Gabapentin As an Antiepileptic Drug in Man
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
ANNNNNNNNNNNNNNNNNNNN 100A 006 Left Eye Input Right Eye Input
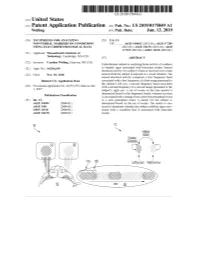
US 20190175049A1 ( 19) United States (12 ) Patent Application Publication (10 ) Pub. No. : US 2019 /0175049 A1 Welling ( 43 ) Pub . Date : Jun . 13 , 2019 ( 54 ) TECHNIQUES FOR ANALYZING (52 ) U . S . CI. NON -VERBAL MARKERS OF CONDITIONS CPC . .. A61B 5 /04842 (2013 . 01 ) ; A61B 5 / 7289 USING ELECTROPHYSIOLOGICAL DATA (2013 . 01) ; A61B 5 /0478 ( 2013 .01 ) ; A61B 5 /7225 ( 2013. 01 ) ; G06N 20 / 10 (2019 .01 ) (71 ) Applicant: Massachusetts Institute of Technology , Cambridge , MA (US ) ( 57 ) ABSTRACT (72 ) Inventor : Caroline Welling, Hanover, NH (US ) Embodiments related to analyzing brain activity of a subject to identify signs associated with binocular rivalry . Sensed ( 21 ) Appl. No. : 16 / 206, 639 electrical activity of a subject' s brain is received over a time period while the subject is exposed to a visual stimulus. The ( 22 ) Filed : Nov. 30 , 2018 sensed electrical activity comprises a first frequency band Related U . S . Application Data associated with a first frequency of a first image presented to the subject ' s left eye , a second frequency band associated (60 ) Provisional application No .62 / 593 , 535, filed on Dec . with a second frequency of a second image presented to the 1 , 2017 subject ' s right eye . A set of events in the time period is determined based on the frequency bands, wherein an event Publication Classification is associated with a change from a previous perceptual event (51 ) Int. Ci. to a new perceptual event. A metric for the subject is A61B 5 /0484 ( 2006 .01 ) determined based on the set of events . The metric is ana A61B 5 /00 ( 2006 .01 ) lyzed to determine whether the subject exhibits signs asso GO6N 20 / 10 (2006 .01 ) ciated with a condition that is associated with binocular A61B 5 /0478 ( 2006 .01 ) rivalry . -

(12) Patent Application Publication (10) Pub. No.: US 2006/0110428A1 De Juan Et Al
US 200601 10428A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2006/0110428A1 de Juan et al. (43) Pub. Date: May 25, 2006 (54) METHODS AND DEVICES FOR THE Publication Classification TREATMENT OF OCULAR CONDITIONS (51) Int. Cl. (76) Inventors: Eugene de Juan, LaCanada, CA (US); A6F 2/00 (2006.01) Signe E. Varner, Los Angeles, CA (52) U.S. Cl. .............................................................. 424/427 (US); Laurie R. Lawin, New Brighton, MN (US) (57) ABSTRACT Correspondence Address: Featured is a method for instilling one or more bioactive SCOTT PRIBNOW agents into ocular tissue within an eye of a patient for the Kagan Binder, PLLC treatment of an ocular condition, the method comprising Suite 200 concurrently using at least two of the following bioactive 221 Main Street North agent delivery methods (A)-(C): Stillwater, MN 55082 (US) (A) implanting a Sustained release delivery device com (21) Appl. No.: 11/175,850 prising one or more bioactive agents in a posterior region of the eye so that it delivers the one or more (22) Filed: Jul. 5, 2005 bioactive agents into the vitreous humor of the eye; (B) instilling (e.g., injecting or implanting) one or more Related U.S. Application Data bioactive agents Subretinally; and (60) Provisional application No. 60/585,236, filed on Jul. (C) instilling (e.g., injecting or delivering by ocular ion 2, 2004. Provisional application No. 60/669,701, filed tophoresis) one or more bioactive agents into the Vit on Apr. 8, 2005. reous humor of the eye. Patent Application Publication May 25, 2006 Sheet 1 of 22 US 2006/0110428A1 R 2 2 C.6 Fig. -

