Hearing Before the Committee on Government Reform
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Values, Justifications, and Perspectives Connected to the Anti-Vaccination Movement Gigi Garzio [email protected]
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Sound Ideas University of Puget Sound Sound Ideas Summer Research Summer 2018 Values, Justifications, and Perspectives Connected to the Anti-Vaccination Movement Gigi Garzio [email protected] Follow this and additional works at: https://soundideas.pugetsound.edu/summer_research Part of the Anthropology Commons, and the Medicine and Health Commons Recommended Citation Garzio, Gigi, "Values, Justifications, and Perspectives Connected to the Anti-Vaccination Movement" (2018). Summer Research. 309. https://soundideas.pugetsound.edu/summer_research/309 This Article is brought to you for free and open access by Sound Ideas. It has been accepted for inclusion in Summer Research by an authorized administrator of Sound Ideas. For more information, please contact [email protected]. Introduction Throughout the 18th and 19th centuries, when the first smallpox outbreak began and the first vaccine was introduced, there has been vaccine skepticism (Offit, 2015). Smallpox outbreaks, and the fatalities that come with it, continued to spread around the world despite the development of the vaccine. However, between the 1940s and the early 1970s, anti-vaccine sentiment declined due to “three trends: a boom in vaccine science, discovery, and manufacture; public awareness of widespread outbreaks of infectious diseases (measles, mumps, rubella, pertussis, polio, and others) and the desire to protect children from these highly prevalent ills; and a baby boom, accompanied by increasing levels of education and wealth” (Poland et al, 2011). These factors led to general public acceptance of vaccines, which resulted in significant decreases in disease outbreaks. However, with less visible outbreaks of disease and more vaccines being added to the childhood vaccination schedule, the presence of the anti-vaccination movement returned in the 1970s (Wolfe, 2002). -
Adverse Effects of Vaccines: Evidence and Causality
REPORT BRIEF AUGUST 2011 .For more information visit www.iom.edu/vaccineadverseeffects Adverse Effects of Vaccines Evidence and Causality Immunizations are a cornerstone of the nation’s efforts to protect people from a host of infectious diseases. As required by the Food and Drug Admin- istration, vaccines are tested for safety before they enter the market, and their performance is continually evaluated to identify any risks that might appear over time. Vaccines are not free from side effects, or “adverse effects,” but most are very rare or very mild. Importantly, some adverse health problems following a vaccine may be due to coincidence and are not caused by the vaccine. As part of the evaluation of vaccines over time, researchers assess evidence to deter- As part of the evaluation of mine if adverse events following vaccination are causally linked to a specific vaccines over time, researchers vaccine, and if so, they are referred to as adverse effects. Under the National assess evidence to determine if Childhood Vaccine Injury Act of 1986, Congress established the National Vac- adverse events following cine Injury Compensation Program (VICP) to provide compensation to peo- vaccination are causally linked to ple injured by vaccines. Anyone who thinks they or a family member—often a a specific vaccine, and if so, they are referred to as adverse effects. child—has been injured can file a claim. The Health Resources and Services Administration (HRSA), the agency within the Department of Health and Human Services that administers VICP, can use evidence that demonstrates a causal link between an adverse event and a vaccine to streamline the claim process. -

Vaccines and Autism: What You Should Know | Vaccine Education
Q A Vaccines and Autism: What you should know Volume& 1 Summer 2008 Some parents of children with autism are concerned that vaccines are the cause. Their concerns center on three areas: the combination measles-mumps-rubella (MMR) vaccine; thimerosal, a mercury-containing preservative previously contained in several vaccines; and the notion that babies receive too many vaccines too soon. Q. What are the symptoms of autism? Q. Does the MMR vaccine cause autism? A. Symptoms of autism, which typically appear during the A. No. In 1998, a British researcher named Andrew Wakefi eld fi rst few years of life, include diffi culties with behavior, social raised the notion that the MMR vaccine might cause autism. skills and communication. Specifi cally, children with autism In the medical journal The Lancet, he reported the stories of may have diffi culty interacting socially with parents, siblings eight children who developed