Q U a R T E R L Y M E D I C a L B U L L E T I N
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Volunteer Guide
Volunteer Guide Seva Mandir welcomes volunteers and interns from a variety of backgrounds, although relevant education and/or work experience within the field of interest is highly preferred. Former volunteers and interns include undergraduate students, graduate students, Ph.D.’s, recipients of fellowships, and career professionals, among others. You must be prepared to stay for a minimum of 2 months. **It is recommended that you bring a printed copy of this guide with you when you arrive at Seva Mandir** www.sevamandir.org Volunteer Guide 1. ABOUT SEVA MANDIR ................................................................................................................... 2 1.1. PROGRAMMES AND DEPARTMENTS ....................................................................................................... 2 1.2. WORK/OFFICE HOURS ........................................................................................................................ 3 2. PRE-DEPARTURE INFORMATION .................................................................................................... 3 2.1. HOW CAN I APPLY AS A VOLUNTEER IN SEVA MANDIR?.............................................................................3 2.2 WHAT CAN I EXPECT TO DO AT SEVA MANDIR? ........................................................................................ 3 2.3. WHAT DOES SEVA MANDIR EXPECT FROM ME? ....................................................................................... 5 2.4. PLANNING YOUR STAY ........................................................................................................................ -

SIF Institutional Information Current Approval Status
SIF Institutional Information Name of the Institution / Institution ID Pacific College Of Pharmacy Pacific Hills Pratap Nagar Extn Air Port Raod Debari Udaipur Rajasthan / PCI-1531 Institute Type existing Year of Establishment of Institute 2006 Extension of approval Raise in Admission Introduction of New Course Starting of Course (Academic Course Session) Conduct u/s 12 Number of admissions requested Yes/No Intake B.Pharm 2006 - 2007 D.Pharm 2010 - 2011 M.Pharm Pharmaceutics 2010 - 2011 M.Pharm Pharmaceutical Quality Assurance 2011 - 2012 M.Pharm Pharmacology 2010 - 2011 Institutional Information Upload the documentary evidence of PCI Approval View House no./ Bld. No./ Apt. No - Street/ Road/ Lane Air Port Road Area/locality/sector Pratap nagar Landmark Debari State/UT RAJASTHAN District UDAIPUR Block Gram Panchayat Debari Village Debari Police Station Pratap nagar Pin Code 313024 Post Office Debari Telephone No 3065000 STD code 294 Fax No 3065001 Email ID [email protected] Web site of institution www.pacific-university.ac.in Nearest Railway Station Udaipur Airport Dabok Details of the Society/Trust/ Management Status of the course conducting body private Name, address of the Society/Trust/ Management Pacific Academy of Higher Education and Research House no./ Bld. No./ Apt. No - Street/ Road/ Lane Air Port road Area/locality/sector Pratap Nagar Landmark Debari State/UT RAJASTHAN District UDAIPUR Block Gram Panchayat Debari Village Debari Police Station Pratap nagar Pin Code 313024 Post Office Debari Telephone No 3065000 STD code 294 Mobile No 9828426099 Fax No 3065001 Email ID [email protected] Web site of trust/society www.pacific-university.ac.in Nearest Railway Station Udaipur Airport Dabok Details of Head of Institution Appointment letter View Name of the Head of the Institution Dr JAYESH DWIVEDI House no./ Bld. -
UNIVERSITY GRANTS COMMISSION State-Wise List of Private