Calcium Channel Blocker As a Drug Candidate for the Treatment of Generalised Epilepsies
UNIVERSITAT DE BARCELONA Faculty of Pharmacy and Food Sciences Calcium channel blocker as a drug candidate for the treatment of generalised epilepsies Final degree project Author: Janire Sanz Sevilla Bachelor's degree in Pharmacy Primary field: Organic Chemistry, Pharmacology and Therapeutics Secondary field: Physiology, Pathophysiology and Molecular Biology March 2019 This work is licensed under a Creative Commons license ABBREVIATIONS AED antiepileptic drug AMPA α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid ANNA-1 antineuronal nuclear antibody 1 BBB blood-brain barrier Bn benzyl BnBr benzyl bromide BnNCO benzyl isocyanate Boc tert-butoxycarbonyl Bu4NBr tetrabutylammonium bromide Ca+2 calcium ion CACNA1 calcium channel voltage-dependent gene cAMP cyclic adenosine monophosphate CCB calcium channel blocker cGMP cyclic guanosine monophosphate CH3CN acetonitrile Cl- chlorine ion Cmax maximum concentration CMV cytomegalovirus CTScan computed axial tomography DCM dichloromethane DIPEA N,N-diisopropylethylamine DMF dimethylformamide DMPK drug metabolism and pharmacokinetics DNET dysembryoplastic neuroepithelial tumours EEG electroencephalogram EPSP excitatory post-synaptic potential FDA food and drug administration Fe iron FLIPR fluorescence imaging plate reader fMRI functional magnetic resonance imaging GABA γ-amino-α-hydroxybutyric acid GAD65 glutamic acid decarboxylase 65 GAERS generalised absence epilepsy rat of Strasbourg GluR5 kainate receptor GTC generalised tonic-clonic H+ hydrogen ion H2 hydrogen H2O dihydrogen dioxide (water) -

A Comparative Study of Progabide, Valproate, and Epilepsy
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.49.11.1251 on 1 November 1986. Downloaded from Journal of Neurology, Neurosurgery, and Psychiatry 1986;49:1251-1257 A comparative study of progabide, valproate, and placebo as add-on therapy in patients with refractory epilepsy P CRAWFORD, D CHADWICK From the Department ofNeurology, Walton Hospital, Liverpool, UK SUMMARY A three way single blind cross-over comparison of progabide, valproate and placebo, as adjunctive therapy, was undertaken in 64 patients with therapy-resistant partial and generalised seizures. The study was not completed because of the incidence of elevated hepatic enzymes on progabide. Analysis of efficacy showed progabide to be inferior to valproate against all seizure types, particularly against tonic-clonic seizures. Valproate was superior to placebo against all seizure types, partial and tonic-clonic seizures. Progabide did not differ significantly from placebo in any instance. In addition progabide caused elevation of hepatic enzymes which was symptomatic in one case, and was associated with an interaction with phenytoin symptoms which resulted in of guest. Protected by copyright. intoxication in some cases. Progabide is a pro-drug and a GABA agonist which treatment limb was of six months with a two week washout possesses anticonvulsant properties in a variety of and cross-over period between treatment phases. Patients experimental models of seizures and epilepsy.' with severe, partial or generalised epilepsies were eligible for Whether it possesses antiepileptic properties in man is admission to the study as long as they had a definite history controversial. A number of double blind of epilepsy confirmed by observation and EEG recording studies and suffered a minimum of one seizure per month during the against placebo have been reported, some of which six months prior to entry into the study. -

Late Shri Vishnu Waman Thakur Charitable Trust`S VIVA INSTITUTE of PHARMACY At: Shirgaon, Veer Sawarkar Road, Virar (E), Taluka: Vasai, Dist
Late Shri Vishnu Waman Thakur Charitable Trust`s VIVA INSTITUTE OF PHARMACY At: Shirgaon, Veer Sawarkar Road, Virar (E), Taluka: Vasai, Dist. Palghar-401305, Maharashtra. FINAL YEAR UNIVERSITY EXAMINATION 2019-2020 Final Year B.Pharm. Semester VIII SUBJECT-BPH_C_801_T-Pharmaceutical Chemistry III MULTIPLE CHOICE QUESTIONS: PRACTICE QUESTION BANK Q. 1 Which is the correct IUPAC name for the following structure? A] 5-chloro-2-(methylamino)-5-phenyl-3H-1,4-benzodiazepine B] 7-chloro-2-(methylamino)-5-pyridinyl-3H-1,4-benzodiazepine-4-oxide C] 7-chloro-2-(ethylamino)-5-phenyl-3H-1,5-benzodiazepine D] 7-chloro-2-(methylamino)-5-phenyl-3H-1,4-benzodiazepine-4-oxide Q. 2 Which of the following is long acting sedative hypnotic? A] Diazepam B] Alprazolam C] Temazepam D] Imipramine Q. 3 Name of oxide derivative used as sedative hypnotic is A] Diazepam B] Chlordiazepoxide C] Nitazepam D] Ramelteon Late Shri Vishnu Waman Thakur Charitable Trust`s VIVA INSTITUTE OF PHARMACY At: Shirgaon, Veer Sawarkar Road, Virar (E), Taluka: Vasai, Dist. Palghar-401305, Maharashtra. Q. 4 With respect to the following general structure which is the correct statement ? A] X must be electropositive substituent for optimum activity B] X must be aromatic ring for optimum activity C] X must be electronegative substituent for optimum activity D] X must be H for optimum activity Q. 5 Which is the incorrect statement with respect to structure given in Q. 4 A] Ring C is ortho substituted with electron withdrawing group for optimum activity B] Ring C when para substituted increases activity C] Ring C is diortho substituted with electron withdrawing group for optimum activity D] Ring C when para substituted decreases activity Q. -

