Angiosarcomas and Other Sarcomas of Endothelial Origin
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hemangiosarcoma Philip J
Ettinger & Feldman – Textbook of Veterinary Internal Medicine Client Information Sheet Hemangiosarcoma Philip J. Bergman What is hemangiosarcoma? Hemangiosarcoma (HSA; angiosarcoma or malignant hemangioendothelioma) is an extremely aggressive tumor of blood vessel origin. Because blood vessels are present throughout the body, virtually any site in the body can have HSA. HSA occurs most frequently in dogs (approximately 2% of all tumors) and the most common site is the spleen. However, additional common sites include the heart, liver, muscle, lung skin, bones, kidney, brain, abdomen, and oral cavity. In three large canine splenic disease studies encompassing approximately 2000 dogs, a “rule of two thirds” was found suggesting that approximately two thirds of dogs with a splenic mass have a cancer (therefore one third are not malignant) and two thirds of the malignant tumors of the spleen are HSA. HSA is a disease generally of older dogs and cats with an average onset of 9 to 10 years; however, there are reports of extremely young dogs and cats with this disease (5 to 6 months to a few years of age). German shepherd dogs are most commonly diagnosed with HSA; however, other large breed dogs such as golden retrievers and Labrador retrievers may also be overrepresented. In cats, the most common breed is the domestic shorthair. The cause of HSA in dogs and cats is presently unknown. Exposures to toxins such as chemicals, insecticides, and radiation have been reported in humans to be associated with HSA. Ultraviolet light exposure from the sun may be a potential cause of HSA in dogs, as HSAs of the skin are commonly seen in dogs with light hair and poor pigmentation (e.g., Salukis, Whippets, and white Bulldogs). -

Glomus Tumor in the Floor of the Mouth: a Case Report and Review of the Literature Haixiao Zou1,2, Li Song1, Mengqi Jia2,3, Li Wang4 and Yanfang Sun2,3*
Zou et al. World Journal of Surgical Oncology (2018) 16:201 https://doi.org/10.1186/s12957-018-1503-6 CASEREPORT Open Access Glomus tumor in the floor of the mouth: a case report and review of the literature Haixiao Zou1,2, Li Song1, Mengqi Jia2,3, Li Wang4 and Yanfang Sun2,3* Abstract Background: Glomus tumors are rare benign neoplasms that usually occur in the upper and lower extremities. Oral cavity involvement is exceptionally rare, with only a few cases reported to date. Case presentation: A 24-year-old woman with complaints of swelling in the left floor of her mouth for 6 months was referred to our institution. Her swallowing function was slightly affected; however, she did not have pain or tongue paralysis. Enhanced computed tomography revealed a 2.8 × 1.8 × 2.1 cm-sized well-defined, solid, heterogeneous nodule above the mylohyoid muscle. The mandible appeared to be uninvolved. The patient underwent surgery via an intraoral approach; histopathological examination revealed a glomus tumor. The patient has had no evidence of recurrence over 4 years of follow-up. Conclusions: Glomus tumors should be considered when patients present with painless nodules in the floor of the mouth. Keywords: Glomus tumor, Floor of mouth, Oral surgery Background Case presentation Theglomusbodyisaspecialarteriovenousanasto- A 24-year-old woman with a 6-month history of swelling mosisandfunctionsinthermalregulation.Glomustu- in the left floor of her mouth was referred to our institu- mors are rare, benign, mesenchymal tumors that tion. Although she experienced slight difficulty in swal- originate from modified smooth muscle cells of the lowing, she did not experience pain or tongue paralysis. -

