Coronary Artery Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

J Wave and Cardiac Death in Inferior Wall Myocardial Infarction
ORIGINAL ARTICLES Arrhythmia 2015;16(2):67-77 J Wave and Cardiac Death in Inferior Wall Myocardial Infarction Myung-Jin Cha, MD; Seil Oh, MD, ABSTRACT PhD, FHRS Background and Objectives: The clinical significance of J wave Department of Internal Medicine, Seoul National University presentation in acute myocardial infarction (AMI) patients remains Hospital, Seoul, Korea unclear. We hypothesized that J wave appearance in the inferior leads and/or reversed-J (rJ) wave in leads V1-V3 is associated with poor prognosis in inferior-wall AMI patients. Subject and Methods: We enrolled 302 consecutive patients with inferior-wall AMI who were treated with percutaneous coronary in- tervention (PCI). Patients were categorized into 2 groups based on electrocardiograms before and after PCI: the J group (J waves in in- ferior leads and/or rJ waves in leads V1-V3) and the non-J group (no J wave in any of the 12 leads). We compared patients with high am- plitude (>2 mV) J or rJ waves (big-J group) with the non-J group. The cardiac and all-cause mortality at 6 months and post-PCI ventricular arrhythmic events ≤48 hours after PCI were analyzed. Results: A total of 29 patients (including 19 cardiac death) had died. Although all-cause mortality was significantly higher in the post-PCI J group than in the non-J group (p=0.001, HR=5.38), there was no difference between the groups in cardiac mortality. When compar- ing the post-PCI big-J group with the non-J group, a significant dif- ference was found in all-cause mortality (n=29, p=0.032, HR=5.4) and cardiac mortality (n=19, p=0.011, HR=32.7). -

Unstable Angina with Tachycardia: Clinical and Therapeutic Implications
Unstable angina with tachycardia: Clinical and therapeutic implications We prospectively evaluated 19 patients with prolonged chest pain not evolving to myocardiai infarction and accompanied with reversible ST-T changes and tachycardia (heart rate >lOO beats/min) in order to correlate heart rate reduction with ischemic electrocardiographic (ECG) changes. Fourteen patients (74%) received previous long-term combined treatment with nifedipine and nitrates. Continuous ECG monitoring was carried out until heart rate reduction and at least one of the following occurred: (1) relief of pain or (2) resolution of ischemic ECG changes. The study protocol consisted of carotid massage in three patients (IS%), intravenous propranolol in seven patients (37%), slow intravenous amiodarone infusion in two patients (lo%), and intravenous verapamil in four patients (21%) with atrial fibrillation. In three patients (16%) we observed a spontaneous heart rate reduction on admission. Patients responded with heart rate reduction from a mean of 126 + 10.4 beats/min to 64 k 7.5 beats/min (p < 0.005) and an ST segment shift of 4.3 k 2.13 mm to 0.89 k 0.74 mm (p < 0.005) within a mean interval of 13.2 + 12.7 minutes. Fifteen (79%) had complete response and the other four (21%) had partial relief of pain. A significant direct correlation was observed for heart rate reduction and ST segment deviation (depression or elevation) (f = 0.7527 and 0.8739, respectively). These patients represent a unique subgroup of unstable angina, in which the mechanism responsible for ischemia is excessive increase in heart rate. Conventional vasodilator therapy may be deleterious, and heart rate reduction Is mandatory. -