autism and intestinal problems and other people; have diffi culty with transitions and need soon after receiving the MMR vaccine. To determine whether routine; engage in repetitive behaviors such as hand fl apping Wakefi eld’s suspicion was correct, researchers performed or rocking; display a preoccupation with activities or toys; a series of studies comparing hundreds of thousands of and suffer a heightened sensitivity to noise and sounds. children who had received the MMR vaccine with hundreds Autism spectrum disorders vary in the type and severity of of thousands who had never received the vaccine. They found the symptoms they cause, so two children with autism may that the risk of autism was the same in both groups. -

Science Reporting Syllabus: Covering the Environment, Technology and Medicine
1 Science reporting syllabus: Covering the environment, technology and medicine Science reporting is in a moment of extreme transition: Popular science writing is experiencing a renaissance at precisely the moment that traditional media outlets are jettisoning specialized reporters. This creates tremendous opportunity and tremendous challenges. This course makes sure students are prepared to meet those challenges. Course objective This course is designed to acquaint reporters with all aspects of science reporting and writing. It will train participants to view new breakthroughs and discoveries with skepticism and will give students a working knowledge of many of the main areas of science coverage, including the environment, artificial intelligence, and human interaction with technology. There will be lessons on social media, online writing, news and feature writing, and writing long-form narratives. Learning objectives The syllabus is designed to strengthen students’ core competencies in several areas: Determining what sources and outlets can be trusted to discuss controversial or unproven claims. Learning which questions will elicit meaningful responses. Understanding that choosing not to cover a story can be just as important an editorial decision as deciding how to cover it. Evaluating what type of form a journalist is most comfortable with and seeking out ways to work in that form. Course design This course will focus on developing toolkits for evaluating science stories in addition to learning about some specific issues or controversies. It is designed as a workshop course for between 10 and 15 students. An integral part of the course is analyzing and critiquing other students’ work. Readings Required books Deborah Blum, Mary Knudson and Robin Marantz Henig, editors, A Field Guide for Science Writers, 2005. -

Royal College of Paediatrics and Child Health British Paediatric Surveillance Unit
Royal College of Paediatrics and Child Health British Paediatric Surveillance Unit 14th Annual Report 1999/2000 The British Paediatric Surveillance Unit always welcomes invitations to give talks describing the work of the Unit and makes every effort to respond to these positively. Enquiries should be directed to our office. The Unit positively encourages recipients to copy and circulate this report to colleagues, junior staff and medical students. Additional copies are available from our office, to which any enquiries should be addressed. Published September 2000 by the: British Paediatric Surveillance Unit A unit within the Research Division of the Royal College of Paediatrics and Child Health 50 Hallam Street London W1W 6DE Telephone: 44 (0) 20 7307 5680 Facsimile: 44 (0) 20 7307 5690 E-mail: [email protected] Registered Charity No. 1057744 ISBN 1 900954 48 6 © British Paediatric Surveillance Unit British Paediatric Surveillance Unit - 14 Annual Report 1999-2000 Compiled and edited by Richard Lynn, Angus Nicoll, Jugnoo Rahi and Chris Verity Membership of Executive Committee 1999/2000 Dr Christopher Verity Chairman Dr Angus Clarke Co-opted Professor Richard Cooke Royal College of Paediatrics and Child Health Research Division Dr Patricia Hamilton Co-opted Professor Peter Kearney Faculty of Paediatrics, Royal College of Physicians of Ireland Dr Jugnoo Rahi Medical Adviser Dr Ian Jones Scottish Centre for Infection and Environmental Health Dr Christopher Kelnar Co-opted Dr Gabrielle Laing Co-opted Mr Richard Lynn Scientific Co-ordinator -
NIH FOIA Log - FY 2017