Infantile Hemangioendothelioma of the Parotid Gland
Elmer ress Case Report Int J Clin Pediatr. 2015;4(4):184-185 Infantile Hemangioendothelioma of the Parotid Gland Veeranna A. Kotrashettia, Vijay Baburao Sonawanea, b, Kapil Bainadea, Reshu Agarwala Abstract parotid region, 4 × 3 cm in size, smooth in surface, no pulsa- tions with no signs of inflammation (Fig. 1). Tumors of salivary glands are uncommon in children (less than 5%). Complete blood count was normal. USG revealed en- Hemangioma is the commonest tumor of salivary gland tumors (more larged parotid gland measuring 3.1 × 2.2 × 2.5 cm with in- than 50%). We report a rare case of infantile hemangioma (IH) of creased vascularity. parotid gland. MRI showed well-defined, lobulated homogenously en- hancing leison diffusely involving the superficial and deep Keywords: Hemangioma; Hemangioendothelioma; Parotid gland layers of parotid gland (Fig. 2). Findings are suggestive of in- fantile hemangioendothelioma. Introduction Discussion Infantile hemangiomas (IHs) are the most common tumor of IH of parotid gland is the most common tumor. Weiss and oth- infancy and have a well-described natural history of rapid growth during early infancy followed by gradual involution [1, 2]. Congenital capillary hemangioma is classified as true hemangioma of infancy [3]. It is usually not noticed in new- born period but becomes prominent in first months of life. Most common age of presentation is about 4 months. Parotid hemangioma demonstrates rapid growth in first months of life but usually regresses after 18 months [4]. MRI is the best im- aging technique to demonstrate parotid hemangioma. MRI shows hyperintense parotid gland hemangioma con- taining vascular flow voids. -

View Open Access Histological Variants of Cutaneous Kaposi Sarcoma Wayne Grayson1 and Liron Pantanowitz*2
Diagnostic Pathology BioMed Central Review Open Access Histological variants of cutaneous Kaposi sarcoma Wayne Grayson1 and Liron Pantanowitz*2 Address: 1Histopathology Department, Ampath National Laboratory Support Services, Johannesburg, South Africa and 2Department of Pathology, Baystate Medical Center, Tufts University School of Medicine, Springfield, Massachusetts, USA Email: Wayne Grayson - [email protected]; Liron Pantanowitz* - [email protected] * Corresponding author Published: 25 July 2008 Received: 23 July 2008 Accepted: 25 July 2008 Diagnostic Pathology 2008, 3:31 doi:10.1186/1746-1596-3-31 This article is available from: http://www.diagnosticpathology.org/content/3/1/31 © 2008 Grayson and Pantanowitz; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract This review provides a comprehensive overview of the broad clinicopathologic spectrum of cutaneous Kaposi sarcoma (KS) lesions. Variants discussed include: usual KS lesions associated with disease progression (i.e. patch, plaque and nodular stage); morphologic subtypes alluded to in the older literature such as anaplastic and telangiectatic KS, as well as several lymphedematous variants; and numerous recently described variants including hyperkeratotic, keloidal, micronodular, pyogenic granuloma-like, ecchymotic, and intravascular KS. Involuting lesions as a result of treatment related regression are also presented. Introduction progression, (2) KS variants alluded to in the older litera- Kaposi sarcoma (KS) is a vascular lesion of low-grade ture, (3) more recently described KS variants, and (4) KS malignant potential that presents most frequently with lesions as a consequence of therapy. -

Vascular Malformations, Skeletal Deformities Including Macrodactyly, Embryonic Veins
1.) Give a general classification and nomenclature to think about when evaluating these patients 2.) Share some helpful tips to narrow the differential in a minute or less of interaction 3.) Discuss some helpful imaging recommendations focusing on ultrasound Vascular Anomalies Tumors: Malformations: Hemangiomas: Low flow: Infantile Hemangioma (IH) Capillary malformation (CM) Rapidly involuting congenital hemangioma (RICH) Non-involuting congenital hemangioma (NICH) Venous malformation (VM) Kaposiform Hemangioendothelioma Lymphatic malformation (LM) (KHE) High flow: Arteriovenous malformation (AVM) Tufted Angioma (TA) Combined including syndromic VA. Other rare tumors www.issva.org • 2014 ISSVA classification is now 20 pages long • The key is that the imaging characteristics have not changed • Rapidly growing field • Traditionally, options were always the same – Surgery – Do nothing • With the increase in awareness and research as well as the development of the specialty of vascular anomalies: New Treatment Options Available – Treatment directly linked to diagnosis • Today, we have: – Interventional catheter based therapies – Laser surgery – Ablation technologies: Cryo, RFA, Microwave, etc. – Direct image-guided medications to administer – Infusion medicines – Oral medicines – Surgery- although much less common – Do Nothing- a VERY important alternative • Survey sample of 100 Referred patients – 47% wrong Dx – 35% wrong Tx • 14% wrong Tx with correct Dx • VAC – 14% indeterminate or wrong Dx – only 4% leave with no Tx plan • Important because -

