Ill-Defined Macule on the Abdomen
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Kaposiform Hemangioendothelioma with Kasabach-Merritt Syndrome Mistaken for Child Abuse in a Newborn
Kaposiform Hemangioendothelioma With Kasabach-Merritt Syndrome Mistaken for Child Abuse in a Newborn Amanda A. Cyrulnik, MD; Manju C. Dawkins, MD; Gert J. Smalberger, MD; Scott Young, MD; Ranon E. Mann, MD; Mark I. Jacobson, MD; Adam J. Friedman, MD Practice Points Vascular tumors in dermatology may mimic child abuse. Even when all signs favor abuse, a nonresolving lesion should alarm clinicians to consider an alter- nate diagnosis. Kasabach-Merritt syndrome is a serious and potentially life-threatening condition that requires prompt evaluation. Kaposiform hemangioendotheliomaCUTIS is a rare vas- elevated D-dimer levels, confirming a diagnosis of cular neoplasm of childhood that may have an Kasabach-Merritt syndrome (KMS). alarming and potentially misleading clinical pre- Cutis. 2014;93:E17-E20. sentation. Awareness of this entity is important to provide appropriate and immediate medical care. Case Report We report the case of a 24-day-old female new- A 24-day-old female newborn presented to a hospi- born who presented with a large bruiselike lesion tal with a large bruiselike lesion on the left leg. A on theDo left leg. A diagnosis ofNot cellulitis suspected diagnosis Copy of cellulitis suspected to be secondary to to be secondary to child abuse was made and the child abuse was made and the patient subsequently patient subsequently was placed in foster care; was placed in foster care; however, the lesion did not however, the lesion did not resolve after treatment resolve after treatment and relocation. At 69 days of and relocation. On reevaluation at our institution, age, the patient was readmitted, now to our hospi- physical examination revealed a round, 34-cm, tal, after the lesion persisted and had progressively violaceous, indurated, fixed, nonblanching, non- expanded. -

Glomus Tumor in the Floor of the Mouth: a Case Report and Review of the Literature Haixiao Zou1,2, Li Song1, Mengqi Jia2,3, Li Wang4 and Yanfang Sun2,3*
Zou et al. World Journal of Surgical Oncology (2018) 16:201 https://doi.org/10.1186/s12957-018-1503-6 CASEREPORT Open Access Glomus tumor in the floor of the mouth: a case report and review of the literature Haixiao Zou1,2, Li Song1, Mengqi Jia2,3, Li Wang4 and Yanfang Sun2,3* Abstract Background: Glomus tumors are rare benign neoplasms that usually occur in the upper and lower extremities. Oral cavity involvement is exceptionally rare, with only a few cases reported to date. Case presentation: A 24-year-old woman with complaints of swelling in the left floor of her mouth for 6 months was referred to our institution. Her swallowing function was slightly affected; however, she did not have pain or tongue paralysis. Enhanced computed tomography revealed a 2.8 × 1.8 × 2.1 cm-sized well-defined, solid, heterogeneous nodule above the mylohyoid muscle. The mandible appeared to be uninvolved. The patient underwent surgery via an intraoral approach; histopathological examination revealed a glomus tumor. The patient has had no evidence of recurrence over 4 years of follow-up. Conclusions: Glomus tumors should be considered when patients present with painless nodules in the floor of the mouth. Keywords: Glomus tumor, Floor of mouth, Oral surgery Background Case presentation Theglomusbodyisaspecialarteriovenousanasto- A 24-year-old woman with a 6-month history of swelling mosisandfunctionsinthermalregulation.Glomustu- in the left floor of her mouth was referred to our institu- mors are rare, benign, mesenchymal tumors that tion. Although she experienced slight difficulty in swal- originate from modified smooth muscle cells of the lowing, she did not experience pain or tongue paralysis. -