UNIVERSITY GRANTS COMMISSION State-wise List of Private Universities as on 01.02.2020 S.No Name of Private University Date of Notification ARUNACHAL PRADESH 1. Apex Professional University, Pasighat, District East Siang, 10.05.2013 Arunachal Pradesh - 791102. 2. Arunachal University of Studies, NH-52, Namsai, Distt – Namsai 26.05.2012 - 792103, Arunachal Pradesh. 3. Arunodaya University, E-Sector, Nirjuli, Itanagar, Distt. Papum 21.10.2014 Pare, Arunachal Pradesh-791109 4. Himalayan University, 401, Takar Complex, Naharlagun, 03.05.2013 Itanagar, Distt – Papumpare – 791110, Arunachal Pradesh. 5. North East Frontier Technical University, Sibu-Puyi, Aalo 03.09.2014 (PO), West Siang (Distt.), Arunachal Pradesh –791001. 6. The Global University, Hollongi, Itanagar, Arunachal Pradesh. 18.09.2017 7. The Indira Gandhi Technological & Medical Sciences University, 26.05.2012 Ziro, Arunachal Pradesh. 8. Venkateshwara Open University, Itanagar, Arunachal Pradesh. 20.06.2012 S.No Andhra Pradesh 9. Bharatiya Engineering Science and Technology Innovation 17.02.2019 University, Gownivaripalli, Gorantla Mandal, Anantapur, Andhra Pradesh 10. Centurian University of Technology and Management, Gidijala 23.05.2017 Junction, Anandpuram Mandal, Visakhapatnam- 531173, Andhra Pradesh. 11. KREA University, 5655, Central, Expressway, Sri City-517646, 30.04.2018 Andhra Pradesh 12. Saveetha Amaravati University, 3rd Floor, Vaishnavi Complex, 30.04.2018 Opposite Executive Club, Vijayawada- 520008, Andhra Pradesh 13. SRM University, Neerukonda-Kuragallu Village, mangalagiri 23.05.2017 Mandal, Guntur, Dist- 522502, Andhra Pradesh (Private University) 14. VIT-AP University, Amaravati- 522237, Andhra Pradesh (Private 23.05.2017 University) ASSAM 15. Assam Don Bosco University, Azara, Guwahati 12.02.2009 16. Assam Down Town University, Sankar Madhab Path, Gandhi 29.04.2010 Nagar, Panikhaiti, Guwahati – 781 036. -

Consolidated List Private Universities
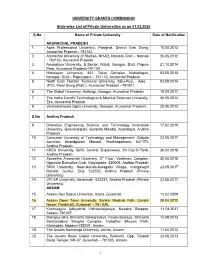
UNIVERSITY GRANTS COMMISSION State-wise List of Private Universities as on 06.08.2021 S.No Name of Private University Date of Notification ARUNACHAL PRADESH 1. Apex Professional University, Pasighat, District East Siang, 10.05.2013 Arunachal Pradesh - 791102. 2. Arunachal University of Studies, NH-52, Namsai, Distt – Namsai 26.05.2012 - 792103, Arunachal Pradesh. 3. Arunodaya University, E-Sector, Nirjuli, Itanagar, Distt. Papum 21.10.2014 Pare, Arunachal Pradesh-791109 4. Himalayan University, 401, Takar Complex, Naharlagun, 03.05.2013 Itanagar, Distt – Papumpare – 791110, Arunachal Pradesh. 5. North East Frontier Technical University, Sibu-Puyi, Aalo 03.09.2014 (PO), West Siang (Distt.), Arunachal Pradesh –791001. 6. The Global University, Hollongi, Itanagar, Arunachal Pradesh. 18.09.2017 7. The Indira Gandhi Technological & Medical Sciences University, 26.05.2012 Ziro, Arunachal Pradesh. 8. Venkateshwara Open University, Itanagar, Arunachal Pradesh. 20.06.2012 Andhra Pradesh 9. Bharatiya Engineering Science and Technology Innovation 17.02.2019 University, Gownivaripalli, Gorantla Mandal, Anantapur, Andhra Pradesh 10. Centurian University of Technology and Management, Gidijala 23.05.2017 Junction, Anandpuram Mandal, Visakhapatnam- 531173, Andhra Pradesh. 11. KREA University, 5655, Central, Expressway, Sri City-517646, 30.04.2018 Andhra Pradesh 12. Saveetha Amaravati University, 3rd Floor, Vaishnavi Complex, 30.04.2018 Opposite Executive Club, Vijayawada- 520008, Andhra Pradesh 13. SRM University, Neerukonda-Kuragallu Village, mangalagiri 23.05.2017 Mandal, Guntur, Dist- 522502, Andhra Pradesh (Private University) 14. VIT-AP University, Amaravati- 522237, Andhra Pradesh (Private 23.05.2017 University) ASSAM 15. Assam Don Bosco University, Azara, Guwahati 12.02.2009 16. Assam Down Town University, Sankar Madhab Path, Gandhi 29.04.2010 Nagar, Panikhaiti, Guwahati – 781 036. -