The J Wave of the ECG. Concepts Compiled by Dr
The J wave of the ECG. Concepts Compiled by Dr. Andrés R. Pérez Riera The J wave is a positive deflection in the ECG normal (present in 2%–14% of healthy individuals and is more prevalent in young males, particularly if athletic and African descent. Additionally, ERP is a common finding in young teen athletes (the prevalence in the athletic population rises to 20-90%.).1 In this population ERP in both inferior and lateral leads is more common (18.2%) than isolated inferior (9.1%) or lateral (8.2%) ERP. Young age might be a contributing factor in causing a more diffuse repolarization abnormality. 2 or pathological that occurs approximately (There is an overlap of ≈10 msec. 3) after the junction between the end of the QRS complex and the beginning of the ST segment, also known as the J point (junction point), QRS end, J-junction, ST0 [zero millisecond] or ST beginning to occur after the notch/slur or J wave 4. It is described as J deflection as slurring/lambda 5 or notching of the terminal portion of QRS complex. Currently, J waves, is defined as an elevation of the QRS-ST junction ≥1 mm either as QRS slurring or notching in at least 2 contiguous leads. Additionally, when it becomes more accentuated, it may appear as a small, R wave (R′) or ST segment elevation. The term J deflection or J-wave has been used to designate the formation of the wave produced when there is a large, prominent deviation of the J point from the baseline with two shapes: notching/spike-and- slurring/lambda 5 or dome 6 variety. -

Heart Valve Disease: Mitral and Tricuspid Valves
Heart Valve Disease: Mitral and Tricuspid Valves Heart anatomy The heart has two sides, separated by an inner wall called the septum. The right side of the heart pumps blood to the lungs to pick up oxygen. The left side of the heart receives the oxygen- rich blood from the lungs and pumps it to the body. The heart has four chambers and four valves that regulate blood flow. The upper chambers are called the left and right atria, and the lower chambers are called the left and right ventricles. The mitral valve is located on the left side of the heart, between the left atrium and the left ventricle. This valve has two leaflets that allow blood to flow from the lungs to the heart. The tricuspid valve is located on the right side of the heart, between the right atrium and the right ventricle. This valve has three leaflets and its function is to Cardiac Surgery-MATRIx Program -1- prevent blood from leaking back into the right atrium. What is heart valve disease? In heart valve disease, one or more of the valves in your heart does not open or close properly. Heart valve problems may include: • Regurgitation (also called insufficiency)- In this condition, the valve leaflets don't close properly, causing blood to leak backward in your heart. • Stenosis- In valve stenosis, your valve leaflets become thick or stiff, and do not open wide enough. This reduces blood flow through the valve. Blausen.com staff-Own work, CC BY 3.0 Mitral valve disease The most common problems affecting the mitral valve are the inability for the valve to completely open (stenosis) or close (regurgitation). -

Coronary Artery Disease
Coronary Artery Disease INFORMATION GUIDE Other names: Atherosclerosis CAD Coronary heart disease (CHD) Hardening of the arteries Heart disease Ischemic (is-KE-mik) heart disease Narrowing of the arteries The purpose of this guide is to help patients and families find sources of information and support. This list is not meant to be comprehensive, but rather to provide starting points for information seeking. The resources may be obtained at the Mardigian Wellness Resource Center located off the Atrium on Floor 2 of the Cardiovascular Center. Visit our website at http://www.umcvc.org/mardigian-wellness-resource-center and online Information guides at http://infoguides.med.umich.edu/home Books, Brochures, Fact Sheets Michigan Medicine. What is Ischemic Heart Disease and Stroke. http://www.med.umich.edu/1libr/CCG/IHDshort.pdf National Heart, Lung and Blood Institute (NHLBI). In Brief: Your Guide to Living Well with Heart Disease. A four-page fact sheet. Available online at: http://www.nhlbi.nih.gov/health/public/heart/other/your_guide/living_hd_f s.pdf National Heart, Lung and Blood Institute (NHLBI). Your Guide to Living Well with Heart Disease. A 68-page booklet is a step-by-step guide to helping people with heart disease make decisions that will protect and improve their lives A printer- friendly version is available at: http://www.nhlbi.nih.gov/health/public/heart/other/your_guide/living_well. pdf Coronary Artery Disease Page 1 Mardigian Wellness Resource Center Coronary Artery Disease INFORMATION GUIDE Books Bale, Bradley. Beat the Heart Attack Gene: A Revolutionary Plan to Prevent Heart Disease, Stroke and Diabetes. New York, NY: Turner Publishing, 2014. -