85 Mv Respectively. When the Membranewas Depolarized, Th
J. Physiol. (1985), 360, pp. 161-185 161 With 14 text-figurem Printed in Great Britain COMPARISON OF THE ACTION OF BACLOFEN WITH y-AMINOBUTYRIC ACID ON RAT HIPPOCAMPAL PYRAMIDAL CELLS IN VITRO BY N. R. NEWBERRY* AND R. A. NICOLLt From the Departments of Pharmacology and Physiology, University of California, San Francisco, CA 94143, U.S.A. (Received 13 June 1984) SUMMARY 1. Intracellular recordings from CAI pyramidal cells in the hippocampal slice preparation were used to compare the action of baclofen, a y-aminobutyric acid (GABA) analogue, with GABA. 2. Ionophoretic application of GABA or baclofen into stratum (s.) pyramidale evoked hyperpolarizations associated with reductions in the input resistance of the cell. Baclofen responses were easier to elicit in the dendrites than in the cell body layer. 3. Blockade of synaptic transmission, with tetrodotoxin or cadmium, did not reduce baclofen responses, indicating a direct post-synaptic action. 4. (+ )-Bicuculline (10 ,UM) and bicuculline methiodide (100 /SM) had little effect on baclofen responses but strongly antagonized somatic GABA responses of equal amplitude. The bicuculline resistance of the baclofen response was not absolute, as higher concentrations of these compounds did reduce it. Pentobarbitone (100 /M) enhanced somatic GABA responses without affecting baclofen responses. (-)-Baclofen was approximately 200 times more potent than (+ )-baclofen. 5. The reversal potentials for the somatic GABA and baclofen responses were -70 mV and -85 mV respectively. When the membrane was depolarized, the baclofen response was reduced. This apparent voltage sensitivity was not seen with somatic GABA responses. 6. Altering the chloride gradient across the cell membrane altered the reversal potential of the somatic GABA response but not that ofthe baclofen response. -

Pharmaceutical Chemistry III MULTIPLE CHOICE QUESTIONS: PRACTICE QUESTION BANK
FINAL YEAR UNIVERSITY EXAMINATION 2019-2020 Final Year B.Pharm. Semester VIII SUBJECT-BPH_C_801_T-Pharmaceutical Chemistry III MULTIPLE CHOICE QUESTIONS: PRACTICE QUESTION BANK SET-I Q. 1 Which is the correct IUPAC name for the following structure? A] 5-chloro-2-(methylamino)-5-phenyl-3H-1,4-benzodiazepine B] 7-chloro-2-(methylamino)-5-pyridinyl-3H-1,4-benzodiazepine-4-oxide C] 7-chloro-2-(ethylamino)-5-phenyl-3H-1,5-benzodiazepine D] 7-chloro-2-(methylamino)-5-phenyl-3H-1,4-benzodiazepine-4-oxide Q. 2 Which of the following is long acting sedative hypnotic? A] Diazepam B] Alprazolam C] Temazepam D] Imipramine Q. 3 Name of oxide derivative used as sedative hypnotic is A] Diazepam B] Chlordiazepoxide C]Nitazepam D] Ramelteon Q. 4 With respect to the following general structure which is the correctstatement ? A] X must be electropositive substituent for optimum activity B] X must be aromatic ring for optimum activity C] X must be electronegative substituent for optimum activity D] X must be H for optimum activity Q. 5 Which is the incorrect statement with respect to structure given in Q. 4 A] Ring C is ortho substituted with electron withdrawing group for optimum activity B] Ring C when para substituted increases activity C] Ring C is diortho substituted with electron withdrawing group for optimum activity D] Ring C when para substituted decreases activity Q. 6 What is the starting material for synthesis of Piroxicam (structure given below) A] B] C] D] Q. 7 Which one of the following is Cytokine inhibitor? A] Abatacept B] Fluoxetine C] Propranolol D]Aldosterone Q. -