City Development Plan for Udaipur, 2041
City Development Plan for Udaipur, 2041 (Interim City Development Plan) June 2014 Supported under Capacity Building for Urban Development project (CBUD) A Joint Partnership Program between Ministry of Urban Development, Government of India and The World Bank CRISIL Risk and Infrastructure Solutions Limited Ministry of Urban Development Capacity Building for Urban Development Project City Development Plan for Udaipur – 2041 Interim City Development Plan June 2014 Green Lake city of India... Education hub … Hospitality centre…. Abbreviations ADB Asian Development Bank BMTPC Building Materials and Technology Promotion Council BOD Biochemical oxygen demand BPL Below Poverty line BRG Backward Regional Grant BRGF Backward Regional Grant Fund CAA Constitutional Amendment Act CAGR Compound Annual Growth Rate CAZRI Central Arid Zone Research Institute CBUD Capacity Building for Urban Development CCAR Climate Change Agenda for Rajasthan CPCB Central Pollution Control Board CST Central Sales Tax DDMA District Disaster Management Authority DEAS Double entry accounting system DLC District land price committee DPR Detailed Project Report DRR Disaster risk reduction EWS Economically weaker section GDDP Gross District Domestic Product GDP Gross Domestic Product GHG Green House Gases GIS Geo information system HRD Human Resource Development IHSDP Integrated Housing and Slum Development Programme IIM Indian Institute of Management INCCA Indian Network for Climate Change Assessment LOS Level of Services MLD Million Liter per Day NLCP National Lake Conservation -

E Souviner Final 02
AMU 1st Annual National Conference of Association for Medical Updates SOUVENIR 1st - 3 rd September 2017 Geetanjali Medical College & Hospital, Udaipur ;k dqUnsUnqrq”kkjgkj/koyk ;k ‘kqHkzoL=ko`rk ;k oh.kkon.Mef.Mrdjk ;k ‘osriùkluk ;k czgekP;qr’kadjizHk`frfHknsZo% lnk iwftrk lk eka ikrq ljLofr Hkxorh fu% ‘ks”ktkM~;kigk Organizing Committee AMU Organizing Committee Chief Patron Patron Co- Patron Co- Patron Mr. J. P. Agarwal Dr. R. K. Nahar Mr. Kapil Agarwal Mr. Ankit Agarwal Chairman, Geetanjali University Trust Vice Chancellor, Geetanjali University Vice Chairman, Geetanjali University Executive Director, GMCH Organizing Chairman Organizing Chairman Organizing Secretary Academic Incharge Dr. F. S. Mehta Dr. G. L. Dad Dr. Ashish Sharma Dr. Apurva Agrawal Organizing Joint Secretary Cultural Coordinator Souvenir Incharge Organizing Joint Secretary Dr. Arvind Yadav Dr. Savita Choudhary Dr. Lalita Jeenger Dr. Jitendra Jeenger Treasurer Workshop Coordinator Quiz Coordinator Quiz Incharge Dr. Himanshu Patel Dr. Manjinder Kaur Dr. Upasana Bhumbla Dr. Manu Sharma AMU From the Editorial desk…. Dear Friends, Colleagues, and delegates, Greetings on behalf of organizing committee Wish you all a fulfilling and academically satisfying year ahead I am glad that we have this opportunity to organize the 1st Annual Conference of Association for Medical Updates on 1st -3 rd September, 2017. I take this opportunity to welcome learned speakers, delegates and their spouse coming to Udaipur from all parts of country. The goal of this conference is to provide a forum for interchange of knowledge and updates from various branches of medical field. Researchers from different field are invited to gather and present their work amongst fellow medical professionals. -

Government of Rajasthan Departments of Higher Education F.1S (1) Edu-4/ 2006 Dated: 07 July, 2017
