is considered a high, intermediate or low-level disinfectant, in that order. Prior to selecting a specific disinfectant, consider the relative resistance of microorganisms. The following table provides information regarding chemical disinfectant resistance of various biological agents. Microbial Resistance to Chemical Disinfectants: Type of Microbe Examples Resistant Bovine spongiform encephalopathy (Mad Prions Cow) Creutzfeldt-Jakob disease Bacillus subtilis; Clostridium sporogenes, Bacterial Spores Clostridioides difficile Mycobacterium bovis, M. terrae, and other Mycobacteria Nontuberculous mycobacterium Poliovirus; Coxsackievirus; Rhinovirus; Non-enveloped or Small Viruses Adenovirus Trichophyton spp.; Cryptococcus sp.; -
EH&S COVID-19 Chemical Disinfectant Safety Information
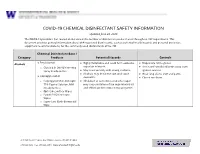
COVID-19 CHEMICAL DISINFECTANT SAFETY INFORMATION Updated June 24, 2020 The COVID-19 pandemic has caused an increase in the number of disinfection products used throughout UW departments. This document provides general information about EPA-registered disinfectants, such as potential health hazards and personal protective equipment recommendations, for the commonly used disinfectants at the UW. Chemical Disinfectant Base / Category Products Potential Hazards Controls ● Ethyl alcohol Highly flammable and could form explosive Disposable nitrile gloves Alcohols ● ● vapor/air mixtures. ● Use in well-ventilated areas away from o Clorox 4 in One Disinfecting Spray Ready-to-Use ● May react violently with strong oxidants. ignition sources ● Alcohols may de-fat the skin and cause ● Wear long sleeve shirt and pants ● Isopropyl alcohol dermatitis. ● Closed toe shoes o Isopropyl Alcohol Antiseptic ● Inhalation of concentrated alcohol vapor 75% Topical Solution, MM may cause irritation of the respiratory tract (Ready to Use) and effects on the central nervous system. o Opti-Cide Surface Wipes o Powell PII Disinfectant Wipes o Super Sani Cloth Germicidal Wipe 201 Hall Health Center, Box 354400, Seattle, WA 98195-4400 206.543.7262 ᅵ fax 206.543.3351ᅵ www.ehs.washington.edu ● Formaldehyde Formaldehyde in gas form is extremely Disposable nitrile gloves for Aldehydes ● ● flammable. It forms explosive mixtures with concentrations 10% or less ● Paraformaldehyde air. ● Medium or heavyweight nitrile, neoprene, ● Glutaraldehyde ● It should only be used in well-ventilated natural rubber, or PVC gloves for ● Ortho-phthalaldehyde (OPA) areas. concentrated solutions ● The chemicals are irritating, toxic to humans ● Protective clothing to minimize skin upon contact or inhalation of high contact concentrations. -
For Peer Review Only - Page 1 of 27 BMJ Open
BMJ Open BMJ Open: first published as 10.1136/bmjopen-2015-010387 on 4 April 2016. Downloaded from FALSIFIED MEDICINES IN PERU: A Retrospective Review (1997-2014). ForJournal: peerBMJ Open review only Manuscript ID bmjopen-2015-010387 Article Type: Research Date Submitted by the Author: 27-Oct-2015 Complete List of Authors: Medina, Edwin; University of Barcelona - Faculty of Pharmacy, Department of Pharmacy and Pharmaceutical Technology Bel, Elvira; University of Barcelona - Faculty of Pharmacy, Department of Pharmacy and Pharmaceutical Technology Suñé, Josep María; University of Barcelona - Faculty of Pharmacy, Department of Pharmacy and Pharmaceutical Technology <b>Primary Subject Public health Heading</b>: Secondary Subject Heading: Global health, Epidemiology, Health policy, Health services research Keywords: Safety, Falsified, Medicines, Alerts, counterfeit, Drugs http://bmjopen.bmj.com/ on September 24, 2021 by guest. Protected copyright. For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml Page 1 of 27 BMJ Open BMJ Open: first published as 10.1136/bmjopen-2015-010387 on 4 April 2016. Downloaded from 1 2 3 FALSIFIED MEDICINES IN PERU: A Retrospective Review (1997-2014). 4 5 6 7 Authors: Edwin Medina1, Elvira Bel1, Josep María Suñé1 8 9 10 11 12 Affiliations: 13 14 15 1. DepartmentFor of peerPharmacy and review Pharmaceutical onlyTechnology, Faculty of 16 Pharmacy, University of Barcelona, Spain 17 18 19 20 Corresponding author: 21 22 Edwin Salvador Medina Vargas 23 24 Department of Pharmacy and Pharmaceutical Technology 25 Faculty of Pharmacy 26 University of Barcelona 27 Joan XXIII, s/n, 08028 Barcelona 28 29 Spain 30 Email: [email protected] 31 32 33 http://bmjopen.bmj.com/ 34 Keywords: Safety, Falsified, Medicines, Alerts, counterfeit, Drugs 35 36 37 38 39 Word Count 40 41 Abstract: 298 on September 24, 2021 by guest. -

