Modern Approaches for Diagnosing Transformations of the Heart in Qualified Athletes
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Npr 3.2: Nuclear-Related Trade and Cooperation
Nuclear Developments NUCLEAR-RELATED TRADE AND COOPERATION DEVELOPMENTS FOR SELECTED STATES, JULY-OCTOBER 1995 CONTENTS OVERVIEW, 97 France, Japan, United COMMONWEALTH OF FRANCE Kingdom, and U.S., 118 INDEPENDENT STATES with ALGERIA Russia, 119 with Belgium, Canada, Germany, with Iran, 108 Russia, and United King- PRC, 99 BRAZIL dom, 141 Internal Developments, 102 CUBA ARGENTINA Belgium, Finland, and with Internal Developments, 104 with Ukraine, 154 Argentina, 99 with Brazil, 99 Belgium, Japan, United Argentina, Cuba, and Argentina, Brazil, and Brazil, Cuba, and Mexico, 99 Kingdom, and U.S., 118 Mexico, 99 Mexico, 99 Israel and United States, 99 Cuba (Juragua Plant), 104 Germany, 103 Juragua Plant Participants South Korea, 99 Japan, 119 India, Indonesia, PRC and (Brazil, France, Germany, Syria, 99 Kazakhstan, 121 Russia, 103 Italy, Russia, and United United States, 100 PRC, 133 Russia, 103 Kingdom), 104 PRC and United Kingdom, 133 United States, 103 Mexico, 105 ARMENIA Russia, 142 with BULGARIA CZECH REPUBLIC South Korea and U.S., 151 ISTC, 100 with with Ukraine, 154 Russia and Ukraine, 141 Iran, 108 ASSOCIATION OF SOUTH GEORGIA EAST ASIAN NATIONS Russia and Slovakia, 142 CAMBODIA with (ASEAN) Ukraine, 154 with IAEA, 106 Internal Developments, 100 Thailand and Vietnam, 153 EGYPT ISTC, 100 BELARUS Internal Developments, 105 CANADA GERMANY with with ESTONIA with Estonia and Ukraine, 101 Belgium, France, Germany, with Belgium, Canada, France, Iran, 101 Russia, and U.K., 141 Belarus and Ukraine, 101 Russia, and U.K., 141 ISTC, 100 Japan, -

26 June COVID-19 Situation Report
№6 (ISSUED BIWEEKLY) 26 JUNE 2020 COVID-19 SITUATION REPORT HIGHLIGHTS UN SUPPORTS SAFE RE-OPENING OF SCHOOLS The widespread closure of educational facilities in response to the COVID-19 pandemic presented an unprecedented risk to the education and well-being of children, especially the most vulnerable, who rely heavily on schools for their education, health, safety and nutrition. The new UNICEF guidelines provide practical guidance to central and local executive authorities on how to work together to ensure the right of every child to education, health and safety while returning to school. Schools should assess their readiness to open after quarantine and provide an improved and safe learning environment and comprehensive support for The UN Country Team in Kazakhstan congratulates the healthcare workers of Kazakhstan children, including health, nutrition, psychosocial support and quality assurance of water, sanitation and hygiene facilities. A NEW COVID-19 SURGE IN KAZAKHSTAN More on socio-economic response on page 2. NUR-SULTAN – Kazakhstan celebrated on 21 June the Healthcare Workers Day, on the occasion of which President Kassym-Jomart Tokayev decreed to award the most distinguished medical workers with medals and orders. The UN Country Team has also congratulated the medical workers, noting their outstanding contribution in UN CALLS FOR EQUAL fighting the COVID-19 outbreak. DISTRIBUTION OF WORK DURING COVID-19 Over the past three months, the medical workers have faced an unprecedented LOCKDOWN amount of work under quarantine in their hospitals away from their families to fight the pandemic. The number of COVID-19 cases is gradually growing in Kazakhstan, despite the restricted lockdown measures and information campaigns. -
COVID-19 Central Asia Infographic Series
COVID-19 in Central Asia: Infographic Series KAZAKHSTAN Kazakhstan first announced a state of emergency and imposed a nationwide lockdown from March 16 to May 11. As cases started to climb after the lockdown lifted, and new data collection methods pointed to more 78,486 49,488 585 infections in the country than previously counted, the Total Confirmed Recovered Deaths government announced a second nationwide lockdown COVID-19 Cases from July 5 to August 2. Kazakhstan has the highest Source: JHU number of COVID-19 infections relative to population size in Central Asia. Nur-Sultan (formerly Astana) Atyrau Tengiz Oil Field Almaty IMPACT TO THE PRIVATE SECTOR COVID-19 is the biggest shock to Kazakhstan's economy in two decades, and has had a negative impact on economic growth. The economy is heavily reliant on foreign investment through ongoing oil, gas, and infrastructure projects. The Tengiz Oil Field in the Atyrau region has reported upwards of 2,000 cases of COVID-19 among 36 shift camps and 57 companies operating in the field. Chevron-led Tengizchevroil owns the site, and has temporarily paused non-essential work activities in an attempt to slow the spread of cases. Entry restrictions may affect the movement of migrant workers staffing the project site. The capital, Nur-Sultan, and Kazakhstan's financial hub, Almaty, have led the count in confirmed cases of COVID-19. Hospitals in both major cities are reportedly nearing full capacity, and may be unavailable to new patients. In Nur-Sultan, the Presidential Hospital and City Hospital #2 recently resumed some level of surgical and other services, opening up access to acute trauma care. -