Association of Cardiomegaly with Coronary Artery Histopathology and Its Relationship to Atheroma
32 Journal of Atherosclerosis and Thrombosis Vol.18, No.1 Coronary Histopathology in Cardiomegaly 33 Original Article Association of Cardiomegaly with Coronary Artery Histopathology and its Relationship to Atheroma Richard Everett Tracy Department of Pathology, Louisiana State University Health Sciences Center, New Orleans, USA Aims: Hypertrophied hearts at autopsy often display excessive coronary artery atherosclerosis, but the histopathology of coronary arteries in hearts with and without cardiomegaly has rarely been com- pared. Methods: In this study, forensic autopsies provided hearts with unexplained enlargement plus com- parison specimens. Right coronary artery was opened longitudinally and flattened for formalin fixa- tion and H&E-stained paraffin sections were cut perpendicular to the endothelial surface. The mi- croscopically observed presence or absence of a necrotic atheroma in the specimen was recorded. At multiple sites far removed from any form of atherosclerosis, measurements were taken of intimal thickness, numbers of smooth muscle cells (SMC) and their ratio, the thickness per SMC, averaged over the entire nonatheromatous arterial length. When the mean thickness per SMC exceeded a cer- tain cutoff point, the artery was declared likely to contain a necrotic atheroma. Results: The prevalence of specimens with necrotic atheromas increased stepwise with increasing heart weight, equally with fatal or with incidental cardiomegaly, and equally with hypertension- or obesity-related hypertrophy, rejecting further inclusion of appreciable age, race, or gender effects. The prevalence of specimens with thickness per SMC exceeding the cutoff point was almost always nearly identical to the prevalence of observed necrotic atheroma, showing the two variables to be tightly linked to each other with quantitative consistency across group comparisons of every form. -

The Management of Acute Coronary Syndromes in Patients Presenting
CONCISE GUIDANCE Clinical Medicine 2021 Vol 21, No 2: e206–11 The management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: key points from the ESC 2020 Clinical Practice Guidelines for the general and emergency physician Authors: Ramesh NadarajahA and Chris GaleB There have been significant advances in the diagnosis and international decline in mortality rates.2,3 In September 2020, management of non-ST-segment elevation myocardial the European Society of Cardiology (ESC) published updated infarction over recent years, which has been reflected in an Clinical Practice Guidelines for the management of ACS in patients international decline in mortality rates. This article provides an presenting without persistent ST-segment elevation,4 5 years after overview of the 2020 European Society of Cardiology Clinical the last iteration. ABSTRACT Practice Guidelines for the topic, concentrating on areas relevant The guidelines stipulate a number of updated recommendations to the general or emergency physician. The recommendations (supplementary material S1). The strength of a recommendation and underlying evidence basis are analysed in three key and level of evidence used to justify it are weighted and graded areas: diagnosis (the recommendation to use high sensitivity according to predefined scales (Table 1). This focused review troponin and how to apply it), pathways (the recommendation provides learning points derived from the guidelines in areas to facilitate early invasive coronary angiography to improve relevant to general and emergency physicians, including diagnosis outcomes and shorten hospital stays) and treatment (a (recommendation to use high sensitivity troponin), pathways paradigm shift in the use of early intensive platelet inhibition). -
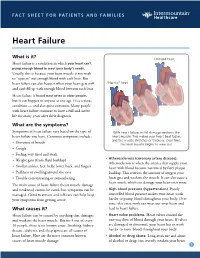
Heart Failure
FACT SHEET FOR PATIENTS AND FAMILIES Heart Failure What is it? Enlarged heart Heart failure is a condition in which your heart can’t pump enough blood to meet your body’s needs. Usually, this is because your heart muscle is too weak to “squeeze” out enough blood with each beat. But heart failure can also happen when your heart gets stiff “Normal” heart and can’t fill up with enough blood between each beat. Heart failure is found most often in older people, but it can happen to anyone at any age. It’s a serious condition — and also quite common. Many people with heart failure continue to have a full and active life for many years after their diagnosis. What are the symptoms? Symptoms of heart failure vary based on the type of With heart failure, initial damage weakens the heart failure you have. Common symptoms include: heart muscle. This makes your heart beat faster, and the muscle stretches or thickens. Over time, • Shortness of breath the heart muscle begins to wear out. • Cough • Feeling very tired and weak • Atherosclerosis (coronary artery disease). • Weight gain (from fluid buildup) Atherosclerosis is when the arteries that supply your • Swollen ankles, feet, belly, lower back, and fingers heart with blood become narrowed by fatty plaque • Puffiness or swelling around the eyes buildup. This restricts the amount of oxygen your • Trouble concentrating or remembering heart gets and weakens the muscle. It can also cause a heart attack, which can damage your heart even more. The main cause of heart failure (heart muscle damage and weakness) cannot be cured, but symptoms can be • High blood pressure (hypertension). -

