Middlesex-London Board of Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2018 Election New Democratic Party of Ontario Candidates
2018 Election New Democratic Party of Ontario Candidates NAME RIDING CONTACT INFORMATION Monique Hughes Ajax [email protected] Michael Mantha Algoma-Manitoulin [email protected] Pekka Reinio Barrie-Innisfil [email protected] Dan Janssen Barrie-Springwater-Ono- [email protected] Medonte Joanne Belanger Bay of Quinte [email protected] Rima Berns-McGown Beaches-East York [email protected] Sara Singh Brampton Centre [email protected] Gurratan Singh Brampton East [email protected] Jagroop Singh Brampton West [email protected] Alex Felsky Brantford-Brant [email protected] Karen Gventer Bruce-Grey-Owen Sound [email protected] Andrew Drummond Burlington [email protected] Marjorie Knight Cambridge [email protected] Jordan McGrail Chatham-Kent-Leamington [email protected] Marit Stiles Davenport [email protected] Khalid Ahmed Don Valley East [email protected] Akil Sadikali Don Valley North [email protected] Joel Usher Durham [email protected] Robyn Vilde Eglinton-Lawrence [email protected] Amanda Stratton Elgin-Middlesex-London [email protected] NAME RIDING CONTACT INFORMATION Taras Natyshak Essex [email protected] Mahamud Amin Etobicoke North [email protected] Phil Trotter Etobicoke-Lakeshore [email protected] Agnieszka Mylnarz Guelph [email protected] Zac Miller Haliburton-Kawartha lakes- [email protected] -
District Name
District name Name Party name Email Phone Algoma-Manitoulin Michael Mantha New Democratic Party of Ontario [email protected] 1 416 325-1938 Bramalea-Gore-Malton Jagmeet Singh New Democratic Party of Ontario [email protected] 1 416 325-1784 Essex Taras Natyshak New Democratic Party of Ontario [email protected] 1 416 325-0714 Hamilton Centre Andrea Horwath New Democratic Party of Ontario [email protected] 1 416 325-7116 Hamilton East-Stoney Creek Paul Miller New Democratic Party of Ontario [email protected] 1 416 325-0707 Hamilton Mountain Monique Taylor New Democratic Party of Ontario [email protected] 1 416 325-1796 Kenora-Rainy River Sarah Campbell New Democratic Party of Ontario [email protected] 1 416 325-2750 Kitchener-Waterloo Catherine Fife New Democratic Party of Ontario [email protected] 1 416 325-6913 London West Peggy Sattler New Democratic Party of Ontario [email protected] 1 416 325-6908 London-Fanshawe Teresa J. Armstrong New Democratic Party of Ontario [email protected] 1 416 325-1872 Niagara Falls Wayne Gates New Democratic Party of Ontario [email protected] 1 416 212-6102 Nickel Belt France GŽlinas New Democratic Party of Ontario [email protected] 1 416 325-9203 Oshawa Jennifer K. French New Democratic Party of Ontario [email protected] 1 416 325-0117 Parkdale-High Park Cheri DiNovo New Democratic Party of Ontario [email protected] 1 416 325-0244 Timiskaming-Cochrane John Vanthof New Democratic Party of Ontario [email protected] 1 416 325-2000 Timmins-James Bay Gilles Bisson -
Meeting Package
