Non-Inflammatory Arthritis Non-Inflammatory Arthritis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Olecranon Bursitis
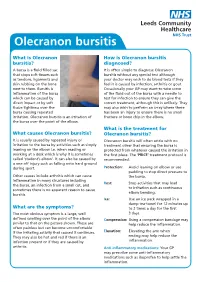
Olecranon bursitis What is Olecranon How is Olecranon bursitis bursitis? diagnosed? A bursa is a fluid filled sac It is often simple to diagnose Olecranon that stops soft tissues such bursitis without any special test although as tendons, ligaments and your doctor may wish to do blood tests if they skin rubbing on the bone feel it is caused by infection, arthritis or gout. next to them. Bursitis is Occasionally your GP may want to take some inflammation of the bursa of the fluid out of the bursa with a needle to which can be caused by test for infection to ensure they can give the direct impact or by soft correct treatment, although this is unlikely. They tissue tightness over the may also wish to perform an x-ray where there bursa causing repeated has been an injury to ensure there is no small irritation. Olecranon bursitis is an irritation of fracture or bone chip in the elbow. the bursa over the point of the elbow. What is the treatment for What causes Olecranon bursitis? Olecranon bursitis? It is usually caused by repeated injury or Olecranon bursitis will often settle with no irritation to the bursa by activities such as simply treatment other that ensuring the bursa is leaning on the elbow i.e. when reading or protected from whatever caused the irritation in working at a desk which is why it is sometimes the first place. The ‘PRICE’ treatment protocol is called ‘student’s elbow’. It can also be caused by recommended: a one off injury such as falling onto hard ground during sport. -

OES Site Color Scheme 1
Nuisance Problems You will Grow to Love Thomas V Gocke, MS, ATC, PA-C, DFAAPA President & Founder Orthopaedic Educational Services, Inc. Boone, NC [email protected] www.orthoedu.com Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. all rights reserved. Faculty Disclosures • Orthopaedic Educational Services, Inc. Financial Intellectual Property No off label product discussions American Academy of Physician Assistants Financial PA Course Director, PA’s Guide to the MSK Galaxy Urgent Care Association of America Financial Intellectual Property Faculty, MSK Workshops Ferring Pharmaceuticals Consultant Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. all rights reserved. 2 LEARNING GOALS At the end of this sessions you will be able to: • Recognize nuisance conditions in the Upper Extremity • Recognize nuisance conditions in the Lower Extremity • Recognize common Pediatric Musculoskeletal nuisance problems • Recognize Radiographic changes associates with common MSK nuisance problems • Initiate treatment plans for a variety of MSK nuisance conditions Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. all rights reserved. Inflammatory Response Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. all rights reserved. Inflammatory Response* When does the Inflammatory response occur: • occurs when injury/infection triggers a non-specific immune response • causes proliferation of leukocytes and increase in blood flow secondary to trauma • increased blood flow brings polymorph-nuclear leukocytes (which facilitate removal of the injured cells/tissues), macrophages, and plasma proteins to injured tissues *Knight KL, Pain and Pain relief during Cryotherapy: Cryotherapy: Theory, Technique and Physiology, 1st edition, Chattanooga Corporation, Chattanooga, TN 1985, p 127-137 Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. -

Sports Medicine Examination Outline
Sports Medicine Examination Content I. ROLE OF THE TEAM PHYSICIAN 1% A. Ethics B. Medical-Legal 1. Physician responsibility 2. Physician liability 3. Preparticipation clearance 4. Return to play 5. Waiver of liability C. Administrative Responsibilities II. BASIC SCIENCE OF SPORTS 16% A. Exercise Physiology 1. Training Response/Physical Conditioning a.Aerobic b. Anaerobic c. Resistance d. Flexibility 2. Environmental a. Heat b.Cold c. Altitude d.Recreational diving (scuba) 3. Muscle a. Contraction b. Lactate kinetics c. Delayed onset muscle soreness d. Fiber types 4. Neuroendocrine 5. Respiratory 6. Circulatory 7. Special populations a. Children b. Elderly c. Athletes with chronic disease d. Disabled athletes B. Anatomy 1. Head/Neck a.Bone b. Soft tissue c. Innervation d. Vascular 2. Chest/Abdomen a.Bone b. Soft tissue c. Innervation d. Vascular 3. Back a.Bone b. Soft tissue c. Innervation 1 d. Vascular 4. Shoulder/Upper arm a. Bone b. Soft tissue c. Innervation d. Vascular 5. Elbow/Forearm a. Bone b. Soft tissue c. Innervation d. Vascular 6. Hand/Wrist a. Bone b. Soft tissue c. Innervation d. Vascular 7. Hip/Pelvis/Thigh a. Bone b. Soft tissue c. Innervation d. Vascular 8. Knee a. Bone b. Soft tissue c. Innervation d. Vascular 9. Lower Leg/Foot/Ankle a. Bone b. Soft tissue c. Innervation d. Vascular 10. Immature Skeleton a. Physes b. Apophyses C. Biomechanics 1. Throwing/Overhead activities 2. Swimming 3. Gait/Running 4. Cycling 5. Jumping activities 6. Joint kinematics D. Pharmacology 1. Therapeutic Drugs a. Analgesics b. Antibiotics c. Antidiabetic agents d. Antihypertensives e. -