Use of 90% Ethanol to Decontaminate Stethoscopes in Resource Limited
Raghubanshi et al. Antimicrobial Resistance and Infection Control (2017) 6:68 DOI 10.1186/s13756-017-0224-x RESEARCH Open Access Use of 90% ethanol to decontaminate stethoscopes in resource limited settings Bijendra Raj Raghubanshi, Supriya Sapkota, Arjab Adhikari*, Aman Dutta, Utsuk Bhattarai and Rastriyata Bhandari Abstract Background: In developing countries like Nepal, 90% ethanol is cheap and is available in most hospitals. The unavailability of isopropyl alcohol (IPA) in these settings led us to compare the efficacy between 90% ethanol and isopropyl alcohol pads in reducing the bacterial contamination of diaphragm of stethoscope. Methods: A randomized blinded experimental study was carried out to determine the difference between cleaning stethoscopes with 90% ethanol and IPA. Cultures of diaphragm were taken before and after cleaning with one of the cleaning agent. Colony forming units (CFU) count and organism identification was done by a blinded investigator. CFU before and after cleaning were compared using Wilcoxon signed–rank test. Mann Whitney U test was used to compare the decrease in CFU count between the cleaning agents. Results: About 30% of the stethoscopes harbored potential pathogens. Significant reduction in CFU was observed with both IPA (Wilcoxon signed–rank test, P value <0.001) and 90% ethanol (Wilcoxon signed–rank test, P value <0. 001). Comparing median decrease in CFU between cleaning with IPA and with 90% ethanol, no significant difference was found (Mann Whitney U test; U = 1357, P value >0.05). Conclusions: Both 90% ethanol and IPA are equally effective in decontaminating the diaphragm of stethoscope. Selection of agent should be done on the basis of cost and availability. -

Hydroxy- -Methylbutyrate (Hmb)
(19) *EP003373740B1* (11) EP 3 373 740 B1 (12) EUROPEAN PATENT SPECIFICATION (45) Date of publication and mention (51) Int Cl.: of the grant of the patent: A23K 10/10 (2016.01) A23L 33/10 (2016.01) 24.02.2021 Bulletin 2021/08 (86) International application number: (21) Application number: 16864978.8 PCT/US2016/061278 (22) Date of filing: 10.11.2016 (87) International publication number: WO 2017/083487 (18.05.2017 Gazette 2017/20) (54) COMPOSITIONS AND METHODS OF USE OF -HYDROXY- -METHYLBUTYRATE (HMB) AS AN ANIMAL FEED ADDITIVE ZUSAMMENSETZUNGEN UND VERFAHREN ZUR VERWENDUNG VON BETA-HYDROXY-BETA-METHYLBUTYRAT (HMB) ALS FUTTERZUSATZ COMPOSITIONS ET PROCÉDÉS D’UTILISATION DE -HYDROXY- -MÉTHYLBUTYRATE (HMB) COMME ADDITIF D’ALIMENT POUR ANIMAUX (84) Designated Contracting States: • BAIER, Shawn AL AT BE BG CH CY CZ DE DK EE ES FI FR GB Polk City, Iowa 50226 (US) GR HR HU IE IS IT LI LT LU LV MC MK MT NL NO PL PT RO RS SE SI SK SM TR (74) Representative: Evans, Jacqueline Gail Victoria Marches Intellectual Property Limited (30) Priority: 10.11.2015 US 201562253428 P Wyastone Business Park Wyastone Leys (43) Date of publication of application: Ganarew 19.09.2018 Bulletin 2018/38 Monmouth NP25 3SR (GB) (73) Proprietor: Metabolic Technologies, Inc. (56) References cited: Ames, IA 50010 (US) WO-A1-2004/037010 US-A- 5 028 440 US-A- 5 087 472 US-A- 5 087 472 (72) Inventors: US-A- 6 103 764 US-A1- 2014 249 223 • FULLER, John US-A1- 2015 025 145 Zearing, Iowa 50278 (US) • RATHMACHER, John Story City, Iowa 50248 (US) Note: Within nine months of the publication of the mention of the grant of the European patent in the European Patent Bulletin, any person may give notice to the European Patent Office of opposition to that patent, in accordance with the Implementing Regulations. -