NIH FOIA Log - FY 2017 Date Request Id Organization Name City State Records Requested Received 45612 LSU Health - Shreveport Shreveport Louisiana Copies of 3 NIDDK grants. 10/3/2016 Records relating to the use of the investigational drug Fostriecin in a human clinical trial sponsored by the NCI's Cancer Therapy Evaluation 45614 Individual Lakeway Texas Program. 10/3/2016 Site visit reports for UTMB (3/1/15- present); Battelle-Ohio (10/1/15- present); and Alpha Genesis-SC 45615 SAEN Milford Ohio (4/1/14-present). 10/3/2016 A copy of NCI grant 1R43CA135915- 45616 UCLA School of Engineering Los Angeles California 01. 10/4/2016 Washington University School of A copy of NIAID grant 45617 Medicine St. Louis Missouri K22AI052407. 10/4/2016 Washington University School of A copy of NHLBI grant 45618 Medicine St. Louis Missouri R01HL081398. 10/4/2016 Grant application and summary Washington University School of statement for NIDDK grant 45619 Medicine St. Louis Missouri K01DK077878. 10/4/2016 Data pertaining to all NIH purchases of the Victor model plate reader (model Victor 1, 2, 3 and Victor X) 45620 IMGEN Technologies Alexandria Virginia from Perkin Elmer from 1999-2012. 10/3/2016 Copy of NEI grant R21EY026438- 45621 Tufts Medical Center Brookline Massachusetts 01. 10/5/2016 A copy of all emails to and from two NIH employees from May 25, 2016 to June 25, 2016 regarding the NTP 45622 Individual Greenbelt Maryland radiofrequency study. 10/5/2016 Date Request Id Organization Name City State Records Requested Received Copies of the RCDC Thesaurus from 45623 Catenion Berlin Other 2010-2014. -

Addressing the Justifications for Vaccine Denial and Applying The
University of Northern Iowa UNI ScholarWorks Honors Program Theses Honors Program 2016 A healthy herd: addressing the justifications for accinev denial and applying the health belief model to the current anti- vaccination movement Sarah L. McHugh University of Northern Iowa Let us know how access to this document benefits ouy Copyright ©2016 Sarah L. McHugh Follow this and additional works at: https://scholarworks.uni.edu/hpt Part of the Infectious Disease Commons, and the Preventive Medicine Commons Recommended Citation McHugh, Sarah L., "A healthy herd: addressing the justifications for accinev denial and applying the health belief model to the current anti-vaccination movement" (2016). Honors Program Theses. 225. https://scholarworks.uni.edu/hpt/225 This Open Access Honors Program Thesis is brought to you for free and open access by the Honors Program at UNI ScholarWorks. It has been accepted for inclusion in Honors Program Theses by an authorized administrator of UNI ScholarWorks. For more information, please contact [email protected]. A HEALTHY HERD: ADDRESSING THE JUSTIFICATIONS FOR VACCINE DENIAL AND APPLYING THE HEALTH BELIEF MODEL TO THE CURRENT ANTI- VACCINATION MOVEMENT A Thesis Submitted in Partial Fulfillment of the Requirements for the Designation University Honors with Distinction Sarah L. McHugh University of Northern Iowa May 2016 This Study by: Sarah L. McHugh Entitled: A Healthy Herd: Addressing the Justifications for Vaccine Denial and Applying the Health Belief Model to the Current Anti-vaccination Movement has been approved as meeting the thesis or project requirement for the Designation University Honors with Distinction __________ ______________________________________________________ Date Dr. Thomas Davis, Honors Thesis Advisor, Division of Health Promotion and Education, School of Health, Physical Education and Leisure Services __________ ______________________________________________________ Date Dr. -
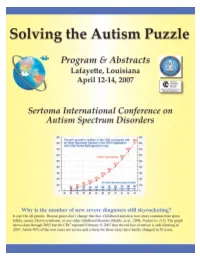
Solving the Autism Puzzle
Contents Foreword .............................. 4 Saturday (Schedule) .................... 18 Acknowledgments by Sertoma . 5 Poster Session 1: Friday 9:30 am . 20 Purpose of Autism07 .................... 6 Poster Session 2: Friday 3:00 pm . 21 Continuing Education Credit . 9 Poster Session 3: Saturday 9:30 am . 22 Thursday (Schedule).................... 11 Exhibitors............................. 25 Downstairs Floor Plan of the Cajundome Partners............................... 25 Convention Center .................. 11 Advertisers............................ 25 Upstairs floor plan for the Cajundome Planning & Organizing Committee . 25 Convention Center .................. 12 Index of Names & Companies . 26 Friday (Schedule) ..................... 13 Copyright © of this Program for Autism07 by the Sertoma Club of Lafayette 2007 Foreword The autism puzzle is about it? This conference addresses that critical question among the most troubling along with questions about the diagnosis and treatment of of today’s world. Severe autism and related disorders. Autism07 has received the autism robs parent and highest possible rating for continuing education from the child of a normal relation American Medical Association. Qualified participants can with each other. Jon receive up to 13.25 AMA PRA Category 1 CreditsTM . Shestack, the producer of Continuing education is also available to dentists, nurses, Father of the Bride and behavior analysts, psychologists, hygienists, social other Hollywood motion workers, occupational therapists, teachers, and -
SCIENCE and HEALTH MISINFORMATION in the DIGITAL AGE: How Does It Spread? Who Is Vulnerable? How Do We Fight It?