Board of Health Meeting 410 Buller Street, Woodstock, Ontario, N4S4N2 Basement Boardroom Wednesday, June 13, 2018 5:00 p.m. AGENDA Item Agenda Item Lead Expected Outcome 1.0 COVENING THE MEETING 1.0 Call to Order, Recognition of Quorum Chair • Introduction of Guests, Board of Health Members and Staff 1.1 Approval of Agenda Chair Decision 1.2 Reminder to disclose Pecuniary Interest and the General nature Chair Thereof when Item Arises 1.3 Reminder that Meetings are Recorded Chair 2.0 APPROVAL OF MINUTES 2.1 Approval of Minutes from May 1, 2018 Chair Decision 3.0 APPROVAL OF CONSENT AGENDA None. 4.0 CORRESPONDENCE RECEIVED REQUIRING ACTION 4.1 May 3, 2018 – Letter from Peterborough PH (OFRB) re: Smoke Peter Heywood Decision Free Movies 4.2 March 28, 2018 – Letter from Hastings Prince Edward Public Peter Heywood Decision Health re: Cannabis Tax Revenue 5.0 CORRESPONDENCE RECEIVED AND FILED 5.1 May 3, 2018 – Letter from Peterborough PH (MPP Laurie Scott) Information Only and Filed re: Smoke Free Movies 5.2 May 3, 2018 – Letter from Peterborough PH (MPP Jeff Leal) re: Information Only and Filed Smoke Free Movies 5.3 April 26, 2018 – Letter from Kingston, Frontenac and Lennox & Information Only and Filed Addington Public Health re: Food Literacy Curriculum 5.4 April 19, 2018 – Report Update from Windsor Essex County Information Only and Filed Health Unit re: Oral health Update 2018 5.5 April 19, 2018 – Report from Windsor Essex County Health Unit Information Only and Filed re: Oral Health Update 2018 5.6 April 19, 2018 – Letter from Grey Bruce -

Government of Ontario Key Contact Ss
GOVERNMENT OF ONTARIO 595 Bay Street Suite 1202 Toronto ON M5G 2C2 KEY CONTACTS 416 586 1474 enterprisecanada.com PARLIAMENTARY MINISTRY MINISTER DEPUTY MINISTER PC CRITICS NDP CRITICS ASSISTANTS Steve Orsini Patrick Brown (Cabinet Secretary) Steve Clark Kathleen Wynne Andrea Horwath Steven Davidson (Deputy Leader + Ethics REMIER S FFICE Deb Matthews Ted McMeekin Jagmeet Singh P ’ O (Policy & Delivery) and Accountability (Deputy Premier) (Deputy Leader) Lynn Betzner Sylvia Jones (Communications) (Deputy Leader) Lorne Coe (Post‐Secondary ADVANCED EDUCATION AND Han Dong Peggy Sattler Education) Deb Matthews Sheldon Levy Yvan Baker Taras Natyshak SKILLS DEVELOPMENT Sam Oosterhoff (Digital Government) (Digital Government) +DIGITAL GOVERNMENT (Digital Government) AGRICULTURE, FOOD AND RURAL AFFAIRS Jeff Leal Deb Stark Grant Crack Toby Barrett John Vanthof +SMALL BUSINESS ATTORNEY GENERAL Yasir Naqvi Patrick Monahan Lorenzo Berardinetti Randy Hillier Jagmeet Singh Monique Taylor Gila Martow (Children, Jagmeet Singh HILDREN AND OUTH ERVICES Youth and Families) C Y S Michael Coteau Alex Bezzina Sophie Kiwala (Anti‐Racism) Lisa MacLeod +ANTI‐RACISM Jennifer French (Anti‐Racism) (Youth Engagement) Jennifer French CITIZENSHIP AND IMMIGRATION Laura Albanese Shirley Phillips (Acting) Shafiq Qaadri Raymond Cho Cheri DiNovo (LGBTQ Issues) Lisa Gretzky OMMUNITY AND OCIAL ERVICES Helena Jaczek Janet Menard Ann Hoggarth Randy Pettapiece C S S (+ Homelessness) Matt Torigian Laurie Scott (Community Safety) (Community Safety) COMMUNITY SAFETY AND Margaret -

PEO GOVERNMENT LIAISON PROGRAM Volume 14, 2020 GLP WEEKLY Issue 28
August 21, PEO GOVERNMENT LIAISON PROGRAM Volume 14, 2020 GLP WEEKLY Issue 28 PEO PRESIDENT SHARES GOALS WITH THE GOVERNMENT LIAISON COMMITTEE The PEO Government Liaison Committee (GLC) held its monthly meeting online on August 19. Joining them was PEO President Marisa Sterling, P.Eng (above), who discussed her 10 year vision for PEO with the Committee. Also attending the meeting were PEO’s GLC Chair Warren Turnbull, P.Eng., Councillor Lorne Cutler, P.Eng., Engineers Canada rep Changiz Sadr, P.Eng., Chapter rep Gabe Tse, P.Eng., Advisory Committee Volunteer rep Vicki