Acute < 6 Weeks Subacute ~ 6 Weeks Chronic >
Pain Articular Non-articular Localized Generalized . Regional Pain Disorders . Myalgias without Weakness Soft Tissue Rheumatism (ex., fibromyalgia, polymyalgia (ex., soft tissue rheumatism rheumatica) tendonitis, tenosynovitis, bursitis, fasciitis) . Myalgia with Weakness (ex., Inflammatory muscle disease) Clinical Features of Arthritis Monoarthritis Oligoarthritis Polyarthritis (one joint) (two to five joints) (> five joints) Acute < 6 weeks Subacute ~ 6 weeks Chronic > 6 weeks Inflammatory Noninflammatory Differential Diagnosis of Arthritis Differential Diagnosis of Arthritis Acute Monarthritis Acute Polyarthritis Inflammatory Inflammatory . Infection . Viral - gonococcal (GC) - hepatitis - nonGC - parvovirus . Crystal deposition - HIV - gout . Rheumatic fever - calcium . GC - pyrophosphate dihydrate (CPPD) . CTD (connective tissue diseases) - hydroxylapatite (HA) - RA . Spondyloarthropathies - systemic lupus erythematosus (SLE) - reactive . Sarcoidosis - psoriatic . - inflammatory bowel disease (IBD) Spondyloarthropathies - reactive - Reiters . - psoriatic Early RA - IBD - Reiters Non-inflammatory . Subacute bacterial endocarditis (SBE) . Trauma . Hemophilia Non-inflammatory . Avascular Necrosis . Hypertrophic osteoarthropathy . Internal derangement Chronic Monarthritis Chronic Polyarthritis Inflammatory Inflammatory . Chronic Infection . Bony erosions - fungal, - RA/Juvenile rheumatoid arthritis (JRA ) - tuberculosis (TB) - Crystal deposition . Rheumatoid arthritis (RA) - Infection (15%) - Erosive OA (rare) Non-inflammatory - Spondyloarthropathies -

Variation in the Initial Treatment of Knee Monoarthritis in Juvenile Idiopathic Arthritis: a Survey of Pediatric Rheumatologists in the United States and Canada
Variation in the Initial Treatment of Knee Monoarthritis in Juvenile Idiopathic Arthritis: A Survey of Pediatric Rheumatologists in the United States and Canada TIMOTHY BEUKELMAN, JAMES P. GUEVARA, DANIEL A. ALBERT, DAVID D. SHERRY, and JON M. BURNHAM ABSTRACT. Objective. To characterize variations in initial treatment for knee monoarthritis in the oligoarthritis sub- type of juvenile idiopathic arthritis (OJIA) by pediatric rheumatologists and to identify patient, physi- cian, and practice-specific characteristics that are associated with treatment decisions. Methods. We mailed a 32-item questionnaire to pediatric rheumatologists in the United States and Canada (n = 201). This questionnaire contained clinical vignettes describing recent-onset chronic monoarthritis of the knee and assessed physicians’ treatment preferences, perceptions of the effective- ness and disadvantages of nonsteroidal antiinflammatory drugs (NSAID) and intraarticular corticos- teroid injections (IACI), proficiency with IACI, and demographic and office characteristics. Results. One hundred twenty-nine (64%) questionnaires were completed and returned. Eighty-three per- cent of respondents were board certified pediatric rheumatologists. Respondents’ treatment strategies for uncomplicated knee monoarthritis were broadly categorized: initial IACI at presentation (27%), initial NSAID with contingent IACI (63%), and initial NSAID with contingent methotrexate or sulfasalazine (without IACI) (10%). Significant independent predictors for initial IACI were believing that IACI is more effective than NSAID, having performed > 10 IACI in a single patient at one time, and initiating methotrexate via the subcutaneous route for OJIA. Predictors for not recommending initial or contin- gent IACI were believing that the infection risk of IACI is significant and lacking comfort with per- forming IACI. Conclusion. There is considerable variation in pediatric rheumatologists’ initial treatment strategies for knee monoarthritis in OJIA. -