Government of Rajasthan Departments of Higher Education F.1S (1) Edu-4/ 2006 Dated: 07 July, 2017 To, Vice Chancellor, (State/Deemed University) President, (Private University) Subject: Instructions & application formats regarding Authentication of Degrees/ Certificates/ Diploma for Education and Employment abroad Reference: D.O. No. F.1S-1I2004-NS.II dated 08.07.2004 of Ministry of Human Resource Development & Letter No. 18-4/2004-NS-II dated 01.06.2005 and even numbered letter of Department of Higher Education dated 22.04.2016,15.07.2016 and 27.l0.2016 Sir/Madam, The Department of Higher Education authenticates degrees/diploma/certificates conferred by universities under its administrative control for Education and Employment abroad. Keeping the convenience of applicants in consideration, detailed guidelines were issued vide even numbered letter dated 22.04.2016 and were revised vide letter dated 27.10.2016. These guidelines have been further revised and are being enclosed at Annexure-I. These guidelines will be effective from 17.07.2017. Kindly direct all concerned of university to complete the formalities as per the enclosed guidelines/instruction and use only the new formats for furnishing information. ~l- Dr. Nathu Lal Suman Joint Secretary Enclosed- As above Copy for information/necessary action please- 1. SA to Hon'ble Higher Education Minister, Secretariat, Jaipur 2. PS, Secretary, Department of Higher Education, Ministry of Human Resource Development, Shastri Bhawan, New Delhi ·110 001 3. PS, ACS, Higher, Technical & Sanskrit Department, Secretariat, Jaipur 4. PS, Commissioner, College Education, Block-IV, Shiksha Sankul, JLN Marg, Jaipur 5. In-charge Website, College Education, Block-IV, Shiksha Sankul, JLN Marg, Jaipur for uploading on website of Department of College Education. -

Udaipur Royal Rajvilas
https://www.propertywala.com/udaipur-royal-rajvilas-udaipur Udaipur Royal Rajvilas - Shobghpura, Udaipur 3 & 4 BHK Villas available in Udaipur Royal Rajvilas Udaipur Royal Rajvilas presented by Udaipur Entertainment World with 3 & 4 BHK Villas available in Shobhagpura, Udaipur Project ID : J290083911 Builder: Udaipur Entertainment World Properties: Apartments / Flats, Commercial Plots / Lands Location: Udaipur Royal Rajvilas, Shobghpura, Udaipur - 313001 (Rajasthan) Completion Date: Dec, 2015 Status: Started Description Udaipur Royal Rajvilas a new residential project launch by Udaipur Entertainment World. Seven stately towers that present a panoramic view of Udaipur in all its legality offering 3 BHK & 4 BHK Luxury Apartments that will change the definition of luxury. The project is a world custom made for aristocratic obsessions. The project is surrounded by wide road network three side roads connectivity Distance of 60- 65 ft between each tower to provide for proper light and ventilation. Amenities Jogging Track Health Club Spa Senior Citizen Park Swimming pool First Aid Center Party Lawn Clubbing Lawn tennis court Half Basketball Court and children’s play-zone. Gymnasium Sauna Massage Parlor Squash and Billiard courts Library and Card room Udaipur Entertainment World is engaged in the Development - Management - Operations of Shopping Malls, Hospitality, Residential, Commercial Offices under the brand name. Udaipur Entertainment World has its fingers on the pulse of the nation. There is an imminent growth story waiting to happen in, what we like to call the Real India or the collective of the numerous non-metro emerging cities of India. We will help the Real India where most of the Indians shaping the country live. -
List of Universities Under Section 2(F) and Section 3 of the UGC Act, 1956
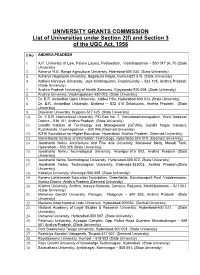