Hilborn, P.Eng., active riding association member Jeffrey Lee, P.Eng., EIT rep Alex Weryha, EIT, student rep Shawn Yanni, Manager, Government Liaison Programs Jeannette Chau, P.Eng. and Government Relations Consultant Howard Brown. For more on this story, see page 3. Through the Professional Engineers Act, PEO governs over 89,000 licence and certificate holders, and regulates and advances engineering practice in Ontario to protect the public interest. Professional engineering safeguards life, health, property, economic interests, the public welfare and the environment. Past issues are available on the PEO Government Liaison Program (GLP) website at https://www.peo.on.ca/index.php/about-peo/glp-weekly- newsletter Deadline for submissions is the Thursday of the week prior to publication. The next issue will be published on August 28, 2020. 1 | PAGE TOP STORIES THIS WEEK 1. MINISTER, PARTY LEADER AND MPPS HOLD EVENTS 2. PEO GLP REP SHARES HIS INSIGHTS ON THE IMPORTANCE OF THE GLP PEO GOVERNMENT LIAISON PROGRAM WORKS The PEO Government Liaison Committee held their monthly virtual meeting this week, and were joined by PEO President Marisa Sterling, P.Eng. -

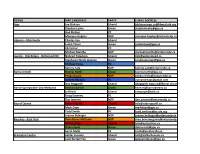
Ontario Government Quick Reference Guide: Key Officials and Opposition Critics August 2014
Ontario Government Quick Reference Guide: Key Officials and Opposition Critics August 2014 Ministry Minister Chief of Staff Parliamentary Assistant Deputy Minister PC Critic NDP Critic Hon. David Aboriginal Affairs Milton Chan Vic Dhillon David de Launay Norm Miller Sarah Campbell Zimmer Agriculture, Food & Rural Affairs Hon. Jeff Leal Chad Walsh Arthur Potts Deb Stark Toby Barrett N/A Hon. Lorenzo Berardinetti; Sylvia Jones (AG); Jagmeet Singh (AG); Attorney General / Minister responsible Shane Madeleine Marie-France Lalonde Patrick Monahan Gila Martow France Gélinas for Francophone Affairs Gonzalves Meilleur (Francophone Affairs) (Francophone Affairs) (Francophone Affairs) Granville Anderson; Alexander Bezzina (CYS); Jim McDonell (CYS); Monique Taylor (CYS); Children & Youth Services / Minister Hon. Tracy Omar Reza Harinder Malhi Chisanga Puta-Chekwe Laurie Scott (Women’s Sarah Campbell responsible for Women’s Issues MacCharles (Women’s Issues) (Women’s Issues) Issues) (Women’s Issues) Monte Kwinter; Cristina Citizenship, Immigration & International Hon. Michael Christine Innes Martins (Citizenship & Chisanga Puta-Chekwe Monte McNaughton Teresa Armstrong Trade Chan Immigration) Cindy Forster (MCSS) Hon. Helena Community & Social Services Kristen Munro Soo Wong Marguerite Rappolt Bill Walker Cheri DiNovo (LGBTQ Jaczek Issues) Matthew Torigian (Community Community Safety & Correctional Hon. Yasir Brian Teefy Safety); Rich Nicholls (CSCS); Bas Balkissoon Lisa Gretzky Services / Government House Leader Naqvi (GHLO – TBD) Stephen Rhodes (Correctional Steve Clark (GHLO) Services) Hon. David Michael Government & Consumer Services Chris Ballard Wendy Tilford Randy Pettapiece Jagmeet Singh Orazietti Simpson Marie-France Lalonde Wayne Gates; Economic Development, Employment & Hon. Brad (Economic Melanie Wright Giles Gherson Ted Arnott Percy Hatfield Infrastructure Duguid Development); Peter (Infrastructure) Milczyn (Infrastructure) Hon. Liz Education Howie Bender Grant Crack George Zegarac Garfield Dunlop Peter Tabuns Sandals Hon. -
RIDING MPP CANDIDATE PARTY E-MAIL ADDRESS Ajax Joe