SCIENCE AND HEALTH MISINFORMATION IN THE DIGITAL AGE: How does it spread? Who is vulnerable? How do we fight it? ERIC MERKLEY & PETER LOEWEN J U LY, 2021 ABOUT PPF Good Policy. Better Canada. The Public Policy Forum builds bridges among diverse participants in the policy-making process and gives them a platform to examine issues, offer new perspectives and feed fresh ideas into critical policy discussions. We believe good policy is critical to making a better Canada—a country that’s cohesive, prosperous and secure. We contribute by: . Conducting research on critical issues . Convening candid dialogues on research subjects . Recognizing exceptional leaders Our approach—called Inclusion to Conclusion—brings emerging and established voices to policy conversations, which informs conclusions that identify obstacles to success and pathways forward. PPF is an independent, non-partisan charity whose members are a diverse group of private, public and non-profit organizations. ppforum.ca @ppforumca © 2021, Public Policy Forum 1400 - 130 Albert Street Ottawa, ON, Canada, K1P 5G4 613.238.7858 ISBN: 978-1-77452-085-7 WITH THANKS TO OUR PARTNERS ABOUT THE AUTHORS ERIC MERKLEY Eric Merkley (PhD, UBC) is an Assistant Professor in the Department of Political Science at the University of Toronto. He was the lead survey analyst of the Media Ecosystem Observatory, which studied the Canadian information ecosystem and public opinion during the COVID-19 pandemic, and the Digital Democracy Project, which studied misinformation and public attitudes during the 2019 Canadian federal election. His research focuses on the link between political elite behaviour, the news media, and public opinion. -
Interpersonal Communication for Immunization Training for Front Line Workers
1 Participant manual Interpersonal Communication for Immunization Training for Front Line Workers UNICEF Europe and Central Asia Region 2 Interpersonal Communication for Immunization. Participant manual Participant manual Interpersonal Communication for Immunization Training for Front Line Workers UNICEF Europe and Central Asia Region 4 Interpersonal Communication for Immunization. Participant manual Acknowledgements This training package was developed by the Johns Hopkins Center for Communication Programs, the UNICEF Europe and Central Asia Regional Office, and UNICEF Country Office staff in Bosnia and Herzegovina and Serbia. We would like to thank Sergiu Tomsa, UNICEF Regional Communication for Development Specialist, Mario Mosquera, UNICEF Regional Communication for Development Adviser and Svetlana Stefanet, UNICEF Regional Immunization Specialist, for their significant contributions to its conceptualization and development. We also thank Fatima Cengic, Health and Nutrition Specialist, UNICEF Bosnia and Herzegovina and Jelena Zajeganovic-Jakovljevic, Early Childhood Development Specialist, UNICEF Serbia, as well as Dragoslav Popovic, consultant, the representatives of Institutes of Public Health, academia, health workers, Roma community mediators and civil society organizations from both countries for their support and active engagement in pre-testing and finalizing the package. The materials are based on state-of-the-art resources from UNICEF, the World Health Organization (WHO), European and American Centers for Disease Control, academic journals and the immunization websites of a range of governments and foundations. Authors: Robert Karam, Johns Hopkins Center for Communication Programs Waverly Rennie, Consultant, Johns Hopkins Center for Communication Programs Stephanie Clayton, Johns Hopkins Center for Communication Programs Design: Benussi&theFish Cover Photo: © UNICEF/UN040868/Bicanski © United Nations Children’s Fund (UNICEF), 2019. Some rights reserved. -

IN the UNITED STATES COURT of FEDERAL CLAIMS OFFICE of SPECIAL MASTERS No. 01-162V Filed: February 12, 2009 to Be Published