UNIVERSITY GRANTS COMMISSION List of Universities under Section 2(f) and Section 3 of the UGC Act, 1956 S.No ANDHRA PRADESH 1. A.P. University of Law, Palace Layout, Pedawaltair, Visakhapatnam – 530 017 (A. P) (State University). 2. Acharya N.G. Ranga Agricultural University, Hderabad-500 030. (State University) 3. Acharya Nagarjuna University, Nagarjuna Nagar, Guntur-522 510. (State University) 4. Adikavi Nannaya University, Jaya Krishnapuram, Rajahmundry – 533 105, Andhra Pradesh. (State University) 5. Andhra Pradesh University of Health Sciences, Vijayawada-520 008. (State University) 6. Andhra University, Visakhapatnam-530 003. (State University) 7. Dr. B.R. Ambedkar Open University, Jubilee Hills, Hyderabad-500 033. (State University) 8. Dr. B.R. Ambedkar University, Etcherla – 532 410 Srikakulam, Andhra Pradesh (State University) 9. Dravidian University, Kuppam-517 425. (State University) 10. Dr. Y.S.R. Horticultural University, PO Box No. 7, Venkataramannagudem, West Godavari District – 536 101, Andhra Pradesh. (State University) 11. Gandhi Institute of Technology and Management (GITAM), Gandhi Nagar Campus, Rushikonda, Visakhapatman – 530 045.(Deemed University) 12. ICFAI Foundation for Higher Education, Hyderabad, Andhra Pradesh. (Deemed University) 13. International Institute of Information Technology, Hyderabad-500 019. (Deemed University) 14. Jawaharlal Nehru Architecture and Fine Arts University, Mahaveer Marg, Masab Tank, Hyderabad – 500 028 (State University) 15. Jawaharlal Nehru Technological University, Anantpur-515 002, Andhra Pradesh (State University) 16. Jawaharlal Nehru Technological University, Hyderabad-500 072. (State University) 17. Jawaharlal Nehru Technological University, Kakinada-533003, Andhra Pradesh.(State University) 18. Kakatiya University, Warangal-506 009. (State University) 19. Koneru Lakshmaiah Education Foundation, Greenfields, Kunchanapalli Post, Vaddeswaram, Guntur District, Andhra Pradesh (Deemed University) 20. -

Bhamashah Award 2019 Engli
BHAMASHAH AWARD - 2019 FOR THE ACADEMIC YEAR 2018-19 S.No. Name of Applicant College/Institute Name of University Percentage B.A. 1. Ms. Deepshikha Ranawat MV Shramjeevi College JRN Rajasthan Vidhyapeeth University 81.55 Udaipur Udaipur B.A. LLB 2. Ms. Disha Bhatt National Law University National Law University 82.43 Jodhpur Jodhpur B. Pharmacy 3. Ms. Pooja Rani Pacific Academy College Pacific University 80.00 Udaipur Udaipur B.Ed. 4. Ms. Ravina Vaishnav Mateshwari T.T. College Mohan Lal Sukhadia University 84.00 Umarda, Udaipur Udaipur B. Architecture 5. Mr. Daksh Jain MBM Engineering College Jai Narayan Vyas University 79.60 Jodhpur Jodhpur B.Sc. 6. Mr. Sahil Saraswat University College of Science Mohan Lal Sukhadia University 92.14 Udaipur Udaipur B.Sc. Home Science 7. Ms. Jaya Lohar Government Girls College Mohan Lal Sukhadia University 77.78 Nathdwara Udaipur B. Sc. Biotechnology 8. Ms. Kinjal Panwar University College of Science Mohan Lal Sukhadia University 90.33 Udaipur Udaipur B.Sc. Agriculture 9. Mr. Pradeep Kumawat College of Agriculture Maharana Pratap University of 88.20 Bhilwara Agriculture and Technology Udaipur Bhamashah_Award_2019_English.docx B.Sc. Nursing 10. Mr. Girish Gurjar Shri Bapuji College Rajasthan University of Health 87.85 Nagaur and Sciences, Jaipur B.T.M. 11. Ms. Surbhi Bhavsar University College of Commerce Mohan Lal Sukhadia University 75.00 and Management Studies Udaipur Udaipur B. Tech Information Technology 12 Mr. Ali Abbas Larji Vellore Institute of Technology VIT University 98.20 Vellore Vellore BCA 13. Ms. Shalini Purohit University College of Mohan Lal Sukhadia University 93.10 Science, Udaipur Udaipur B.T.P. -

University Grants Commission