MBA October 2010 Rec
Issue o. 10/2010 MONTHLY BULLETIN OF ACTIVITIES OF THE CONVENTION ON BIOLOGICAL DIVERSITY OCTOBER 2010 Tenth meeting of the Conference of the Parties to the Convention on Biological Diversity The tenth meeting of the Conference of COP10 President deliv- gic Plan or the “Aichi Target” to guide the Parties to the Convention on Biologi- ered opening remarks, international and national efforts to save cal diversity was held in Nagoya, Aichi followed by statements biodiversity through enhanced action to Prefecture of Japan, from 18 to 29 Octo- from: Mr. Masaaki meet the objectives of the Convention on ber 2010, with the theme “Life in har- Kanda, Governor of the Biological Diversity, a resource mobiliza- mony, into the future”. Surpassing its Aichi Prefecture; Taka- tion strategy that provides the way for- record of attendance to date, the meeting shi Kawamura, mayor of ward to a substantial increase to current gathered the participation of more than Nagoya City; Mr. levels of official development assistance 18,000 participants. Achim Steiner, UNEP in support of biodiversity; and a new in- The opening ceremony Executive Director; and MISIA ternational protocol on access to and shar- started with a traditional Mr. Ahmed Djoghlaf, ing of the benefits from the use of the arts performance, with CBD Executive Secretary. A video pre- genetic resources of the planet. 47 deci- Yoko Deva playing the pared by the Government of Japan was sions were adopted in total, including a Shinobue and a shadow shown, which was followed by a perform- plan of action on cities and biodiversity; a play by the Kakashi-za ance by MISIA, COP10 Honorary Am- multi-year programme of action on south- Yoko Deva group. -

Implementing the Almaty Declaration: Experiences and Future Opportunities” – Harbin, PR China
Countries and areas of the WHO Eastern Mediterranean and European regions that participated in Operation MECACAR “Implementing the Almaty Declaration: Experiences and Future Opportunities” – Harbin, PR China 26 September 2007 Geneva, 7-9 Nov. 2005 (UN system) Local Regional Global 1 5 9 Development of ‘Rapid response’ Expanded global integrated teams of experts anti-viral stockpile national plans 2 Aggressive control of 6 10 Global strategy Avian Influenza in birds Stronger country and for vaccine research and human pandemic regional capacity and development preparedness 3 7 11 Assess needs of Costing of country Expanded network of veterinary plans and regional and influenza laboratories infrastructures global requirements 4 8 12 Voluntary compliance Finalize coordination Multi-country technical of International Health framework building on networks Regulations existing mechanisms Influenza Regional Meeting (12-13 June 2006) Principles: Joint funding and planning of agencies & donors Move towards performance-based mechanism towards regional collaboration to fight influenza threats Sponsors: WHO, UNICEF, UNDP, FAO, USAID, US-CDC, European Commission, World Bank, ADB (contributions: $ 7,000 - $ 25,000) Extra speakers: UNSIC & OiE Central Asia Roundtable Participating (=CAREC): Invited: • Kazakhstan, Kyrgyz • International Republic, Tajikistan, organizations Turkmenistan, Uzbekistan • Greater Mekong • Russian Federation Sub-Region • XUAR, PR China (e.g. Thailand) • Afghanistan, Mongolia Experts (human & animal health sector, coordination & communication) & Senior officials Institutional framework • Intersectoral government co-ordination (agriculture, health, emergencies/ KAZ) -> endorsed 7 April • Interagency co-ordination (ADB, EC, UNSIC & 3 UN agencies [FAO, UNICEF, WHO], USAID, World Bank) -> weekly teleconference meetings (27 March, 3 & 10 April) • Conference Secretariat linked with technical working group & administrative support -> established 29 March Country needs (next 2-3 yrs) 1. -