Benign Hemangiomas
TUMORS OF BLOOD VESSELS CHARLES F. GESCHICKTER, M.D. (From tke Surgical Palkological Laboratory, Department of Surgery, Johns Hopkins Hospital and University) AND LOUISA E. KEASBEY, M.D. (Lancaster Gcaeral Hospital, Lancuster, Pennsylvania) Tumors of the blood vessels are perhaps as common as any form of neoplasm occurring in the human body. The greatest number of these lesions are benign angiomas of the body surfaces, small elevated red areas which remain without symptoms throughout life and are not subjected to treatment. Larger tumors of this type which undergb active growth after birth or which are situated about the face or oral cavity, where they constitute cosmetic defects, are more often the object of surgical removal. The majority of the vascular tumors clinically or pathologically studied fall into this latter group. Benign angiomas of similar pathologic nature occur in all of the internal viscera but are most common in the liver, where they are disclosed usually at autopsy. Angiomas of the bone, muscle, and the central nervous system are of less common occurrence, but, because of the symptoms produced, a higher percentage are available for study. Malignant lesions of the blood vessels are far more rare than was formerly supposed. An occasional angioma may metastasize following trauma or after repeated recurrences, but less than 1per cent of benign angiomas subjected to treatment fall into this group. I Primarily ma- lignant tumors of the vascular system-angiosarcomas-are equally rare. The pathological criteria for these growths have never been ade- quately established, and there is no general agreement as to this par- ticular form of tumor. -

Angiosarcomas and Other Sarcomas of Endothelial Origin
Angiosarcomas and Other Sarcomas of Endothelial Origin a,b a Angela Cioffi, MD , Sonia Reichert, MD , c a,b,d, Cristina R. Antonescu, MD , Robert G. Maki, MD, PhD, FACP * KEYWORDS Angiosarcoma Epithelioid hemangioendothelioma Vascular sarcoma Kaposi sarcoma VEGF KDR FLT4 Translocation Organ transplant KEY POINTS Vascular sarcomas are rare and collectively affect fewer than 600 people a year in the United States (incidence approximately 2/million). Because angiosarcomas, hemangioendotheliomas, and other vascular tumors have unique embryonal derivation, it is not surprising that they have a unique sensitivity pattern to chemotherapy agents. Surgery, when possible, remains the primary treatment for angiosarcomas. Adjuvant radiation for primary disease seems prudent for at least some angiosarcoma, given the high local-regional recurrence rate of these tumors. Angiosarcomas also have a high rate of metastasis, but it is not clear that adjuvant chemotherapy improves survival. Epithelioid hemangioendothelioma is a unique form of sarcoma often presenting as multi- focal disease. Most patients can do well with observation alone, although a fraction of pa- tients have more aggressive disease and have difficulties in both local control and metastatic disease. Continued Disclosures: R.G. Maki receives clinical research support from Morphotek/Eisai, Ziopharm, and Imclone/Lilly. He has also consulted for Eisai, Morphotek/Eisai, Imclone/Lilly, Taiho, Glaxo- SmithKline, Merck, Champions Biotechnology, and Pfizer. He has received speaker’s fees from Novartis. He is an unpaid consultant for the Sarcoma Foundation of America, SARC: Sarcoma Alliance for Research through Collaboration, n-of-one, and 23 & me. C.R. Antonescu, A. Cioffi, and S. Reichert report no conflicts. -

View Open Access Histological Variants of Cutaneous Kaposi Sarcoma Wayne Grayson1 and Liron Pantanowitz*2
Diagnostic Pathology BioMed Central Review Open Access Histological variants of cutaneous Kaposi sarcoma Wayne Grayson1 and Liron Pantanowitz*2 Address: 1Histopathology Department, Ampath National Laboratory Support Services, Johannesburg, South Africa and 2Department of Pathology, Baystate Medical Center, Tufts University School of Medicine, Springfield, Massachusetts, USA Email: Wayne Grayson - [email protected]; Liron Pantanowitz* - [email protected] * Corresponding author Published: 25 July 2008 Received: 23 July 2008 Accepted: 25 July 2008 Diagnostic Pathology 2008, 3:31 doi:10.1186/1746-1596-3-31 This article is available from: http://www.diagnosticpathology.org/content/3/1/31 © 2008 Grayson and Pantanowitz; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract This review provides a comprehensive overview of the broad clinicopathologic spectrum of cutaneous Kaposi sarcoma (KS) lesions. Variants discussed include: usual KS lesions associated with disease progression (i.e. patch, plaque and nodular stage); morphologic subtypes alluded to in the older literature such as anaplastic and telangiectatic KS, as well as several lymphedematous variants; and numerous recently described variants including hyperkeratotic, keloidal, micronodular, pyogenic granuloma-like, ecchymotic, and intravascular KS. Involuting lesions as a result of treatment related regression are also presented. Introduction progression, (2) KS variants alluded to in the older litera- Kaposi sarcoma (KS) is a vascular lesion of low-grade ture, (3) more recently described KS variants, and (4) KS malignant potential that presents most frequently with lesions as a consequence of therapy. -