Bilateral Calcified Ischiogluteal Bursitis and Shoulder Tendinopathy
Bilateral Calcified Ischiogluteal Bursitis and Conflict of Interest: None Shoulder Tendinopathy: A Case Report declared Seyyed-Mohsen Hosseininejad1,2, Saman Shakeri1, Hossein Mohebbi1, Mehdi Aarabi2, Shiva Momen3 This article has been peer reviewed. 1Shahid Beheshti University of Medical Sciences, Tehran, Iran 2 Golestan University of Medical Sciences, Gorgan, Iran Article Submitted on: 21st 3Mazandaran University of Medical Sciences, Sari, Iran January 2019 Article Accepted on: 1st ABSTRACT June 2020 The ischiogluteal bursitis which is a rare the buttock. Ischiogluteal bursitis Aspiration Funding Sources: None disorder is irregularly found between the showed calcareous deposits; local injection declared gluteus maximus and ischial tuberosity. A of corticosteroid helped the patient to get 41-year-old female with bilateral calcifying free of symptoms. Calcified ischiogluteal Correspondence to: Dr ischiogluteal bursitis and her right shoulder bursitis is a rare condition but simply Seyyed-Mohsen Hosseininejad tendinopathy were presented. She had no diagnosed on x-ray. Local steroid injection related past medical history nor trauma to could provide symptom relief. Address: Shahid Beheshti University of Medical Sciences, Tehran, Iran Keywords: Calcifying Ischiogluteal Bursitis; Aspiration; Treatment; Shoulder pain; Tendinopathy E-mail: Hosseininejad.s.mohsen INTRODUCTION painful swelling in her both buttocks. The patient @gmail.com Ischiogluteal bursitis is a rare condition in which had no related past medical history nor recent Cite this Article: bursa between the gluteus maximus muscle and major trauma. Ischial tuberosities had swelling Hosseininejad SM, ischial tuberosity, which physiologically and tenderness in. Right shoulder had positive Shakeri S, Mohebbi H, decreases the frictional force, develops impingement tests but full range of motion. Aarabi M, Momen S. -

Endoscopic Hamstring Repair
Lorem Ipsum Endoscopic Hamstring Repair Carlos A. Guanche, MD Southern California Orthopedic Institute 12 Lorem Ipsum 2 Endoscopic Hamstring Repair With the expansion of knowledge regarding hip pathologies as a result of the increased treatment of hip problems arthroscopically has come an expanded treatment of many injuries that were previously treated through open methods. The treatment of symptomatic ischial bursitis and hamstring injuries is one such area. In this paper, the author describes the surgical procedure and discusses the findings and preliminary outcomes in a group of the first 15 patients undergoing the procedure. The clinical rationale associated with the treatment algorithm is also discussed. Hamstring injuries have been effectively addressed in the past with a variety of open methods.(1,2) However, the endoscopic management of much pathology previously treated with more invasive, open approaches has evolved. The technique described in this chapter is another such evolution. Hamstring injuries are common and can affect all levels of The hamstrings originate from the ischial tuberosity and athletes. (3-7) There is a continuum of hamstring injuries insert distally below the knee on the proximal tibia, with the that can range from musculotendinous strains to avulsion exception of the short head of the biceps femoris. The tibial injuries. (3,4) Most hamstring strains do not require surgical branch of the sciatic nerve innervates the semitendinosus, intervention and resolve with a variety of modalities and semimembranosus, and the peroneal branch of the sciatic rest. (3-7) In some patients, chronic pain can occur at the nerve innervates the long head of the biceps femoris.(5) hamstring origin from either partial or complete tears as well as from chronic ischial bursitis. -

