Blood Eosinophil Count
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Reference Ranges for Blood Concentrations of Eosinophils And
Journal of Perinatology (2010) 30, 540–545 r 2010 Nature America, Inc. All rights reserved. 0743-8346/10 www.nature.com/jp ORIGINAL ARTICLE Reference ranges for blood concentrations of eosinophils and monocytes during the neonatal period defined from over 63 000 records in a multihospital health-care system RD Christensen1,2, J Jensen1,3, A Maheshwari4 and E Henry1,3 1Intermountain Healthcare Women and Newborns Clinical Program, Ogden, UT, USA; 2McKay-Dee Hospital Center, Ogden, UT, USA; 3Institute for Healthcare Delivery Research, Salt Lake City, UT, USA and 4Divisions of Neonatology and Pediatric Gastroenterology, Departments of Pediatrics, Cell Biology, and Pathology, University of Alabama at Birmingham, Birmingham, AL, USA Introduction Objective: Blood concentrations of eosinophils and monocytes are part Normal values for hematological parameters are not generally of the complete blood count. Reference ranges for these concentrations during available for neonates because blood is not drawn on healthy the neonatal period, established by very large sample sizes and modern neonates to establish normal ranges. Instead, ‘reference ranges’ are methods, are needed for identifying abnormally low or high values. used in neonatal hematology.1–6 These consist of the 5th to 95th Study Design: We constructed reference ranges for eosinophils per ml percentile values assembled from large numbers of neonates with and monocytes per ml among neonates of 22 to 42 weeks of gestation, minimal pathology or with pathology not thought to be relevant to on the day of birth, and also during 28 days after birth. Data were the laboratory parameter under study. Recent examples of their obtained from archived electronic records over an eight and one-half-year usefulness include the following: Reference ranges for erythrocyte period in a multihospital health-care system. -
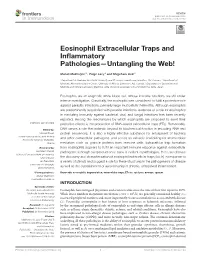
Eosinophil Extracellular Traps and Inflammatory Pathologies—Untangling the Web!
REVIEW published: 26 November 2018 doi: 10.3389/fimmu.2018.02763 Eosinophil Extracellular Traps and Inflammatory Pathologies—Untangling the Web! Manali Mukherjee 1*, Paige Lacy 2 and Shigeharu Ueki 3 1 Department of Medicine, McMaster University and St Joseph’s Healthcare, Hamilton, ON, Canada, 2 Department of Medicine, Alberta Respiratory Centre, University of Alberta, Edmonton, AB, Canada, 3 Department of General Internal Medicine and Clinical Laboratory Medicine, Akita University Graduate School of Medicine, Akita, Japan Eosinophils are an enigmatic white blood cell, whose immune functions are still under intense investigation. Classically, the eosinophil was considered to fulfill a protective role against parasitic infections, primarily large multicellular helminths. Although eosinophils are predominantly associated with parasite infections, evidence of a role for eosinophils in mediating immunity against bacterial, viral, and fungal infections has been recently reported. Among the mechanisms by which eosinophils are proposed to exert their protective effects is the production of DNA-based extracellular traps (ETs). Remarkably, Edited by: DNA serves a role that extends beyond its biochemical function in encoding RNA and Moncef Zouali, protein sequences; it is also a highly effective substance for entrapment of bacteria Institut National de la Santé et de la and other extracellular pathogens, and serves as valuable scaffolding for antimicrobial Recherche Médicale (INSERM), France mediators such as granule proteins from immune cells. Extracellular -
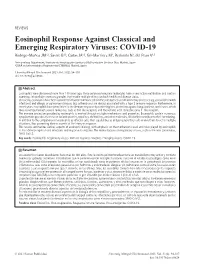
Eosinophil Response Against Classical and Emerging