Multinucleate Cell Angiohistiocytoma
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book. s0060 MULTINUCLEATE CELL ANGIOHISTIOCYTOMA s0065 Definition • Fibroblast-like and histiocyte-like mononuclear cells u0390 p0300 • A distinctive benign dermal proliferation composed • Thickened collagen bundles, frequently hyalinized u0395 of thin-walled capillaries and veins, admixed with • Occasional inflammatory cells, predominantly u0400 scattered multinucleated cells lymphocytes • Hemorrhage absent, no hemosiderin deposition u0405 s0070 Clinical features • Decreased elastic fibers in the dermis can be observed u0410 s0075 Epidemiology • Overlying epidermis normal, but can also be u0415 p0310 • Female predominance (F:M = 3 : 1) hyperplastic u0275 • Middle-aged adult patients • Proliferation restricted to upper and middermis u0420 s0080 Presentation Immunopathology/special stains s0100 p0325 • Slowly growing single or multiple firm, red-brown to • Multinucleated cells display variable CD68 positivity -

Requires Subscription
DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com An unusual lesion on the nose: microvenular hemangioma A. Tulin Mansur1, Gulsen Tukenmez Demirci2, Eltaf A. Ozbal Koc3, Semsi Yildiz4 1 Dermatology Department, Istanbul Hospital, Baskent University, Istanbul, Turkey 2 Dermatology Department, Acibadem Altunizade Hospital, Acibadem University, Istanbul, Turkey 3 Ear, Nose and Throat Diseases Department, Istanbul Hospital, Baskent University, Istanbul, Turkey 4 Pathology Department, Istanbul Hospital, Baskent University, Istanbul, Turkey Key words: vascular anomaly, hemangioma Citation: Mansur AT, Tukenmez Demirci G, Ozbal Koc EA, Yildiz S. An unusual lesion on the nose: microvenular hemangioma. Dermatol Pract Concept. 2018;8(1):7-11. DOI: https://doi.org/10.5826/dpc.0801a02 Received: April 25, 2017; Accepted: October 6, 2017; Published: January 31, 2018 Copyright: ©2018 Mansur et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Funding: None. Competing interests: The authors have no conflicts of interest to disclose. All authors have contributed significantly to this publication. Corresponding author: Gulsen Tukenmez Demirci, Associate Professor, Dermatology Department, Acibadem Altunizade Hospital, Üsküdar 34662, Istanbul,˙ Turkey. Email: [email protected] ABSTRACT Microvenular hemangioma (MVH) is an acquired, benign type of hemangioma that usually manifests itself as a solitary, slowly growing, red to violaceous, asymptomatic papule, plaque or nodule. It is typically located on the trunk or extremities of young adults. It can be difficult to differentiate MVH from other types of hemangioma and Kaposi sarcoma. Herein we report a case of MVH unusual for its location, age of onset, and morphologic features. -