RIDING MPP CANDIDATE PARTY E-MAIL ADDRESS Ajax Joe Dickson Liberal [email protected] Stephen Leahy Green [email protected] Rod Phillips PC Monique Hughes NDP [email protected] Algoma—Manitoulin Charles Fox Liberal Justin Tilson Green [email protected] Jib Turner PC Michael Mantha NDP [email protected] Aurora - Oak Ridges - Richmond Hill Naheed Yaqubian Liberal [email protected] Stephanie Nicole Duncan Green [email protected] Michael Parsa PC Katrina Sale NDP [email protected] Barrie-Innisfil Bonnie North Green [email protected] Pekka Reinio NDP [email protected] Andrea Khanjin PC [email protected] Ann Hoggarth Liberal [email protected] Barrie-Springwater-Oro-Medonte Keenan Aylwin Green [email protected] Jeff Kerk Liberal [email protected] Doug Downey PC Dan Janssen NDP [email protected] Bay of Quinte Robert Quaiff Liberal [email protected] Mark Daye Green [email protected] Todd Smith PC [email protected] Joanne Belanger NDP [email protected] Beaches—East York Rima Berns-McGown NDP [email protected] Arthur Potts Liberal [email protected] Debra Scott Green [email protected] Sarah Mallo PC [email protected] Brampton Centre Safdar Hussain Liberal [email protected] Laila Zarrabi Yan Green [email protected] Harjit Jaswal PC [email protected] Sara Singh NDP [email protected] Brampton East Dr. Parminder Singh Liberal [email protected] Raquel Fronte Green [email protected] Sudeep Verma PC Gurratan -

Angry Birds: Twitter Harassment of Canadian Female Politicians By
Angry Birds: Twitter Harassment of Canadian Female Politicians By Jess Ann Gordon Submitted to the Faculty of Extension University of Alberta In partial fulfillment of the requirements for the degree of Master of Arts in Communications and Technology August 5, 2019 2 Acknowledgments Written with gratitude on the unceded traditional territories of the Skwxw�7mesh (Squamish), Səl̓ �lwətaʔ/Selilwitulh (Tsleil-Waututh), and xʷməθkʷəy̓əm (Musqueam) Nations, and on Treaty 6 territory, the traditional lands of diverse Indigenous peoples including the Cree, Blackfoot, Métis, Nakota Sioux, Iroquois, Dene, Ojibway, Saulteaux, Anishinaabe, Inuit, and many others. I would like to take this opportunity to thank my friends, family, cohort colleagues, and professors who contributed to this project. Thank you to my project supervisor, Dr. Gordon Gow, for his steadying support throughout the project and the many valuable suggestions. Thank you as well to Dr. Stanley Varnhagen, who provided invaluable advice on the design and content of the survey. I am grateful to both Dr. Gow and Dr. Varnhagen for sharing their expertise and guidance to help bring this project to life. Thank you to my guinea pigs, who helped me to identify opportunities and errors in the draft version of the survey: Natalie Crawford Cox, Lana Cuthbertson, Kenzie Gordon, Ross Gordon, Amanda Henry, Lucie Martineau, Kory Mathewson, and Ian Moore. Thank you to my MACT 2017 cohort colleagues and professors their support and encouragement. Particularly, I’d like to thank Ryan O’Byrne for helping me to clarify the project concept in its infant stages, and for being a steadfast cheerleader and friend throughout this project and the entire MACT program. -

Student Alliance