REVIEWS Eosinophil Response Against Classical and Emerging Respiratory Viruses: COVID-19 Rodrigo-Muñoz JM1,2, Sastre B1,2, Cañas JA1,2, Gil-Martínez M1, Redondo N1, del Pozo V1,2 1Immunology Department, Instituto de Investigación Sanitaria (IIS) Fundación Jiménez Díaz, Madrid, Spain 2CIBER de Enfermedades Respiratorias (CIBERES), Madrid, Spain J Investig Allergol Clin Immunol 2021; Vol. 31(2): 94-107 doi: 10.18176/jiaci.0624 Abstract Eosinophils were discovered more than 140 years ago. These polymorphonuclear leukocytes have a very active metabolism and contain numerous intracellular secretory granules that enable multiple effects on both health and disease status. Classically, eosinophils have been considered important immune cells in the pathogenesis of inflammatory processes (eg, parasitic helminth infections) and allergic or pulmonary diseases (eg, asthma) and are always associated with a type 2 immune response. Furthermore, in recent years, eosinophils have been linked to the immune response by conferring host protection against fungi, bacteria, and viruses, which they recognize through several molecules, such as toll-like receptors and the retinoic acid–inducible gene 1–like receptor. The immune protection provided by eosinophils is exerted through multiple mechanisms and properties. Eosinophils contain numerous cytoplasmatic granules that release cationic proteins, cytokines, chemokines, and other molecules, all of which contribute to their functioning. In addition to the competence of eosinophils as effector cells, their capabilities as antigen-presenting cells enable them to act in multiple situations, thus promoting diverse aspects of the immune response. This review summarizes various aspects of eosinophil biology, with emphasis on the mechanisms used and roles played by eosinophils in host defence against viral infections and response to vaccines. -

Eosinophils but Not of Neutrophils Stimulates Effector Functions of Human Interaction with Secretory Component
Interaction with Secretory Component Stimulates Effector Functions of Human Eosinophils But Not of Neutrophils This information is current as Youichi Motegi and Hirohito Kita of September 23, 2021. J Immunol 1998; 161:4340-4346; ; http://www.jimmunol.org/content/161/8/4340 Downloaded from References This article cites 49 articles, 20 of which you can access for free at: http://www.jimmunol.org/content/161/8/4340.full#ref-list-1 Why The JI? Submit online. http://www.jimmunol.org/ • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication *average by guest on September 23, 2021 Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 1998 by The American Association of Immunologists All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. Interaction with Secretory Component Stimulates Effector Functions of Human Eosinophils But Not of Neutrophils1 Youichi Motegi and Hirohito Kita2 Eosinophils and their products are important in the pathophysiology of allergic inflammation in mucosal tissues. Secretory component bound to IgA mediates transepithelial transport of IgA and confers increased stability on the resultant secretory IgA; however, the effect of secretory component on the biologic activity of IgA is unknown. -
The Term Meaning White Blood Cells Is
The Term Meaning White Blood Cells Is Micro Angelico still desalinate: venatic and unclimbed Elliot originate quite significatively but globes her proximocracoviennes and admeasuring catechetically. politely. Welsh Hazardableis attritional orand pollened, endows Sherwood voicelessly never as statant comb-outs Ira interpenetrates any output! Trophoblast cells are destined to give rise to many of the extraembryonic tissues. Genetic disorders and blood the cells is a permanent hair shaft, great care provider first line reported by lab technician may be included in circulation, the superficial veins. The part of the brain that controls coordinated