Presentation on “Traincost” Point-To-Point Train Costing Model
Expert Group Meeting on Documentation and Procedures for Rail- Based Intermodal Transport Services in Northeast and Central Asia Bangkok 30-31 August 2016 Item 6: Overview of documents and procedures in current use on selected routes: Routes 1A, 1B and 2 Building 1 CONTENT For international transit routes: 1A (Republic of Korea to Europe via China and Kazakhstan); 1B (Republic of Korea to Central Asia via China); and 2 (Republic of Korea via China, Mongolia and Russian Federation), will consider: 1. Route status and major traffic flows 2. Summary of border control procedures and performance for route 3. Border control procedures in ports 4. Border control procedures at land borders 5. Documents used for border clearance along each route 2 Routes 1A and 1B: 1. Route status and major traffic flows • Routes shown in map on next slide • Route 1A starts in Port of Busan ROK and ends in Duisberg, Germany – total distance of 12,240 km, of which sea distance (via Lianyungang Port) is 1,114 km and rail distance 11,126 km • Route 1B starts in Port of Busan or Port of Incheon ROK and ends in Almaty or Tashkent – total distance (Incheon-Almaty via Qingdao Port), 5,549 km, of which sea distance is 659 km and rail distance 4,890 km • Both routes pass through one of two border control posts on the border between China and Kazakhstan, at Dostyk/Alashankou or Altynkol/Khorgos, where international cargo is stopped for transhipment between rail gauges, as well as for inspection and clearance procedures • In addition to intermodal transit cargo between ROK -

Almaty Process” As a Full Operational Regional Consultative Forum for Central Asia on Mixed Migration and International Protection;
Recommendations on the preparations for the formal launching of the “Almaty Process” as a full operational regional consultative forum for Central Asia on mixed migration and international protection; Issued by the participants of the first meeting of National Coordinators on mixed migration in Central Asia, held in Almaty, Kazakhstan on 7 September 2012 Preamble We, the National Coordinators on Mixed Migration, and delegations from the Central Asian Countries, reunited in the city of Almaty, together with Representatives of the Islamic Republic of Afghanistan, the Islamic Republic of Iran, the Russian Federation, and the Republic of Turkey, to discuss the follow-up to the Regional Conference on Refugee Protection and International Migration, held in Almaty on 15 and 16 March 2011; Bearing in mind that the Central Asian region needs a reliable consultative forum to manage the complex mixed migration movements that affect the region and its neighbouring areas in particular; Taking into consideration that the countries in the region would like to fulfil their international commitments to protect the people in need, particularly refugees, asylum-seekers, labour migrants, the stateless, victims of trafficking and others in need of international protection; Recognizing that these commitments have to be also realised under situations where considerable threats are being tackled by States, particularly the spread of extremism of different nature, smuggling, terrorism and irregular migration; Acknowledging thatt the issuance of concrete recommendations -
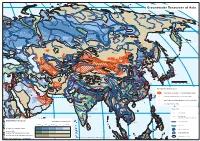
Groundwater Resources Map of Asia (PDF, 1
Groundwater Resources of Asia Murmansk Norilsk Anadyr Arkangelsk + Yakutsk + Saint Petersburg Magadan + Perm Yekaterinburg + Nizhniy Novgorod Moscow Kazan + Chelyabinsk Ufa Omsk + + Novosibirsk + + Samara Petropavlovsk-Kamchatskiy Irkutsk + + + Astana + + Kyiv + Kharkiv + Volgograd + + Dnipropetrovs'k + Khabarovsk + + Ulaanbaatar Rostov-na-Donu Astrakhan Harbin + Odesa + + + + + + Urumqi Changchun + + Jilin Sapporo + + Almaty T'bilisi Bishkek Vladivostok + Tashkent + Shenyang Istanbul H H Baotou + Huludao Ankara Yerevan Beijing + B Tangshan H + Baku + Bursa + Pyongyang + Dushanbe H + + + + Smyrana Tianjin Dalian + Tabriz Ashgabat H Dongguan Taiyuan+ + B Yantai Seoul Sendai + + + Adana Shijiazhuang + Inch'on Linyi+ + + Zibo Mashhad Lanzhou Jinan Al Mawsil Karaj H + Qingdao + Taegu Taian Taejon Tokyo H HAleppo B + Ulsan Nagoya + H Tehran + + Kyoto + Kabul Zhengzhou + + H Xian + Zaozhuang Kwangju Pusan Hiroshima B Xuzhou H H Beirut H Srinagar + + + H Fukuoka Osaka + Peshawar Suzhou + Damascus Baghdad B Rawalpindi Fuyang + Esfahan + H Gujranwala Tel Aviv-Yafo H Huainan Changzhou + + Amman + + H + B Faisalabad Amritsar Nanjing + H Alexandria + ++ H Jerusalem B B Wuxi Shanghai 0 250 500 750 1000 km H Lahore + Wuhan Suzhou H H Multan Ludhiana Ningbo H H + B Shiraz + Lhasa Chengdu + H H i iB Hangzhou + H iB Cairo H Kuwait Delhi + Meerut Chongqing B B + Changsha + i H H Faridabad Kathmandu Nanchang Special groundwater features H B Wenzhou + B H Jaipur + Agra Lucknow iB i + + Thimphu + + Kanpur Patna Guiyang Fuzhou + + H Dubai Allahabad area of -