Assessment of Molecular Action of Direct Gating and Allosteric Modulatory Effects of Carisoprodol (Somartm) on GABA a Receptors
Graduate Theses, Dissertations, and Problem Reports 2015 Assessment of molecular action of direct gating and allosteric modulatory effects of carisoprodol (SomaRTM) on GABA A receptors Manoj Kumar Follow this and additional works at: https://researchrepository.wvu.edu/etd Recommended Citation Kumar, Manoj, "Assessment of molecular action of direct gating and allosteric modulatory effects of carisoprodol (SomaRTM) on GABA A receptors" (2015). Graduate Theses, Dissertations, and Problem Reports. 6022. https://researchrepository.wvu.edu/etd/6022 This Dissertation is protected by copyright and/or related rights. It has been brought to you by the The Research Repository @ WVU with permission from the rights-holder(s). You are free to use this Dissertation in any way that is permitted by the copyright and related rights legislation that applies to your use. For other uses you must obtain permission from the rights-holder(s) directly, unless additional rights are indicated by a Creative Commons license in the record and/ or on the work itself. This Dissertation has been accepted for inclusion in WVU Graduate Theses, Dissertations, and Problem Reports collection by an authorized administrator of The Research Repository @ WVU. For more information, please contact [email protected]. ASSESSMENT OF MOLECULAR ACTION OF DIRECT GATING AND ALLOSTERIC MODULATORY EFFECTS OF MEPROBAMATE (MILTOWN®) ON GABAA RECEPTORS Manish Kumar, MD, MS Dissertation submitted to the School of Pharmacy at West Virginia University in partial fulfillment of Requirements -

Pregabalin Abuse: a Case Report Ilhan Yargic1, Filiz Alyanak Ozdemiroglu2
Olgu Sunumları / Case Reports DOI: 10.5350/KPB-BCP201121110 Pregabalin Abuse: A Case Report Ilhan Yargic1, Filiz Alyanak Ozdemiroglu2 ÖZET: ABS TRACT: Pregabalin kötüye kullanımı: Bir olgu sunumu Pregabalin abuse: a case report Pregabalin epilepsi, nöropatik ağrı ve yaygın anksiyete Pregabalin is a gamma-amino butyric acid (GABA) analogue bozukluğunun tedavilerinde kullanılan bir gama-aminobu- used in the treatment of epilepsy, neuropathic pain, and tirik asit (GABA) analoğudur. Pregabalin Türkiye’de kontrole generalized anxiety disorder. Although pregabalin is not tabi ilaçlardan olmamasına karşın kötüye kullanılma potan- a controlled medication in Turkey, it has a potential risk 1M.D., Professor of Psychiatry, Istanbul siyeline sahiptir. Türkiye’de yaygın anksiteye bozukluğu gibi of abuse. It has not been approved for the treatment of University, Istanbul Faculty of Medicine, Psychiatry Department, Istanbul-Turkey psikiyatrik hastalıkların tedavisi için ruhsatlandırılmış olma- psychiatric disorders (such as generalized anxiety disorder) 2M.D., Istinye Devlet Hastanesi, Psikiyatri AD, dığı için henüz psikiyatri hastaları arasında popüler değildir. in Turkey, so it is not yet popular as a drug of abuse among Istinye, Istanbul-Turkey 37 yaşında, bipolar bozukluğu ve benzodiyazepin kötüye psychiatric patients. We report the first case of pregabalin Ya zış ma Ad re si / Add ress rep rint re qu ests to: kullanımı öyküsü olan bir erkek hastada Türkiye’den ilk pre- abuse in Turkey in a 37 year old male patient who has a İlhan Yargıç, M.D., Istanbul -