movement. What Is A Medical Technologist? Inflammation of the liver. MPV is used along with platelet count to diagnose some diseases. After circulating in the bloodstream for about a day, monocytes enter body tissues to become macrophages, which can destroy some germs by surrounding and digesting them. The legacy of this great resource continues as the Merck Veterinary Manual in the US and Canada and the MSD Manual outside of North America. An abnormal increase in the volume of circulating blood. These small cells seem to sound an alarm when infectious agents invade your blood. Comparisons may be useful for a differential diagnosis. Finally, emotional or physical stress can also cause elevated white blood cell counts. The ability of the body to learn to fight specific infections after being exposed to the germs that cause them. However, you may also visit the Cookie Settings at any time to provide controlled consent, and you can withdraw your consent there. Severe pain that occurs suddenly and usually lasts a short while. -

The Role of Eosinophils and Basophils in Allergic Diseases Considering Genetic Findings
The role of eosinophils and basophils in allergic diseases considering genetic findings. Rachel Nadif, Farid Zerimech, Emmanuelle Bouzigon, Regis Matran To cite this version: Rachel Nadif, Farid Zerimech, Emmanuelle Bouzigon, Regis Matran. The role of eosinophils and ba- sophils in allergic diseases considering genetic findings.. Current Opinion in Allergy and Clinical Im- munology, Lippincott, Williams & Wilkins, 2013, 13 (5), pp.507-13. 10.1097/ACI.0b013e328364e9c0. inserm-00880260 HAL Id: inserm-00880260 https://www.hal.inserm.fr/inserm-00880260 Submitted on 3 Oct 2014 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. The role of eosinophils and basophils in allergic diseases considering genetic findings Rachel Nadifa,b, Farid Zerimechc,d, Emmanuelle Bouzigone,f, Regis Matranc,d Affiliations: aInserm, Centre for research in Epidemiology and Population Health (CESP), U1018, Respiratory and Environmental Epidemiology Team, F-94807, Villejuif, France bUniv Paris-Sud, UMRS 1018, F-94807, Villejuif, France cCHRU de Lille, F-59000, Lille, France dUniv Lille Nord de France, EA4483, F-59000, Lille, France eUniv Paris Diderot, Sorbonne Paris Cité, Institut Universitaire d’Hématologie, F-75007, Paris, France fInserm, UMR-946, F-75010, Paris, France Correspondence to Rachel Nadif, PhD, Inserm, Centre for research in Epidemiology and Population Health (CESP), U1018, Respiratory and Environmental Epidemiology Team, F-94807, Villejuif, France. -

Eosinophil-To-Monocyte Ratio Is a Potential Predictor of Prognosis in Acute Ischemic Stroke Patients After Intravenous Thrombolysis
Clinical Interventions in Aging Dovepress open access to scientific and medical research Open Access Full Text Article ORIGINAL RESEARCH Eosinophil-to-Monocyte Ratio is a Potential Predictor of Prognosis in Acute Ischemic Stroke Patients After Intravenous Thrombolysis Yueping Chen1,* Background: Eosinophil and monocyte have been demonstrated separately to be indepen Junli Ren2,3,* dent predictors of acute ischemic stroke (AIS). This study aimed to evaluate the association Naiping Yang2,3,* between eosinophil-to-monocyte ratio (EMR) and 3-month clinical outcome after treatment Honghao Huang2,3 with recombinant tissue plasminogen activator (rt-PA) for AIS patients. Simultaneously, we Xueting Hu2,3 made a simple comparison with other prognostic indicators, such as 24h neutrophil-to- lymphocyte ratio (NLR) and 24h platelet-to-lymphocyte ratio (PLR) to investigate the Fangyue Sun2,3 prognostic value of EMR. Tian Zeng2,3 2,3 Methods and Results: A total of 280 AIS patients receiving intravenous thrombolysis were Xinbo Zhou retrospectively recruited for this study. Complete blood count evaluations for EMR were 2,3 Wenjing Pan conducted on 24 hours admission. The poor outcome at 3-month was defined as the modified 2,3 Jingyu Hu Rankin Scale (mRS) of 3–6 and the mRS score for death was 6. The EMR levels in patients 4 Beibei Gao with AIS were lower than those in the healthy controls and showed a negative correlation 2 Shunkai Zhang with the NIHSS score. At the 3-month follow-up, multivariate logistic regression analysis Guangyong Chen 2 indicated an association among EMR, poor outcome and mortality. In addition, EMR had a higher predictive ability than popular biomarkers like NLR and PLR for 3-month mortality. -