A Case of Lymphangioleiomyomatosis Originated in the Pelvic Cavity
J Gynecol Oncol Vol. 19, No. 3:195-198, September 2008 DOI:10.3802/jgo.2008.19.3.195 Case Report A case of lymphangioleiomyomatosis originated in the pelvic cavity Jung-Mi Han, Kyung-Hee Lee, Sung-Joo Kim, Chae-Chun Rhim, Young-Han Park, Jung-Bae Kang, Sun-Young Jeon1 Departments of Obstetrics and Gynecology, 1Pathology, Hallym University Medical College, Anyang, Korea Lymphangioleiomyomatosis is a rare disease that is characterized by proliferation of abnormal smooth muscle-like cells, especially that which occurs in the pulmonary parenchyme. It primarily affects women of child-bearing age. The majority of primary lymphangioleiomyomatosis occurs in the lung, but there are a few reports of extrapulmonary cases. We experienced a rare case of lymphangioleiomyomatosis which originated in the pelvic cavity (in the posterior portion of the uterus), and report with brief review of literatures. Key Words: Lymphangioleiomyomatosis, Pelvis, Uterus INTRODUCTION hypervascular tumor between the uterus and the right ovary, and two small myomas about 2 cm in size (Fig. 1). Under the Lymphangioleiomyomatosis is a very rare disease which impression of ovarian malignancy she had admitted for shows typical features of abnormal smooth muscle cell further evaluation including MRI. Her initial serum CA-125 proliferation and which develops in females during the level was 26.7 U/ml and CA 19-9 level was below 2 U/ml, and reproductive period.1,2 The majority cases of this disease other hematologic findings were all within the normal range. primarily occur in the lungs, but extrapulmonary regions such Magnetic resonance imaging study of the abdomen-pelvis as the pelvis and retroperitoneal spaces are occasionally demonstrated an approximately 4.0×5.0×4.0 cm sized tumor primary sites. -

Kaposiform Hemangioendothelioma in Tonsil of a Child
Rekhi et al. World Journal of Surgical Oncology 2011, 9:57 http://www.wjso.com/content/9/1/57 WORLD JOURNAL OF SURGICAL ONCOLOGY CASEREPORT Open Access Kaposiform hemangioendothelioma in tonsil of a child associated with cervical lymphangioma: a rare case report Bharat Rekhi1*, Shweta Sethi1, Suyash S Kulkarni2 and Nirmala A Jambhekar1 Abstract Kaposiform hemangioendothelioma (KHE) is an uncommon vascular tumor of intermediate malignant potential, usually occurs in the extremities and retroperitoneum of infants and is characterized by its association with lymphangiomatosis and Kasabach-Merritt phenomenenon (KMP) in certain cases. It has rarely been observed in the head and neck region and at times, can present without KMP. Herein, we present an extremely uncommon case of KHE occurring in tonsil of a child, associated with a neck swelling, but unassociated with KMP. A 2-year-old male child referred to us with history of sore throat, dyspnoea and right-sided neck swelling off and on, since birth, was clinicoradiologically diagnosed with recurrent tonsillitis, including right sided peritonsillar abscess, for which he underwent right-sided tonsillectomy, elsewhere. Histopathological sections from the excised tonsillar mass were reviewed and showed a tumor composed of irregular, infiltrating lobules of spindle cells arranged in kaposiform architecture with slit-like, crescentic vessels. The cells displayed focal lumen formation containing red blood cells (RBCs), along with platelet thrombi and eosinophilic hyaline bodies. In addition, there were discrete foci of several dilated lymphatic vessels containing lymph and lymphocytes. On immunohistochemistry (IHC), spindle cells were diffusely positive for CD34, focally for CD31 and smooth muscle actin (SMA), the latter marker was mostly expressed around the blood vessels. -