Gamma-Aminobutyric Acid (GABA) Is a Major NeuroTransmitter Widely Distributed Throughout the Central Nervous System (CNS)
Alternative Medicine Review Volume 12, Number 3 2007 Monograph GABA Gamma-Aminobutyric O + Acid (GABA) H3N O- Introduction Gamma-aminobutyric acid (GABA) is a major neuro transmitter widely distributed throughout the central nervous system (CNS). Because too much excitation can lead to irritability, restlessness, insomnia, seizures, and movement disorders, it must be balanced with inhibition. GABA – the most important inhibitory neurotransmitter in the brain – provides this inhibition, acting like a “brake” during times of runaway stress. Medications for anxiety, such as benzodiazepines, stimulate GABA receptors and induce relaxation. Either low GABA levels or decreased GABA function in the brain is associated with several psy- chiatric and neurological disorders, including anxiety, depression, insomnia, and epilepsy. Studies indicate GABA can improve relaxation and enhance sleep. Both synthetic and natural GABA are available as dietary supplements in the United States. Natural GABA is produced via a fermentation process that utilizes Lactobacillus hilgardii – the bacteria used to ferment vegetables in the preparation of the traditional Korean dish known as kimchi. Biochemistry and Pharmacokinetics Within the brain, glutamic acid is converted to GABA via the enzyme glutamate decarboxylase and its cofac- tor pyridoxal 5’ phosphate (P5P; active vitamin B6). GABA is metabolized by gamma-aminobutyrate transaminase, also a P5P-dependent enzyme, forming an intermediate metabolite succinate semialdehyde. This metabolite can then be reduced to gamma-hydroxybutyrate, or oxidized to succinate and eventually converted to CO2 and water via the citric acid cycle. When plasma membrane depolarization induces the release of GABA from nerve terminals, GABA binds to GABA receptors – such as the GABAA and GABAB receptors – that are distributed on post-synaptic cell membranes. -

Pharmaceuticals As Environmental Contaminants
PharmaceuticalsPharmaceuticals asas EnvironmentalEnvironmental Contaminants:Contaminants: anan OverviewOverview ofof thethe ScienceScience Christian G. Daughton, Ph.D. Chief, Environmental Chemistry Branch Environmental Sciences Division National Exposure Research Laboratory Office of Research and Development Environmental Protection Agency Las Vegas, Nevada 89119 [email protected] Office of Research and Development National Exposure Research Laboratory, Environmental Sciences Division, Las Vegas, Nevada Why and how do drugs contaminate the environment? What might it all mean? How do we prevent it? Office of Research and Development National Exposure Research Laboratory, Environmental Sciences Division, Las Vegas, Nevada This talk presents only a cursory overview of some of the many science issues surrounding the topic of pharmaceuticals as environmental contaminants Office of Research and Development National Exposure Research Laboratory, Environmental Sciences Division, Las Vegas, Nevada A Clarification We sometimes loosely (but incorrectly) refer to drugs, medicines, medications, or pharmaceuticals as being the substances that contaminant the environment. The actual environmental contaminants, however, are the active pharmaceutical ingredients – APIs. These terms are all often used interchangeably Office of Research and Development National Exposure Research Laboratory, Environmental Sciences Division, Las Vegas, Nevada Office of Research and Development Available: http://www.epa.gov/nerlesd1/chemistry/pharma/image/drawing.pdfNational -

Marrakesh Agreement Establishing the World Trade Organization
No. 31874 Multilateral Marrakesh Agreement establishing the World Trade Organ ization (with final act, annexes and protocol). Concluded at Marrakesh on 15 April 1994 Authentic texts: English, French and Spanish. Registered by the Director-General of the World Trade Organization, acting on behalf of the Parties, on 1 June 1995. Multilat ral Accord de Marrakech instituant l©Organisation mondiale du commerce (avec acte final, annexes et protocole). Conclu Marrakech le 15 avril 1994 Textes authentiques : anglais, français et espagnol. Enregistré par le Directeur général de l'Organisation mondiale du com merce, agissant au nom des Parties, le 1er juin 1995. Vol. 1867, 1-31874 4_________United Nations — Treaty Series • Nations Unies — Recueil des Traités 1995 Table of contents Table des matières Indice [Volume 1867] FINAL ACT EMBODYING THE RESULTS OF THE URUGUAY ROUND OF MULTILATERAL TRADE NEGOTIATIONS ACTE FINAL REPRENANT LES RESULTATS DES NEGOCIATIONS COMMERCIALES MULTILATERALES DU CYCLE D©URUGUAY ACTA FINAL EN QUE SE INCORPOR N LOS RESULTADOS DE LA RONDA URUGUAY DE NEGOCIACIONES COMERCIALES MULTILATERALES SIGNATURES - SIGNATURES - FIRMAS MINISTERIAL DECISIONS, DECLARATIONS AND UNDERSTANDING DECISIONS, DECLARATIONS ET MEMORANDUM D©ACCORD MINISTERIELS DECISIONES, DECLARACIONES Y ENTEND MIENTO MINISTERIALES MARRAKESH AGREEMENT ESTABLISHING THE WORLD TRADE ORGANIZATION ACCORD DE MARRAKECH INSTITUANT L©ORGANISATION MONDIALE DU COMMERCE ACUERDO DE MARRAKECH POR EL QUE SE ESTABLECE LA ORGANIZACI N MUND1AL DEL COMERCIO ANNEX 1 ANNEXE 1 ANEXO 1 ANNEX