Malignant Vascular Tumors&Mdash
Modern Pathology (2014) 27, S30–S38 S30 & 2014 USCAP, Inc All rights reserved 0893-3952/14 $32.00 Malignant vascular tumors—an update Cristina Antonescu Department of Pathology, Memorial Sloan-Kettering Cancer Center, New York, NY, USA Although benign hemangiomas are among the most common diagnoses amid connective tissue tumors, sarcomas showing endothelial differentiation (ie, angiosarcoma and epithelioid hemangioendothelioma) represent under 1% of all sarcoma diagnoses, and thus it is likely that fewer than 500 people in the United States are affected each year. Differential diagnosis of malignant vascular tumors can be often quite challenging, either at the low end of the spectrum, distinguishing an epithelioid hemangioendothelioma from an epithelioid hemangioma, or at the high-grade end of the spectrum, between an angiosarcoma and a malignant epithelioid hemangioendothelioma. Within this differential diagnosis both clinico-radiological features (ie, size and multifocality) and immunohistochemical markers (ie, expression of endothelial markers) are often similar and cannot distinguish between benign and malignant vascular lesions. Molecular ancillary tests have long been needed for a more objective diagnosis and classification of malignant vascular tumors, particularly within the epithelioid phenotype. As significant advances have been recently made in understanding the genetic signatures of vascular tumors, this review will take the opportunity to provide a detailed update on these findings. Specifically, this article will focus on -
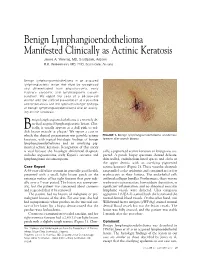
Benign Lymphangioendothelioma Manifested Clinically As Actinic Keratosis James A
Benign Lymphangioendothelioma Manifested Clinically as Actinic Keratosis James A. Yiannias, MD, Scottsdale, Arizona R.K. Winkelmann, MD, PhD, Scottsdale, Arizona Benign lymphangioendothelioma is an acquired lymphangiectatic lesion that must be recognized and differentiated from angiosarcoma, early Kaposi’s sarcoma, and lymphangioma circum- scriptum. We report the case of a 68-year-old woman with the clinical presentation of a possible actinic keratosis and the typical histologic findings of benign lymphangioendothelioma and an overly- ing actinic keratosis. enign lymphangioendothelioma is a recently de- scribed acquired lymphangiectatic lesion. Clin- ically, it usually appears as a dull pink to red- B 1 dish brown macule or plaque. We report a case in which the clinical presentation was possible actinic FIGURE 1. Benign lymphangioendothelioma at extensor keratosis, with typical histologic findings of benign forearm after punch biopsy. lymphangioendothelioma and an overlying pig- mented actinic keratosis. Recognition of this entity is vital because the histologic differential diagnosis cally, a pigmented actinic keratosis or lentigo was sus- includes angiosarcoma, early Kaposi’s sarcoma, and pected. A punch biopsy specimen showed delicate, lymphangioma circumscriptum. thin-walled, endothelium-lined spaces and clefts in the upper dermis, with an overlying pigmented Case Report actinic keratosis (Figure 2). These vascular channels A 68-year-old white woman in generally good health ran parallel to the epidermis and contained no or few presented with a small, light brown patch on the erythrocytes in their lumina. The endothelial cells extensor surface of her right forearm that grew radi- outlined collagen bundles. Furthermore, there was no ally over a 2-year period. The lesion was asymptom- erythrocyte extravasation, hemosiderin deposition, or atic, but the patient was concerned about cosmesis significant inflammation, and no abnormal muscular and requested that it be removed. -

Hepatic Angiosarcoma Masquerading As Hemangioma
Hepatic Angiosarcoma Masquerading as Hemangioma: A CASO CLÍNICO Challenging Differential Diagnosis Angiosarcoma Hepático e Hemangioma: Um Diagnóstico Diferencial Desafiante Ana Rita GARCIA1, João RIBEIRO1, Helena GERVÁSIO1, Francisco Castro e SOUSA2,3 Acta Med Port 2017 Oct;30(10):750-753 ▪ https://doi.org/10.20344/amp.8593 ABSTRACT Hemangiomas are usually diagnosed based on ultrasound findings. The presence of symptoms, rapid growth or atipical imagiological findings should make us consider other diagnoses, including malignant tumors such as angiosarcomas. We describe the case of a previously healthy 46-year-old female without a history of exposure to carcinogens who presented with abdominal pain for two months. Diagnostic work-up revealed elevated gamma-glutamyl transferase and lactate dehydrogenase levels. Abdominal ultrasound described a large nodular lesion in the right lobe of the liver described as a hemangioma. One month later, a computed tomography-scan was made and revealed the same lesion, which had grown from 13.5 to 20 cm, maintaining typical imaging characteristics of a hemangioma. A right hepatectomy was performed and pathology revealed an angiosarcoma. After surgery, a positron emission tomography-com- puted tomography scan showed hepatic and bone metastasis. The patient started taxane-based chemotherapy and lumbar palliative radiotherapy, but died 10 months after surgery. This case shows how difficult it is to diagnose hepatic angiosarcoma relying only on imaging findings. Two abdominal computed tomography -scans were performed and none suggested this diagnosis. Angiosarcoma is a very aggressive tumour with an adverse prognosis. Surgery is the only curative treatment available. However, it is rarely feasible due to unresectable disease or distant metastasis. -