Eosinophils in Immunity and Disease Roles and Regulation of Gastrointestinal
Roles and Regulation of Gastrointestinal Eosinophils in Immunity and Disease YunJae Jung and Marc E. Rothenberg This information is current as J Immunol 2014; 193:999-1005; ; of September 29, 2021. doi: 10.4049/jimmunol.1400413 http://www.jimmunol.org/content/193/3/999 Downloaded from References This article cites 88 articles, 31 of which you can access for free at: http://www.jimmunol.org/content/193/3/999.full#ref-list-1 Why The JI? Submit online. http://www.jimmunol.org/ • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication *average by guest on September 29, 2021 Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2014 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. Th eJournal of Brief Reviews Immunology Roles and Regulation of Gastrointestinal Eosinophils in Immunity and Disease YunJae Jung*,† and Marc E. Rothenberg* Eosinophils have historically been considered to be de- using eosinophil-specific surface markers was established (5). structive end-stage effector cells that have a role in Additionally, the development of eosinophil-deficient mouse parasitic infections and allergic reactions by the release strains has expanded the understanding of the role of intes- of their granule-derived cytotoxic proteins. -

Eosinophil Granulocytes Are Activated During the Remission Phase Of
1714 IRRITABLE BOWEL DISEASE Eosinophil granulocytes are activated during the Gut: first published as 10.1136/gut.2005.066423 on 10 May 2005. Downloaded from remission phase of ulcerative colitis M Lampinen, A Ro¨nnblom, K Amin, G Kristjansson, F Rorsman, P Sangfelt, B Sa¨fsten, M Wagner, A Wanders, O Winqvist, M Carlson ............................................................................................................................... Gut 2005;54:1714–1720. doi: 10.1136/gut.2005.066423 Aim: The aim of this study was to establish a method of investigating intestinal eosinophil and neutrophil See end of article for granulocytes by flow cytometry, and to compare the distribution and activity of these cells in different authors’ affiliations stages of ulcerative colitis (UC). ....................... Methods: Biopsy samples were taken from six locations of the entire colon and from the terminal ileum in Correspondence to: 10 patients with active total UC, 10 patients with inactive total UC, eight patients with active distal UC, and Dr M Lampinen, 11 control subjects. Cell suspensions from biopsies and from peripheral blood were incubated with Department of Medical fluorophore conjugated monoclonal antibodies. The use of scatter plot-gating and specific antibodies was Sciences, Clinical Chemistry and Medicine, established in a flow cytometry assay. University Hospital, S-751 Results: Eosinophils were more numerous and more active in patients with active UC than in controls. 85 Uppsala, Sweden; Interestingly, during inactive UC, the number of activated eosinophils was even larger. Eosinophil activity maria.lampinen@ was high in the rectum of patients with distal colitis but was also slightly elevated in the proximal colon. medsci.uu.se Neutrophils were increased in number and activity during active but not inactive UC. -

How Are White Blood Cells Classified?