UNIVERSITY GRANTS COMMISSION Total No. of Universities in the Country as on 22.02.2017 Universities Total No. State Universities 359 Deemed to be Universities 123 Central Universities 47 Private Universities 260 Total 789 1 S.No ANDHRA PRADESH Date/Year of Notification/ Establishment 1. Acharya Nagarjuna University, Nagarjuna Nagar-522510, Dt. Guntur, Andhra 1976 Pradesh. (State University) 2. Adikavi Nannaya University, 25-7-9/1, Jayakrishnapuram, Rajahmundry – 533 2006 105, East Godavari District, Andhra Pradesh. (State University) 3. Andhra University, Waltair, Visakhapatnam-530 003, Andhra Pradesh. (State 1926 University) 4. Damodaram Sanjivayya National Law University, Plot No. 116, Sector 11 MVP 2008 Colony, Visakhapatnam – 530 017, Andhra Pradesh. (State University) 5. Dr. B.R. Ambedkar University, Etcherla, Dt. Srikakulam-532410, Andhra 2008 Pradesh. (State University) 6. Dravidian University, Srinivasanam, -517 425, Chittoor District, Andhra 1997 Pradesh. (State University) 7. Dr. Y.S.R. Horticultural University, PO Box No. 7, Venkataramannagudem, 2011 West Godavari District – 536 101, Andhra Pradesh. (State University) 8. Dr. N.T.R. University of Health Sciences (Formerly Andhra Pradesh University 1986 of Health Sciences), Vijayawada-520 008, Andhra Pradesh. (State University) 9. Gandhi Institute of Technology and Management (GITAM), Gandhi Nagar 13.08.2007 Campus, Rushikonda, Visakhapatman – 530 045, Andhra Pradesh.(Deemed University) 10. Jawaharlal Nehru Technological University, Anantpur-515 002, Andhra 2008 Pradesh (State University) 11. Jawaharlal Nehru Technological University, Pithapuram Road, Kakinada- 2008 533003, East Godvari District, Andhra Pradesh.(State University) 12. Koneru Lakshmaiah Education Foundation, Greenfields, Kunchanapalli Post, 20.02.2009 Vaddeswaram, Guntur District-522002, Andhra Pradesh. (Deemed University) 13. Krishna University, Andhra Jateeya Kalasala, Campus, Rajupeta, 2008 Machllipatanam – 521 001, Krishna District, Andhra Pradesh. -

National Level Review / Interface Meeting of NAD Scheduled on 26Th June 2018
National Level Review / Interface Meeting of NAD scheduled on 26th June 2018 Sl.No Name of Institution Amity University, Rajasthan NH-11C, 1 Kant Kalwar, Jaipur- 303 002. Bhagwant University, Post Box No. 87, 2 Sikar Road, Ajmer-305 001. Bhupal Nobles University, Maharana Pratap Station Road, Sevashram 3 Circle, Udaipur – 313001, Rajasthan. Career Point University, Kota, 4 Rajasthan. Dr. K.N. Modi University, Plot-1, RIICO Industrial Area Ph-II, Newai, Distt. 5 Tonk , Rajasthan – 304 021. Geetanjali University, Udaipur, 6 Rajasthan. Homoeopathy University, Saipura, Sanganer, Jaipur – 302 029, 7 Rajasthan. ICFAI University, Khasra No. 505/1, Village-Jamdoli, Agra Road, Jaipur – 8 302 031, Rajasthan. IIHMR University, 1, Prabhu Dayal Marg, Near Sanganer Airport, Jaipur - 9 302 029, Rajasthan. J.E.C.R.C. University, Jaipur, 10 Rajasthan. J.K. Lakshmipat University, Laliya Ka Vas, PO Mahapura, Ajmer Road, 11 Jaipur – 302 026, Rajasthan. Jagannath University, Vill.-Rampura, 12 Teshil – Chaksu, Jaipur. Jaipur National University, Jagatpura, 13 Jaipur. Jayoti Vidyapeeth Women’s University, Vedant Gyan Valley Village, Jharna Mahala, Jabner, Link Road NH-8, 14 Jaipur. Jodhpur National University, Narnadi Jhanwar Road, Jodhpur–342 15 001 Madhav University, Madhav University, “Madhav Hills”, Opp. Banas Bridge Toll, NH-14, Village-Wada/Bhujela, Panchayat Samiti – Bharja, Tehsil – Pindwara, Abu Road, District-Sirohi, 16 Rajasthan – 307026. Maharaj Vinayak Global University, 17 Jaipur, Rajasthan. Maharishi Arvind University, Mundiaramsar, Near Bindayaka Industrial Area, Jaipur-302012, 18 Rajasthan. Mahatma Gandhi University of Medical Sciences & Technology, RIICO Institutional Area, Sitapur, Tonk Road, 19 Jaipur – 302 022. Mahatma Jyoti Rao Phoole University, SP-2 &3, Kant Kalwar, RIICO Industrial 20 Area, Tala Mod, NH-I, Achrol, Jaipur Manipal University, Vatika Infotech City, Near GVK Toll Plaza, Jaipur ajmer Experss Way, Post – Thikaria, 21 Jaipur – 302 026, Rajasthan.