Chemical Disinfectant and Cleaning Agent Safety – Frequently Asked Questions
Caribbean Public Health Agency Technical Guidance: COVID-19 Series No 33 Chemical Disinfectant and Cleaning Agent Safety – Frequently Asked Questions Suggested Citation: CARPHA. (2020). Chemical disinfectant and cleaning agent safety – frequently asked questions. Caribbean Public Health Agency Technical Guidance: COVID-19 Series, no. 33. CARPHA 2020 Chemical Disinfectant and Cleaning Agent Safety – Frequently Asked Questions 9 July 2020 Why are we concerned about cleaning agents and disinfectants? Selecting the correct chemical agent for cleaning and disinfecting and safely handling and using that agent is essential to health and wellbeing. Recently, with the increased focus on cleaning to reduce the risk of exposure to coronavirus disease, there have been an associated increase in media stories warning the public of the dangerous chemicals used for disinfectants. All chemical cleaning agents can be harmful to the health of the person using the product if it is not used as directed on the label by the manufacturer. Chemical agents can cause burns, breathing difficulties or damage to the lungs, or possibly result in poisoning. Persons should carefully read instructions for use, safety data sheets, and any health warnings to ensure they have selected the correct chemical agents, have the appropriate personal protection, and use and store the chemicals in a safe way. What are the properties of effective chemical cleaning agents and disinfectants? A wide variety of chemical agents can be used for cleaning, sanitising, and disinfecting. There are 4 categories of cleaners: detergents, degreasers, abrasives, and acids. Each is effective for cleaning different surfaces depending on the type of soiling. Different chemical agents are effective for killing different bacteria and viruses.1 Molds and fungus will require a sporicidal agent2. -

Amoxicillin in Water: Insights Into Relative Reactivity, Byproduct Formation, and Toxicological Interactions During Chlorination
applied sciences Article Amoxicillin in Water: Insights into Relative Reactivity, Byproduct Formation, and Toxicological Interactions during Chlorination Antonietta Siciliano 1 , Marco Guida 1 , Giovanni Libralato 1 , Lorenzo Saviano 1, Giovanni Luongo 2 , Lucio Previtera 3, Giovanni Di Fabio 2 and Armando Zarrelli 2,* 1 Department of Biology, University of Naples Federico II, 80126 Naples, Italy; [email protected] (A.S.); [email protected] (M.G.); [email protected] (G.L.); [email protected] (L.S.) 2 Department of Chemical Sciences, University of Naples Federico II, 80126 Naples, Italy; [email protected] (G.L.); [email protected] (G.D.F.) 3 Associazione Italiana per la Promozione delle Ricerche su Ambiente e Salute umana, 82030 Dugenta, Italy; [email protected] * Correspondence: [email protected]; Tel.: +39-08-167-4472 Abstract: In recent years, many studies have highlighted the consistent finding of amoxicillin in waters destined for wastewater treatment plants, in addition to superficial waters of rivers and lakes in both Europe and North America. In this paper, the amoxicillin degradation pathway was investigated by simulating the chlorination process normally used in a wastewater treatment plant to reduce similar emerging pollutants at three different pH values. The structures of 16 isolated Citation: Siciliano, A.; Guida, M.; degradation byproducts (DPs), one of which was isolated for the first time, were separated on a Libralato, G.; Saviano, L.; Luongo, G.; C-18 column via a gradient HPLC method. Combining mass spectrometry and nuclear magnetic Previtera, L.; Di Fabio, G.; Zarrelli, A. resonance, we then compared commercial standards and justified a proposed formation mechanism Amoxicillin in Water: Insights into beginning from the parent drug. -