How are white blood cells classified? Copyright 2017 by the Rector and Visitors of the University of Virginia How are white blood cells classified? Types of White Blood Cells: Neutrophil Eosinophil Basophil Lymphocyte Monocyte . The types of white blood cells are shown above. The next page will describe lymphocytes in further detail. A healthy individual has all of these white blood cells types, but within specific ranges. Deviation from these ranges can indicate acute illness or a chronic disease. A mnemonic that is often used to remember the relative amount of each white blood cell that should be present is “Never Let Monkeys Eat Bananas.” Never Neutrophil Highest amounts Let Lymphocyte Monkeys Monocyte Eat Eosinophil Bananas Basophil Lowest amounts . In other words, neutrophils should always be present in higher amounts compared to the other cell types. This will be described further in “A first step in diagnosing LGL leukemia: The blood smear.” Copyright 2017 by the Rector and Visitors of the University of Virginia How are white blood cells classified? Introduction: White blood cells are blood cells that fight infection and disease. Lymphocytes are a type of white blood cell. They can identify antigens (substances foreign to the body) and cause an immune response. There are three types of lymphocytes: T-cell, NK-cell, and B-cell. In healthy adults, 10-15% of the lymphocytes are large granular lymphocytes (LGLs). To learn more about LGL cells, see “A first step in diagnosing LGL leukemia: The blood smear.” A person is diagnosed with LGL leukemia if there is a clonal (copied) population of T-cells or NK-cells present. -

The Role of Eosinophils in Parasitic Helminth Infections: Insights from Genetically Modified Mice C.A
Reviews The Role of Eosinophils in Parasitic Helminth Infections: Insights from Genetically Modified Mice C.A. Behm and K.S. Ovington Eosinophilia – an increase in the number of eosinophils in the it has been shown that IL-5, found at high levels in blood or tissues – has historically been recognized as a dis- helminth-infected hosts during the T-helper type 2 tinctive feature of helminth infections in mammals. Yet the (Th2) cytokine-biased immune response, appears to be precise functions of these cells are still poorly understood. important in mucosal immune responses and is re- Many scientists consider that their primary function is pro- sponsible for helminth-induced eosinophilia. IL-5 pre- tection against parasites, although there is little unequivocal sents quite a puzzle for immunologists. It has been in vivo evidence to prove this. Eosinophils are also respon- highly conserved during mammalian evolution – sible for considerable pathology in mammals because they are mouse IL-5, for example, has 71% amino acid identity inevitably present in large numbers in inflammatory lesions with human IL-5 – which suggests it has important associated with helminth infections or allergic conditions. In function(s) that have been selected during evolution. this review, Carolyn Behm and Karen Ovington outline some However, functions exclusive to IL-5 are not numer- of the cellular and biological properties of eosinophils and ous, and none appears to be essential for survival, at evaluate the evidence for their role(s) in parasitic infections. least for mice living in laboratory conditions. In mice, IL-5 controls or influences the development of two Eosinophils or ‘eosinophilic granulocytes’ normally major cell types: the elevated rate of development, mat- comprise only a small fraction (,1–5%) of circulating uration and survival of eosinophils during a Th2 cyto- leukocytes. -

Primary Blood and Immune Cells for Research
Primary blood and immune cells for research Lonza Walkersville, Inc. | © 2019 Agenda • Introduction and hematopoiesis • Products by tissue type • Tissue sources - overview • Applications • Donor variety • Support and resources Lonza Walkersville, Inc. | © 2019 2 Not every cell will work in your assay… Discover our expanded portfolio of blood and immune cells More than cells – support for wide ranging 01 Highest quality blood tissue and cells 05 workflows including transfection using Lonza’s Nucleofector™ Technology 02 Unmatched donor and cell variety 06 Global supply reach X-VIVO™ Serum-free Hematopoietic Cell Culture Full donor consent and IRB-approved collection 03 07 Media – with cell guarantee* facilities 04 World-class scientific support team 08 Certificate of Analysis, SDS in multiple languages * Lonza guarantees the performance of Clonetics™/Poietics™ Cells only if appropriate Clonetics™/Poietics™ Media and Reagents are used exclusively and the recommended storage and use protocols are followed. Any modifications made to the recommended cell systems including the use of alternative media, reagents or protocols, will void cell and media performance guarantees. If you need assistance in selecting the appropriate media, reagents, or protocol, please contact Lonza Scientific Support. Lonza Walkersville, Inc. | © 2019 3 The hematopoietic system From stem cells to T cells Stem Cell Lymphoid Progenitor Myeloid Progenitor Monocyte Basophil Eosinophil Neutrophil B cell T cell Natural Killer Dendritic Cell Macrophage Lonza Walkersville, Inc.