Risk Stratification in Acute Coronary Syndrome: Focus on Unstable Angina/Non-ST Segment Elevation Myocardial Infarction R Bugiardini
729 EDITORIAL Heart: first published as 10.1136/hrt.2004.034546 on 14 June 2004. Downloaded from Risk stratification in acute coronary syndrome: focus on unstable angina/non-ST segment elevation myocardial infarction R Bugiardini ............................................................................................................................... Heart 2004;90:729–731. doi: 10.1136/hrt.2004.034546 Although there have been advances in the management of fashion. Experts in a variety of fields make decisions using a more intuitive process of unstable angina/non-ST segment elevation myocardial recognising patterns and applying their own infarction syndromes, the rate of cardiovascular mortality rules. In varying proportions, pathophysiologic after discharge is still unacceptably high. With many reasoning, personal clinical experience, and recent published research each play a role in therapeutic options available, the clinician is challenged to the development of our own clinical rules. This identify the safest and most effective treatment for long term approach may produce incorrect use of tools of survival of each individual patient risk stratifications and inappropriate use of treatment strategies and procedures. However, ........................................................................... errors are more often due to ‘‘failure’’ of the system, not of the doctors. Most errors occur at the transfer of care, and particularly at the transfer from the outpatient to the inpatient ‘‘Simple, but not too simple’’—Albert Einstein sites. There are a number of programs now focusing on errors and strategies to reduce errors welve million individuals in the USA and (GAP, CRUSADE QI, JACHO).5–7 All of these 143 million worldwide have coronary artery programs focus on education of physicians, Tdisease. Two million US patients are better interaction between health care organisa- admitted annually to cardiac care units with tions and physicians, and appropriate use of care acute coronary syndromes (ACS). -

Angina: Contemporary Diagnosis and Management Thomas Joseph Ford ,1,2,3 Colin Berry 1
Education in Heart CHRONIC ISCHAEMIC HEART DISEASE Heart: first published as 10.1136/heartjnl-2018-314661 on 12 February 2020. Downloaded from Angina: contemporary diagnosis and management Thomas Joseph Ford ,1,2,3 Colin Berry 1 1BHF Cardiovascular Research INTRODUCTION Learning objectives Centre, University of Glasgow Ischaemic heart disease (IHD) remains the leading College of Medical Veterinary global cause of death and lost life years in adults, and Life Sciences, Glasgow, UK ► Around one half of angina patients have no 2 notably in younger (<55 years) women.1 Angina Department of Cardiology, obstructive coronary disease; many of these Gosford Hospital, Gosford, New pectoris (derived from the Latin verb ‘angere’ to patients have microvascular and/or vasospastic South Wales, Australia strangle) is chest discomfort of cardiac origin. It is a 3 angina. Faculty of Health and Medicine, common clinical manifestation of IHD with an esti- The University of Newcastle, ► Tests of coronary artery function empower mated prevalence of 3%–4% in UK adults. There Newcastle, NSW, Australia clinicians to make a correct diagnosis (rule- in/ are over 250 000 invasive coronary angiograms rule- out), complementing coronary angiography. Correspondence to performed each year with over 20 000 new cases of ► Physician and patient education, lifestyle, Dr Thomas Joseph Ford, BHF angina. The healthcare resource utilisation is appre- medications and revascularisation are key Cardiovascular Research Centre, ciable with over 110 000 inpatient episodes each aspects of management. University of Glasgow College year leading to substantial associated morbidity.2 In of Medical Veterinary and Life Sciences, Glasgow G128QQ, UK; 1809, Allen Burns (Lecturer in Anatomy, Univer- tom. -