HIV-2 BLOT 1.2 Instructions for Use
HIV-2 BLOT 1.2 Instructions For Use FOR RESEARCH USE ONLY NOT FOR USE IN DIAGNOSTIC PROCEDURES REVISION DATE: 2017/05 Note Changes Highlighted MAC0012-ENG-1 (18 Tests): 11022-018 (36 Tests): 11022-036 NAME AND INTENDED USE The MP DIAGNOSTICS HIV-2 BLOT 1.2 is a qualitative enzyme immunoassay for in-vitro detection of specific antibodies to HIV-2 in human serum or plasma. This test kit is supplied for research purposes only. It is not intended for use in the diagnosis or prognosis of disease. In particular, this test cannot be used to evaluate blood specimens for the purposes of donor screening or as a confirmatory diagnostic. INTRODUCTION The MP Diagnostics HIV-2 BLOT 1.2 kit is intended as a supplemental antibody assay for Research Use Only. Human Immunodeficiency Virus Type 2 (HIV-2) infection was first described in 1985 in asymptomatic prostitutes from Senegal. The virus was subsequently isolated in 1986 from patients with AIDS-like symptoms in Guinea Bissau and Cape Verde. HIV-2 is related to, but distinct from HIV-1, the prototype AIDS virus. As such HIV-2 has many molecular, biological and serological similarities with HIV-1. Reports have shown that the infection is not limited to Africa and that HIV-2 seropositive individuals have been identified in Europe and the United States. DESCRIPTIONS OF SYMBOLS USED The following are graphical symbols used in or found on MP Diagnostics products and packaging. These symbols are the most common ones appearing on medical devices and their packaging. Some of the common symbols are explained in more detail in European Standard BS EN 980:2008 and International Standard ISO 15223-1:2007. -

VOLUME 2 Cleaning Agents, Sanitisers and Disinfectants in Food Businesses: Detection of Traces and Human Risk Assessment Processes
Chemicals in Food Hygiene VOLUME 2 Cleaning agents, sanitisers and disinfectants in food businesses: detection of traces and human risk assessment processes Chemicals in Food Hygiene – Volume 2 Foreword The Global Food Safety Initiative (GFSI) is a considering carry-over risks of traces in non-profit industry association tasked with foods; promoting continuous improvement of food ➢ Reviewed and identified gaps in the safety management systems to ensure suitability of existing methods for confidence in the delivery of safe food to detection of traces at relevant points in consumers worldwide. GFSI provides a the food production process; platform for collaboration between some of ➢ Developed the GFSI position on the use of the world’s leading food safety experts from cleaning agents, sanitisers and retailer, producers and food service disinfectants and the relationship with companies, service providers associated with microbial resistance. the food supply chain, international organisations, academia and government. The TWG produced 2 volumes within one document: Since GFSI’s inception in 2000, experts from all over the world have been collaborating in ➢ Volume one of this document provides a numerous Technical Working Groups (TWG) high-level overview of the considerations to tackle current food safety issues defined that a food business operator needs to by GFSI stakeholders. In 2017 a TWG was consider in relation to ensuring established to determine best practices in appropriate hygienic practices. This relation to biocides (defined as the residues volume is aimed at a variety of readers from cleaning agents, sanitisers and from the food truck operator or farmer disinfectants) in the food supply chain. -