IN THE UNITED STATES COURT OF FEDERAL CLAIMS OFFICE OF SPECIAL MASTERS No. 01-162V Filed: February 12, 2009 To Be Published * * * * * * * * * * * * * * * * * * * * * * * * * * * * COLTEN SNYDER, by and through * KATHRYN SNYDER and JOSEPH SNYDER, * his natural guardians and next friends * Omnibus Autism * Proceeding; * Autism Spectrum Disorder, * Pervasive Developmental * Disorder, Causation, Petitioners, * Measles, MMR, Mercury, * Thimerosal, Waiver v. * Applying Daubert, * Weight of Expert Opinions, SECRETARY OF THE DEPARTMENT * Credibility of Witnesses OF HEALTH AND HUMAN SERVICES, * * Respondent. * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * Christopher W. Wickersham, Sr., Esq., Lloyd Bowers, Esq., and Thomas B. Powers, Esq., for petitioners. Alexis S. Babcock, Esq., Katherine Esposito, Esq., Voris Johnson, Esq., and Vincent Matanoski, Esq., U.S. Department of Justice, Washington, DC, for respondent. DECISION1 Vowell, Special Master: On March 22, 2001, Kathryn and Joseph Snyder [“petitioners”] filed a petition for compensation under the National Vaccine Injury Compensation Program, 42 U.S.C. 1 Vaccine Rule 18(b) provides the parties 14 days to request redaction of any material “(i) which is trade secret or commercial or financial information which is privileged and confidential, or (ii) which are medical files and similar files, the disclosure of which would constitute a clearly unwarranted invasion of privacy.” 42 U.S.C. § 300aa12(d)(4)(B). Petitioners have waived their right to request such redaction. See Petitioners’ Notice to W aive the 14-Day “W aiting” Period as Defined in Vaccine Rule 18(b), filed December 2, 2008. Respondent also waived the right to object to the disclosure of information submitted by respondent. See Respondent’s Consent to Disclosure, filed January 14, 2009. Accordingly, this decision will be publicly available immediately after it is filed. -

Correlation of Influenza Vaccination and Influenza Incidence on Covid-19 Severity
Influenza and Covid-19 severity 1 Report Correlation of Influenza Vaccination and Influenza Incidence on Covid-19 Severity Mark Christopher Arokiaraj, MD DM, Cardiology, Pondicherry Institute of Medical Sciences, India 605014. [email protected] Key words: Covid-19, Influenza vaccination, Influenza lower respiratory tract infections, Mortality, Morbidity, Immunity. Abstract The pandemic of Covid-19 is evolving worldwide, and it is associated with high mortality and morbidity. There is a growing need to discuss the elements of coordinated strategy to control the spread and mitigate the severity and mortality of Covid-19. H1N1 vaccine and streptococcus pneumonia vaccines are available. The current analysis was performed to correlate the severity of Covid-19 and influenza (H1N1) vaccination statistics and also the influenza lower respiratory tract incidence. There is a correlation between Covid-19 related mortality and morbidity and the status of influenza vaccination, which appears protective. The tendency of correlation is more visualized as the pandemic is evolving. The case incidence and recovery parameters also showed a beneficial trend. Since evolutionarily influenza is close to SARS-CoV-2 viruses and shares some common epitopes and mechanisms, there is a possibility of partial protection to reduce the Covid-19 related severity using the influenza vaccination. In countries where influenza immunization is less, there is a correlation between lower respiratory tract infections (LRI) and influenza attributable to lower respiratory tract infections incidence and Covid-19 severity, which is beneficial. Receiver operating curve (ROC) statistics showed an area under the curve of 0.86 (CI 0.78 to 0.944, P <0.0001) to predict Covid-19 mortality >150/million, and a decreasing trend of influenza LRI episodes.