ONTARIO UNDERGRADUATE STUDENT ALLIANCE ADVOCACY CONFERENCE 2020 November 16-19th ABOUT OUSA The Ontario Undergraduate Student Alliance (OUSA) represents the interests of approximately 150,000 professional and undergraduate, full-time and part-time university students at eight student associations across Ontario. Our vision is for an accessible, affordable, accountable and high quality post-secondary education in Ontario. OUSA’s approach to advocacy is based on creating substantive, student driven, and evidence-based policy recommendations. INTRODUCTION Student leaders representing over 150,000 undergraduate students from across Ontario attended OUSA’s annual Student Advocacy Conference from November 16th to the 19th. Delegates met with over 50 MPPs from four political parties and sector stakeholders to discuss the future of post-secondary education in Ontario and advance OUSA’s advocacy priorities. Over five days, the student leaders discussed student financial aid, quality of education, racial equity, and student mental health. As we navigate the global pandemic, OUSA recommends improvements to the Ontario Student Assistance Program (OSAP), guidance and support for quality online learning, training and research to support racial equity, and funding for student mental health services. Overall, OUSA received a tremendous amount of support from members and stakeholders. ATTENDEES Julia Periera (WLUSU) Eric Chappell (SGA-AGÉ) Devyn Kelly (WLUSU) Nathan Barnett (TDSA) Mackenzy Metcalfe (USC) Rayna Porter (TDSA) Matt Reesor (USC) Ryan Tse (MSU) Megan Town (WUSA) Giancarlo Da-Ré (MSU) Abbie Simpson (WUSA) Tim Gulliver (UOSU-SÉUO) Hope Tuff-Berg (BUSU) Chris Yendt (BUSU) Matthew Mellon (AMS) Alexia Henriques (AMS) Malek Abou-Rabia (SGA-AGÉ) OUSA MET WITH A VARIETY OF STAKEHOLDERS MPPS CABINET MINISTERS Minister Michael Tibollo MPP Stephen Blais Office of Minister Monte McNaughton MPP Jeff Burch Office of Minister Peter Bethlenfalvy MPP Teresa Armstrong . -

Second Report from the Mayor's Economic And
We’re all in this together Second Report from the Mayor’s Economic and Social Impact and Recovery Task Forces 8 May 2020 Introduction 2 Progress so far 3 Ideas for Action 6 During the shutdown 6 Grants rather than loans or deferrals for commercial rent (already actioned) 6 Pooling resources or collaborating to allow smaller organizations access to EAP services like counselling 6 Insurance companies should reduce premiums to reflect changes in economic activity and mobility 7 Consider distributing funds though existing organizations like Regional Innovation Centres 7 Delivery food on a regular basis to agencies that provide food to people 7 Maximize number of people receiving support through discretionary benefits 7 Supporting physical distancing by people who are living unsheltered 7 Communicate government programs via widely available print publications that are delivered 7 Continuing transit service to make sure people can continue to move around the city for essential trips 8 Significant increases in funding for mental health for children and youth 8 Clarify how psychotherapists can provide emergency counselling 8 Broaden distribution of comfort stations to include Hamilton Road 8 Providing blankets to agencies working with people experiencing homelessness 8 Expand the number of monthly rent supplements 8 Creating more space to provide shelter 8 Connecting faith communities to support service agencies 9 Supporting the specific needs of international students 9 During the recovery 9 Rapid shift to office employees working remotely should -