8 Liver Hemangioma
Liver Hemangioma 101 8 Liver Hemangioma Valérie Vilgrain and Giuseppe Brancatelli CONTENTS 8.1 Introduction 8.1 Introduction 101 8.2 Sonography 101 8.3 Computed Tomography 102 Hemangioma is the most common benign hepatic 8.4 Magnetic Resonance 104 tumor. The prevalence of hemangioma in the general 8.5 Scintigraphy 107 population ranges from 1%–2% to 20% (Semelka and 8.6 Percutaneous Biopsy 107 Sofka 1997). The female-to-male ratio varies from 8.7 Atypical Patterns 108 2:1 to 5:1. They occur at all ages. The vast majority of 8.7.1 Hemangioma with Echoic Border 108 8.7.2 Large, Heterogeneous Hemangioma 108 hemangiomas remain clinically silent. Few patients 8.7.3 Rapidly Filling Hemangioma 108 are symptomatic due to a mass lesion, complications 8.7.4 Very Slow Filling Hemangioma 110 or compression of adjacent structures. Most of these 8.7.5 Calcifi ed Hemangioma 110 symptoms are observed in large hemangiomas. The 8.7.6 Hyalinized Hemangioma 110 natural history of hemangiomas is variable: most of 8.7.7 Cystic or Multilocular Hemangioma 111 8.7.8 Hemangioma with Fluid–Fluid Level 111 them remain stable, some may grow or involute. The 8.7.9 Pedunculated Hemangioma 111 role of sex hormones in causing enlargement during 8.7.10 Hemangioma with pregnancy or recurrence is disputed. Arterial-Portal Venous Shunt 111 Hemangiomas are usually solitary, less than 5 cm 8.7.11 Hemangioma with Capsular Retraction 111 in size and appear as well-delineated lesions of red 8.8 Hemangioma Developing in Abnormal Liver 112 color that partially collapse on sectioning. -

Hepatic Angiosarcoma: Mimicking of Angioma on Three-Phase Technetium-99M Red Blood Cell Scintigraphy
Hepatic Angiosarcoma: Mimicking of Angioma on Three-Phase Technetium-99m Red Blood Cell Scintigraphy Ferris Ginsberg, James D. Slavin, Jr., and Richard P. Spencer Department of Radiology, Saint Francis Hospital and Medical Center, Hartford; and Department of Nuclear Medicine, University of Connecticut Health Center, Farmington, Connecticut A [99mTc]RBC study in a 63-yr-old man showed intrahepatic lesions which initially had less activity than surrounding liver tissue. When viewed 3 hr later, these had "reversed" and the lesions revealed increased uptake of the radiolabeled red cells. Some extrahepatic areas showed the same pattern (these were in the mesentery of the small bowel). The lesions proved to be angiosarcomas. Hence, the behavior of labeled red cells in these angiosarcomas mimicked that in benign hemangiomas. J NucÃMed 27:1861-1863,1986 . he three-phase technetium-99m red cell ([WmTc] ~ 1,500 rad external radiation to the region. During a chole- RBC) imaging technique has been reported as highly cystectomy performed 10 yr prior to the current admission, specific for identifying benign intrahepatic heman careful exploration of the abdomen revealed only thickening giomas; the imaging pattern has not been described in of the left retroperitoneum. There was no evidence of tumor any other lesion (1-3). We describe a case with an at that time and the liver was noted to be normal. imaging study identical to that of intrahepatic heman An exploratory laparotomy was performed 3 wk after ad mission; it revealed multiple intrahepatic masses as well as giomas, but which was due to a malignant tumor. multiple smaller nodular lesions involving most of the small bowel mesentery.