Sodium Hypochlorite
SODIUM HYPOCHLORITE What is SODIUM HYPOCHLORITE? Sodium hypochlorite is a liquid with an odor of chlorine. Usually it is clear but some solutions are greenish to yellow in color. Other names for sodium hypochlorite include Clorox , bleach, liquid bleach, sodium oxychloride, Javex, antiformin, showchlon, Chlorox, B-K, Carrel-Dakin Solution, Chloros, Dakin’s Solution, hychlorite, Javelle Water, Mera Industries 2MOm≥B, Milton, modified Dakin’s Solution, Piochlor, and 13% active chlorine. Where can sodium hypochlorite be found and how is it used? Sodium hypochlorite is mainly used as a bleaching agent or disinfectant. A disinfectant kills bacteria that can carry diseases. It is found in consumer and commercial bleaches, cleaning solutions, and disinfectants for drinking water, wastewater and swimming pools. How can people be exposed to sodium hypochlorite? You could be exposed to sodium hypochlorite through: Breathing fumes while using products containing sodium hypochlorite. Drinking water from public drinking water supplies where these chemicals were added to kill bacteria. You could also be exposed by drinking sodium hypochlorite by accident. Touching sodium hypochlorite if gloves are not worn when using products containing it. Eye Contact by splashing sodium hypochlorite during use. People who work where sodium hypochlorite is used to bleach paper and textiles may have slightly higher levels of exposure in all of the above areas. How does sodium hypochlorite work and how can it affect my health? Sodium hypochlorite is a corrosive substance, meaning that it will eat away at materials it contacts. Accidental sodium hypochlorite poisoning can be deadly. Severe injuries can occur to the mouth, throat, esophagus and stomach. -

Kinetic Studies on Oxidative Dissolution of Elemental Mercury in Aqueous Sodium Hypochlorite
International Journal of Environmental Science and Development, Vol. 7, No. 7, July 2016 Kinetic Studies on Oxidative Dissolution of Elemental Mercury in Aqueous Sodium Hypochlorite S. Bandyopadhyay, S. Chakraborty, D. B. Zaini, and S. Bhattacharjee mercury and second order reaction kinetics was observed Abstract—Aqueous sodium hypochlorite is often used to between elemental mercury and free chlorine. detoxify solid wastes containing elemental mercury and its Solid wastes are often treated with aqueous sodium compounds by oxidative dissolution of mercury in the form of a hypochlorite to remove mercury and its compounds. Brine soluble mercurochloro complex. Experiments were conducted to estimate global kinetics and interfacial mass transfer mud of a chlor-alkali industry containing elemental mercury parameters of the reaction between elemental mercury and and its salts is a solid waste and is usually dumped off-site in a aqueous sodium hypochlorite. The reaction did not conform to lined pond. Sometimes this brine mud is treated with aqueous either pure mass transfer or pure instantaneous reaction sodium hypochlorite to remove toxic mercury from the sludge. regimes. The order and activation energy of the reaction were This is a solid-liquid reaction and involves mass transfer of -1 estimated to be 1.168 and 13.48 kJ mol respectively. mercury from the solid matrix into a liquid phase. Sizeneva et Experimental data on reaction enhancement factors may be used al. [10] studied oxidative dissolution of Hg0 in NaOCl at pH for design of an industrial solid waste detoxification reactor. 0 0 5.9, 6.5, 6.9 and 8.5 at 25 C and 50 C. -

Knolltextiles Cleaning Information
Cleaning Information Regular Maintenance It is important to vacuum upholstery regularly to remove the surface dust that builds up and slowly contributes to a greying effect that diminishes the clarity of the original color. Please note that vacuuming should be done with the proper attachments to avoid breaking down the fibers and contributing to “pilling.” In addition to regular vacuuming, a professional cleaner should come in at least once or twice a year to thoroughly clean the fabrics and remove the soiling that a normal vacuum cleaner cannot reach. The expense of this service is small compared to the reward of seating that looks good as new after a lot of use. Cleaning Codes W: Water-based cleaning agents or foam may be used for cleaning this fabric. S: Only mild, pure water-free dry cleaning solvents may be used for cleaning this fabric. W-S: Water-based cleaning agents and foam or mild, waterfree solvents may be used for cleaning this fabric. W Bleach: Water-based or foam cleaning agents or diluted household bleach may be used for cleaning this fabric. W-S Bleach: Clean with water or solvent-based cleaning agents or diluted household bleach. X: This fabric should be vacuumed or brushed lightly to remove soil. Warning: Do not use water-based foam or liquid cleaning agents of any type on this fabric. Cleaning vs Sanitizing vs Disinfecting Cleaning, disinfecting and sanitizing are often used synonymously, but they are not the same thing. Cleaning removes the visible foreign matter from a surface. Disinfecting, when done according to the instructions of a suitable cleaner, kills all bacteria and viruses present, while sanitizing reduces the level of bacteria and viruses present.