Concurrent Onset of Adult Onset Still's Disease and Insulin Dependent Diabetes Mellitus
Annals ofthe Rheumatic Diseases 1990; 49: 547-548 547 Concurrent onset of adult onset Still's disease and Ann Rheum Dis: first published as 10.1136/ard.49.7.547 on 1 July 1990. Downloaded from insulin dependent diabetes mellitus J T Sibley Abstract time, partial thromboplastin time, C3, C4, Clq Within two weeks after symptoms of an upper binding, tri-iodothyronine, thyroxine, serum respiratory tract infection a 32 year old man amylase, serum protein electrophoresis, and developed Still's disease and insulin dependent gallium scan. diabetes mellitus, both ofwhich have persisted Initial and convalescent serum rubella titres for 24 months. Investigations failed to confirm (haemagglutination inhibition) were both 1/640. acute infection but did show isolated persistent Hepatic transaminases were five times normal. increase of serum antibodies to rubelia virus. Abdominal ultrasound confirmed splenomegaly The simultaneous onset of these two diseases and showed decreased echogenicity of the suggests a shared cause, possibly associated pancreas. An abdominal computed tomography with rubella infection. scan was normal except for hepatosplenomegaly. Percutaneous liver biopsy showed only minor focal portal tract inflammation. A two dimen- Adult onset Still's disease is an uncommon sional echocardiogram showed a small peri- entity characterised by a multisystem illness cardial effusion. HLA typing results were with a wide constellation of features, notably A2,-;B44,5 1 ;Cw2,-;DR1,7. fever, rash, and arthritis.' Its cause is unknown, The diagnosis of adult onset Still's disease though there are a few reports of association was based on the typical clinical features, with viral illness.2A Insulin dependent diabetes including the characteristic evanescent rash and mellitus is also thought in some cases to have a daily fever in the absence ofclinical or laboratory viral cause,5 but I am unaware of any reports of confirmation of other diagnostic possibilities.' 6 the simultaneous onset of these two diseases. -

Pediatric MSK Protocols
UT Southwestern Department of Radiology Ankle and Foot Protocols - Last Update 5-18-2015 Protocol Indications Notes Axial Coronal Sagittal Ankle / Midfoot - Routine Ankle Pain Axial = In Relation to Leg "Footprint" (Long Axis to Foot) T1 FSE PD SPAIR T1 FSE Injury, Internal Derangement Coronal = In Relation to Leg (Short Axis Foot) PD SPAIR STIR Talar OCD, Coalition Protocol Indications Notes Axial Coronal Sagittal Ankle / Midfoot - Arthritis Arthritis Axial = In Relation to Leg "Footprint" (Long Axis to Foot) PD SPAIR PD SPAIR T1 FSE Coronal = In Relation to Leg (Short Axis Foot) STIR T1 SPIR POST T1 SPIR POST Protocol Indications Notes Axial Coronal Sagittal Foot - Routine Pain, AVN Axial = In Relation to Leg "Footprint" (Long Axis to Foot) T1 FSE PD FSE T1 FSE Coronal = In Relation to Leg (Short Axis Foot) PD SPAIR PD SPAIR STIR Protocol Indications Notes Axial Coronal Sagittal Foot - Arthritis Arthritis Axial = In Relation to Leg "Footprint" (Long Axis to Foot) T1 FSE PD SPAIR STIR Coronal = In Relation to Leg (Short Axis Foot) PD SPAIR T1 SPIR POST 3D WATS T1 SPIR POST Protocol Indications Notes Axial Coronal Sagittal Great Toe / MTP Joints Turf Toe Smallest Coil Possible (Microcoil if Available) PD FSE T1 FSE PD FSE Sesamoiditis FoV = Mid Metatarsal Through Distal Phalanges PD SPAIR PD SPAIR PD SPAIR Slice thickness = 2-3 mm, 10% gap Axial = In relation to the great toe (short axis foot) Coronal = In relation to the great toe (long axis foot / footprint) Appropriate Coronal Plane for Both Ankle and Foot Imaging UT Southwestern Department -