Angiokeratoma.Pdf
Classification of vascular tumors/nevi Vascular tumors mainly of infancy and childhood • Hemangioma of infancy. • Congenital hemangioma. • Miliary hemangiomatosis of infancy. • Spindle cell hemangioma. • Kaposiform hemangioendothelioma. • Tufted angioma. • Sinusoidal hemagioma. Vascular malformation - Capillary: • Salmon patch. • Potr-wine stain. • Nevus anemicus. - Mixed vascular malformation: • Reticulate vascular nevus. • Klipple ternaunay syndrome. • Venous malformation. • Blue rubber bleb nevus syndrome. • Maffucci syndrome. • Zosteriform venous malformation. • Other multiple vascular malformation syndrome. - Lymphatic malformations: • Microcystic/Macrocystic. • Rapid flow (arteriovenous malformation). Angiokeratoma: • Angiokeratoma circumscriptum naeviforme. • Angiokeratoma of Mibelli (or angiokeratoma acroasphyticum digitorum) . • Solitary papular angiokeratoma. • Angiokeratoma of fordyce (or angiokeratoma scroti). • Angiokeratoma corporis diffusum. Cutanous vascular hyperplasia: • Lobular capillary hemangioma. • Epithelioid hemangioma. • Crisoid aneurysm. • Reactive angioendotheliomatosis. • Gromeruloid hemangioma. • Hobnail hemangioma. • Microvascular hemangioma. Benign neoplasm: • Glomus tumors. Malignancy: • Kaposi sarcoma. • Angiosarcoma. • Retiform hemangioendothelioma. Modified classification of the International Society for the Study of Vascular Anomalies (Rome, Italy, 1996) : Tumors: -Hemangiomas: • Superficial (capillary or strawberry haemangioma). • Deep (cavernous haemangioma). • Combined. - Others: • Kaposiform -

Malignant Vascular Tumors&Mdash
Modern Pathology (2014) 27, S30–S38 S30 & 2014 USCAP, Inc All rights reserved 0893-3952/14 $32.00 Malignant vascular tumors—an update Cristina Antonescu Department of Pathology, Memorial Sloan-Kettering Cancer Center, New York, NY, USA Although benign hemangiomas are among the most common diagnoses amid connective tissue tumors, sarcomas showing endothelial differentiation (ie, angiosarcoma and epithelioid hemangioendothelioma) represent under 1% of all sarcoma diagnoses, and thus it is likely that fewer than 500 people in the United States are affected each year. Differential diagnosis of malignant vascular tumors can be often quite challenging, either at the low end of the spectrum, distinguishing an epithelioid hemangioendothelioma from an epithelioid hemangioma, or at the high-grade end of the spectrum, between an angiosarcoma and a malignant epithelioid hemangioendothelioma. Within this differential diagnosis both clinico-radiological features (ie, size and multifocality) and immunohistochemical markers (ie, expression of endothelial markers) are often similar and cannot distinguish between benign and malignant vascular lesions. Molecular ancillary tests have long been needed for a more objective diagnosis and classification of malignant vascular tumors, particularly within the epithelioid phenotype. As significant advances have been recently made in understanding the genetic signatures of vascular tumors, this review will take the opportunity to provide a detailed update on these findings. Specifically, this article will focus on -
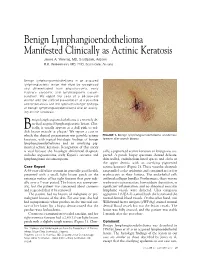
Benign Lymphangioendothelioma Manifested Clinically As Actinic Keratosis James A
Benign Lymphangioendothelioma Manifested Clinically as Actinic Keratosis James A. Yiannias, MD, Scottsdale, Arizona R.K. Winkelmann, MD, PhD, Scottsdale, Arizona Benign lymphangioendothelioma is an acquired lymphangiectatic lesion that must be recognized and differentiated from angiosarcoma, early Kaposi’s sarcoma, and lymphangioma circum- scriptum. We report the case of a 68-year-old woman with the clinical presentation of a possible actinic keratosis and the typical histologic findings of benign lymphangioendothelioma and an overly- ing actinic keratosis. enign lymphangioendothelioma is a recently de- scribed acquired lymphangiectatic lesion. Clin- ically, it usually appears as a dull pink to red- B 1 dish brown macule or plaque. We report a case in which the clinical presentation was possible actinic FIGURE 1. Benign lymphangioendothelioma at extensor keratosis, with typical histologic findings of benign forearm after punch biopsy. lymphangioendothelioma and an overlying pig- mented actinic keratosis. Recognition of this entity is vital because the histologic differential diagnosis cally, a pigmented actinic keratosis or lentigo was sus- includes angiosarcoma, early Kaposi’s sarcoma, and pected. A punch biopsy specimen showed delicate, lymphangioma circumscriptum. thin-walled, endothelium-lined spaces and clefts in the upper dermis, with an overlying pigmented Case Report actinic keratosis (Figure 2). These vascular channels A 68-year-old white woman in generally good health ran parallel to the epidermis and contained no or few presented with a small, light brown patch on the erythrocytes in their lumina. The endothelial cells extensor surface of her right forearm that grew radi- outlined collagen bundles. Furthermore, there was no ally over a 2-year period. The lesion was asymptom- erythrocyte extravasation, hemosiderin deposition, or atic, but the patient was concerned about cosmesis significant inflammation, and no abnormal muscular and requested that it be removed. -