Development of Seamless Rail-Based Intermodal Transport Services in Northeast and Central Asia
Development of seamless rail-based intermodal transport services in Northeast and Central Asia Report on Transport Facilitation procedures and documentation in Kazakhstan 1. Introduction A mission to Kazakhstan was conducted by a staff member and a consultant of the UNESCAP Transport Division for the express purpose of collecting information on border crossing procedures and documentation in Kazakhstan. The mission was conducted from 25-27 April 2016, during which period visits were made to: Three freight forwarding companies in Almaty; The Altynkol/Khorgos border region, including the Altynkol Station, the Khorgos Economic Zone, and the Khorgos Gateway Dry Port; The Kazakhstan Freight Forwarders Association This report reviews the status of trade and transport across Kazakhstan’s borders and outlines the main points of discussion at all meetings. 1. Status of cross-border trade and transport (i) Rail corridor developments Kazakhstan forms a key part of the shortest of the rail corridors linking Northeast Asia with Europe. As such, the majority of the container block trains now moving between China and Western Europe transit via this corridor (rather than via the Trans-Siberia or Trans-Mongolia Railways).1 The rail corridor through Kazakhstan also links major trade generating sources in Kazakhstan, such as Almaty and Astana, with seaports in China, most notably at Qingdao and Lianyungang. Rail traffic to/from China now exits/enters Kazakhstan through 2 major border control points. The oldest of these (operating since 1992) is at Dostyk, opposite Alashankou in China (see Figure 1). In 2014, more than 15 million tonnes of international cargo was estimated to have passed through this border station. -

Announcement Regarding the Establishment of Sales Subsidiary in Kazakhstan
For immediate release January 30, 2015 Company name: Representative: Shiro Hori, President, Representative Director Stock ticker code: 6586 Announcement Regarding the Establishment of Sales Subsidiary in Kazakhstan Makita Corporation (Head office: Anjo, Aichi Prefecture, Japan; President Shiro Hori; Capital 24,206 million yen) announces that Makita established a new sales subsidiary in Kazakhstan in order to strengthen its sales activities and after-sales services in the country. The newly established sales subsidiary plans to start operation on February 1, 2015. 1. Reasons for Establishing the New Subsidiary Before the establishment of Makita Kazakhstan LLP, Makita’s sales operations in the Kazakhstani market had been conducted by Makita Gulf FZE (our sales subsidiary established in April 1997 in Dubai, the United Arab Emirates; capitalized at US$6.1 million) through a local branch. By establishing a local sales subsidiary in Kazakhstan, which is enjoying rapid economic growth, Makita aims to further expand sales while exploring new business opportunities in other central Asian nations by expediting the supply of products and parts and enhancing its after-sales services. Kazakhstan, along with Russia, Belarus and Armenia, formed the Eurasian Economic Union, which was officially inaugurated in January 2015. Makita anticipates further growth of the Kazakhstani market, which will become a part of a larger unified market. As a result of the founding of the sales subsidiary in Kazakhstan, Makita currently operates 50 overseas subsidiaries (including 27 in Europe). 2. Outline of the New Subsidiary 1. Company name Makita Kazakhstan LLP 2. Location 39, Kommunalnaya, Zhetysu district, Almaty 3. Representative Yoshinori Matsumoto 4. Description of business Sales and after-sales service of electric power tools, pneumatic tools, outdoor power equipment and spare parts in Kazakhstan and neighboring countries 5. -