Biological Treatment in Resistant Adult-Onset Still's Disease: a Single-Center, Retrospective Cohort Study
Arch Rheumatol 2021;36(x):i-viii doi: 10.46497/ArchRheumatol.2021.8669 ORIGINAL ARTICLE Biological treatment in resistant adult-onset Still’s disease: A single-center, retrospective cohort study Seda Çolak, Emre Tekgöz, Maghrur Mammadov, Muhammet Çınar, Sedat Yılmaz Department of Internal Medicine, Division of Rheumatology, Gülhane Training and Research Hospital, Ankara, Turkey ABSTRACT Objectives: The aim of this study was to assess the demographic and clinical characteristics of patients with adult-onset Still’s disease (AOSD) under biological treatment. Patients and methods: This retrospective cohort study included a total of 19 AOSD patients (13 males, 6 females; median age: 37 years; range, 28 to 52 years) who received biological drugs due to refractory disease between January 2008 and January 2020. The data of the patients were obtained from the patient files. The response to the treatment was evaluated based on clinical and laboratory assessments at third and sixth follow-up visits. Results: Interleukin (IL)-1 inhibitor was prescribed for 13 (68.4%) patients and IL-6 inhibitor prescribed for six (31.6%) patients. Seventeen (89.5%) patients experienced clinical remission. Conclusion: Biological drugs seem to be effective for AOSD patients who are resistant to conventional therapies. Due to the administration methods and the high costs of these drugs, however, tapering the treatment should be considered, after remission is achieved. Keywords: Adult-onset Still’s disease, anakinra, tocilizumab, treatment. Adult-onset Still’s disease (AOSD) is a rare diseases that may lead to similar clinical and systemic inflammatory disease with an unknown laboratory findings. etiology. The main clinical manifestations of It is well known that proinflammatory the disease are fever, maculopapular salmon- pink rash, arthralgia, and arthritis. -

Orthopaedics Instructions: to Best Navigate the List, First Download This PDF File to Your Computer
Orthopaedics Instructions: To best navigate the list, first download this PDF file to your computer. Then navigate the document using the bookmarks feature in the left column. The bookmarks expand and collapse. Finally, ensure that you look at the top of each category and work down to review notes or specific instructions. Bookmarks: Bookmarks: notes or specific with expandable instructions and collapsible topics As you start using the codes, it is recommended that you also check in Index and Tabular lists to ensure there is not a code with more specificity or a different code that may be more appropriate for your patient. Copyright APTA 2016, ALL RIGHTS RESERVED. Last Updated: 09/14/16 Contact: [email protected] Orthopaedics Disorder by site: Ankle Achilles tendinopathy ** Achilles tendinopathy is not listed in ICD10 M76.6 Achilles tendinitis Achilles bursitis M76.61 Achilles tendinitis, right leg M76.62 Achilles tendinitis, left leg ** Tendinosis is not listed in ICD10 M76.89 Other specified enthesopathies of lower limb, excluding foot M76.891 Other specified enthesopathies of right lower limb, excluding foot M76.892 Other specified enthesopathies of left lower limb, excluding foot Posterior tibialis dysfunction **Posterior Tibial Tendon Dysfunction (PTTD) is not listed in ICD10 M76.82 Posterior tibial tendinitis M76.821 Posterior tibial tendinitis, right leg M76.822 Posterior tibial tendinitis, left leg M76.89 Other specified enthesopathies of lower limb, excluding foot M76.891 Other specified enthesopathies of right lower limb, -

Download Versus Arthritis
Elbow pain Elbow pain information booklet Contents How does the elbow work? 4 What causes elbow pain and stiffness? 6 Should I see a healthcare professional? 8 What can I do to help myself? 9 How are elbow problems diagnosed? 12 What treatments are there for elbow pain? 14 Specific elbow conditions 18 Glossary 26 Research and new developments 27 Keeping active with elbow pain 28 Where can I find out more? 32 We’re the 10 million people living with arthritis. We’re the carers, researchers, health professionals, friends and parents all united in Talk to us 33 our ambition to ensure that one day, no one will have to live with the pain, fatigue and isolation that arthritis causes. We understand that every day is different. We know that what works for one person may not help someone else. Our information is a collaboration of experiences, research and facts. We aim to give you everything you need to know about your condition, the treatments available and the many options you can try, so you can make the best and most informed choices for your lifestyle. We’re always happy to hear from you whether it’s with feedback on our information, to share your story, or just to find out more about the work of Versus Arthritis. Contact us at [email protected] Words shown are explained in the glossary on p.26. Registered office: Versus Arthritis, Copeman House, St Mary’s Gate, Chesterfield S41 7TD in bold Registered Charity England and Wales No. 207711, Scotland No. SC041156.