Hepatic Angiosarcoma Masquerading As Hemangioma
Hepatic Angiosarcoma Masquerading as Hemangioma: A CASO CLÍNICO Challenging Differential Diagnosis Angiosarcoma Hepático e Hemangioma: Um Diagnóstico Diferencial Desafiante Ana Rita GARCIA1, João RIBEIRO1, Helena GERVÁSIO1, Francisco Castro e SOUSA2,3 Acta Med Port 2017 Oct;30(10):750-753 ▪ https://doi.org/10.20344/amp.8593 ABSTRACT Hemangiomas are usually diagnosed based on ultrasound findings. The presence of symptoms, rapid growth or atipical imagiological findings should make us consider other diagnoses, including malignant tumors such as angiosarcomas. We describe the case of a previously healthy 46-year-old female without a history of exposure to carcinogens who presented with abdominal pain for two months. Diagnostic work-up revealed elevated gamma-glutamyl transferase and lactate dehydrogenase levels. Abdominal ultrasound described a large nodular lesion in the right lobe of the liver described as a hemangioma. One month later, a computed tomography-scan was made and revealed the same lesion, which had grown from 13.5 to 20 cm, maintaining typical imaging characteristics of a hemangioma. A right hepatectomy was performed and pathology revealed an angiosarcoma. After surgery, a positron emission tomography-com- puted tomography scan showed hepatic and bone metastasis. The patient started taxane-based chemotherapy and lumbar palliative radiotherapy, but died 10 months after surgery. This case shows how difficult it is to diagnose hepatic angiosarcoma relying only on imaging findings. Two abdominal computed tomography -scans were performed and none suggested this diagnosis. Angiosarcoma is a very aggressive tumour with an adverse prognosis. Surgery is the only curative treatment available. However, it is rarely feasible due to unresectable disease or distant metastasis. -

The Rare Case of Positive FDG-Positron Emission
Case Report iMedPub Journals British Journal of Research 2017 http://www.imedpub.com/ Vol.4 No.3:19 ISSN 2394-3718 DOI: 10.21767/2394-3718.100019 The Rare Case of Positive FDG-Positron Emission Tomography for Giant Cavernous Hemangioma of the Liver Sollaku S1, Frantellizzi V1,2*, Casciani E3, Gualdi G3, Liberatore M1, Monteleone F1 and De Vincentis G1 1Department of Radiological, Oncological and Anatomo-Pathological Sciences, University of Rome Sapienza, Rome, Italy 2PhD Programm: Angio-Cardio-Thoracic Pathophisiology and Imaging, Sapienza University of Rome, Rome, Italy 3Department of Emergency Medicine, Policlinico Umberto I, Sapienza University of Rome, Rome, Italy *Corresponding author: Dr Viviana Frantellizzi, Department of Radiological, Oncological and Anatomo-Pathological Sciences, University of Rome Sapienza,Rome, Italy, Tel: +39 06 49978590; Fax: +39 06 49978592; E-mail: [email protected] Received Date: June 24, 2017; Accepted Date: August 14, 2017; Published Date: August 16, 2017 Copyright: © 2017 Sollaku S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Citation: Sollaku S, Frantellizzi V, Casciani E, Gualdi G, Liberatore M, et al. The Rare Case of Positive FDG-Positron Emission Tomography for Giant Cavernous Hemangioma of the Liver. Br J Res 2017, 4(3): 19. Abstract Hemangioma is the most common benign liver tumor and the second most common liver tumor after metastases. Large hemangiomas are often heterogeneous. When they exceed 4 cm in diameter, they are termed giant hemangiomas.