KNOW the FACTS ABOUT Heart Disease
KNOW THE FACTS ABOUT Heart Disease What is heart disease? Having high cholesterol, high blood pressure, or diabetes also can increase Heart disease is the leading cause of your risk for heart disease. Ask your death in the United States. More than doctor about preventing or treating these 600,000 Americans die of heart disease medical conditions. each year. That’s one in every four deaths in this country.1 What are the signs and symptoms? The term “heart disease” refers to several The symptoms vary depending on the types of heart conditions. The most type of heart disease. For many people, common type is coronary artery disease, chest discomfort or a heart attack is the which can cause heart attack. Other first sign. kinds of heart disease may involve the Someone having a heart attack may valves in the heart, or the heart may not experience several symptoms, including: pump well and cause heart failure. Some people are born with heart disease. l Chest pain or discomfort that doesn’t go away after a few minutes. l Pain or discomfort in the jaw, neck, Are you at risk? or back. Anyone, including children, can l Weakness, light-headedness, nausea develop heart disease. It occurs when (feeling sick to your stomach), or a substance called plaque builds up in a cold sweat. your arteries. When this happens, your arteries can narrow over time, reducing l Pain or discomfort in the arms blood flow to the heart. or shoulder. Smoking, eating an unhealthy diet, and l Shortness of breath. not getting enough exercise all increase If you think that you or someone you your risk for having heart disease. -

SIGN 152 • Cardiac Arrhythmias in Coronary Heart Disease
www.healthcareimprovementscotland.org Edinburgh Office | Gyle Square |1 South Gyle Crescent | Edinburgh | EH12 9EB Telephone 0131 623 4300 Fax 0131 623 4299 Glasgow Office | Delta House | 50 West Nile Street | Glasgow | G1 2NP Telephone 0141 225 6999 Fax 0141 248 3776 The Healthcare Environment Inspectorate, the Scottish Health Council, the Scottish Health Technologies Group, the Scottish Intercollegiate Guidelines Network (SIGN) and the Scottish Medicines Consortium are key components of our organisation. SIGN 152 • Cardiac arrhythmias in coronary heart disease A national clinical guideline September 2018 Evidence KEY TO EVIDENCE STATEMENTS AND RECOMMENDATIONS LEVELS OF EVIDENCE 1++ High-quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low risk of bias 1+ Well-conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias 1 - Meta-analyses, systematic reviews, or RCTs with a high risk of bias High-quality systematic reviews of case-control or cohort studies ++ 2 High-quality case-control or cohort studies with a very low risk of confounding or bias and a high probability that the relationship is causal Well-conducted case-control or cohort studies with a low risk of confounding or bias and a moderate probability that the 2+ relationship is causal 2 - Case-control or cohort studies with a high risk of confounding or bias and a significant risk that the relationship is not causal 3 Non-analytic studies, eg case reports, case series 4 Expert opinion RECOMMENDATIONS Some recommendations can be made with more certainty than others. The wording used in the recommendations in this guideline denotes the certainty with which the recommendation is made (the ‘strength’ of the recommendation).