September 11, 2018 7:00 P.M
The Niagara Catholic District School Board through the charisms of faith, social justice, support and leadership, nurtures an enriching Catholic learning community for all to reach their full potential and become living witnesses of Christ. AGENDA AND MATERIAL COMMITTEE OF THE WHOLE MEETING TUESDAY, SEPTEMBER 11, 2018 7:00 P.M. FATHER KENNETH BURNS, C.S.C. BOARD ROOM CATHOLIC EDUCATION CENTRE, WELLAND, ONTARIO A. ROUTINE MATTERS 1. Opening Prayer – Trustee Burtnik - 2. Roll Call - 3. Approval of the Agenda - 4. Declaration of Conflict of Interest - 5. Approval of Minutes of the Committee of the Whole Meeting - 5.1 June 12, 2018 A5.1 5.2 June 20, 2018 A5.2 6. Consent Agenda Items - 6.1 Architect Selection for Monsignor Clancy Catholic Elementary School and A6.1 Our Lady of Mount Carmel Catholic Elementary School 6.2 Staff Development Department Professional Development Opportunities A6.2 6.3 In Camera Items F1.1, F1.2 and F4 - B. PRESENTATIONS C. COMMITTEE AND STAFF REPORTS 1. Director of Education and Senior Staff Introduction to the 2018-2019 School Year C1 2. Provisions of Special Education Programs and Services - Special Education Plan C2 3. Niagara Compliance Audit Committee Report C3 4. Monthly Updates 4.1 Student Senate Update - 4.2 Senior Staff Good News Update - D. INFORMATION 1. Trustee Information 1.1 Spotlight on Niagara Catholic – June 19, 2018 D1.1 1.2 Calendar of Events – September 2018 D1.2 2 1.3 Ontario Legislative Highlights – June 22, 2018, July & August 2018 D1.3 1.4 Letter to Parents and Guardians – September 2018 D1.4 1.5 Niagara Foundation for Catholic Education Golf Tournament – September 19, 2018 D1.5 1.6 OCSTA 2018 Fall Regional Meeting – September 26, 2018 D1.6 1.7 OCSTA 2018 Fall Regional Meeting Questions for Discussion D1.7 E. -

Board of Health
Board of Health Thursday, September 20, 2018 1:30 p.m. Public Health Sudbury & Districts Boardroom 1300 Paris Street Board of Health, Public Health Sudbury & Districts, September 20, 2018 Board of Health Meeting #06-18 1.0 CALL TO ORDER 2.0 ROLL CALL 3.0 REVIEW OF AGENDA / DECLARATIONS OF CONFLICT OF INTEREST Agenda - September 20, 2018 Page 7 4.0 DELEGATION / PRESENTATION i) Public Health Update on Cannabis Anik Proulx, Manager, Health Promotion Division 5.0 CONSENT AGENDA i) Minutes of Previous Meeting a. Fifth Meeting – June 21, 2018 Page 11 ii) Business Arising From Minutes iii) Report of Standing Committees a. Board of Health Executive Committee Unapproved Page 18 Minutes, July 11, 2018 iv) Report of the Medical Officer of Health / Chief Executive Officer a. MOH/CEO Report, September 2018 Page 21 Financial Statements ending July 31, 2018 Page 36 v) Correspondence a. Repeal of Section 43 of the Criminal Code Refresh 2017 Letter from the Perth Board of Health to the Minister of Page 40 Justice dated June 14, 2018 b. Cannabis Sales Taxation Revenue Page 2 of 152 Letter from the Grey Bruce Health Unit Acting Medical Page 41 Officer of Health to the Premier-Elect dated June 18, 2018 c. Recommendation/Resolution Report – Oral Health Report Update 2018 Letter from the Grey Bruce Health Unit Acting Medical Page 42 Officer of Health to the Windsor-Essex County Health Unit dated June 18, 2018 d. Youth Exposure to Smoking in Movies Letter from the Grey Bruce Health Unit Acting Medical Page 43 Officer of Health to the Ontario Film Review Board dated June 18, 2018 e.