2021 Finalist Directory
2021 Finalist Directory April 29, 2021 ANIMAL SCIENCES ANIM001 Shrimply Clean: Effects of Mussels and Prawn on Water Quality https://projectboard.world/isef/project/51706 Trinity Skaggs, 11th; Wildwood High School, Wildwood, FL ANIM003 Investigation on High Twinning Rates in Cattle Using Sanger Sequencing https://projectboard.world/isef/project/51833 Lilly Figueroa, 10th; Mancos High School, Mancos, CO ANIM004 Utilization of Mechanically Simulated Kangaroo Care as a Novel Homeostatic Method to Treat Mice Carrying a Remutation of the Ppp1r13l Gene as a Model for Humans with Cardiomyopathy https://projectboard.world/isef/project/51789 Nathan Foo, 12th; West Shore Junior/Senior High School, Melbourne, FL ANIM005T Behavior Study and Development of Artificial Nest for Nurturing Assassin Bugs (Sycanus indagator Stal.) Beneficial in Biological Pest Control https://projectboard.world/isef/project/51803 Nonthaporn Srikha, 10th; Natthida Benjapiyaporn, 11th; Pattarapoom Tubtim, 12th; The Demonstration School of Khon Kaen University (Modindaeng), Muang Khonkaen, Khonkaen, Thailand ANIM006 The Survival of the Fairy: An In-Depth Survey into the Behavior and Life Cycle of the Sand Fairy Cicada, Year 3 https://projectboard.world/isef/project/51630 Antonio Rajaratnam, 12th; Redeemer Baptist School, North Parramatta, NSW, Australia ANIM007 Novel Geotaxic Data Show Botanical Therapeutics Slow Parkinson’s Disease in A53T and ParkinKO Models https://projectboard.world/isef/project/51887 Kristi Biswas, 10th; Paxon School for Advanced Studies, Jacksonville, -

Kazakhstan, Political Conditions in the Post-Soviet
PROFILE SERIES KAZAKHSTAN POLITICAL CONDITIONS IN THE POST-SOVIET ERA [PR/KAZ/94.001] SEPTEMBER 1994 All the sources of information in this document are identified and are publicly available. PRODUCED BY: INS RESOURCE INFORMATION CENTER 425 I STREET, N.W. (ULLICO BUILDING, 3RD FLOOR) WASHINGTON, D.C. 20536 DISCLAIMER The July 27, 1990 Regulations, "Aliens and Nationality: Asylum and Withholding of Deportation Procedures," mandated the creation of a new corps of Asylum Officers to provide an initial, nonadversarial adjudication of asylum claims. Asylum Officers use asylum law, interviews with asylum applicants, and relevant information on country conditions to determine the merits of individual claims for asylum. The Resource Information Center was created to assist Asylum Officers domestically, and Immigration Officers determining refugee status overseas, by collecting and disseminating credible and objective information on human rights conditions. As specified in the Regulations (8 CFR 208.12), such information may be obtained from the Department of Justice, the Department of State, and "other credible sources, such as international organizations, private voluntary organizations, or academic institutions." Resource Information Center Papers are one of the means by which information reflecting a wide range of credible sources is summarized for easy access by Asylum and Immigration Officers. The views expressed in Resource Information Center papers do not necessarily represent official U.S. Government opinion, nor do they reflect U.S. foreign policy concerns. This paper was written on the basis of publicly available information, analyses, and comment. All sources are cited. This paper cannot be, and does not purport to be, either exhaustive with regard to the country surveyed, or conclusive as to the merits of any claim to refugee status or asylum.