Visakhapatnam, India, Sanitation Assessment Final Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Studies on Coastal Geomorphology Along Visakhapatnam to Bhimunipatnam, East Coast of India M
J. Ind. Geophys. Union ( October 2012 ) Vol.16, No.4, pp. 179-187 Studies on Coastal Geomorphology along Visakhapatnam to Bhimunipatnam, East Coast of India M. Jagannadha Rao, Greeshma Gireesh A.G., P. Avatharam1, N.C. Anil2 and T. Karuna Karudu Delta Studies Institute, 1Dept of Geology, 2Dept. of Geo-Engineering, Andhra University, Visakhapatnam. ABSTRACT An attempt has been made to study and record the diverse coastal geomorphic features along Visakhapatnam – Bhimunipatnam coast. The study area is marked by geomorphic features resulted from various coastal and land ward processes. The geomorphic units under different heads namely, features formed by present day wave action, features formed due to sea level oscillations and features formed by rock and sea water interaction have been presented. The influence of sea level oscillations and land and sea interaction forms a diverse coastal geomorphology along the coast. The details of features such as beach, dune system, inter tidal deposits, red sediments, wave cut platform, marine terrace, sea stack, sea cave, serpent hood structures, promontories, wind gap and natural bridge have been recorded and the formation as well as significance of their occurrence are presented. The coastal geomorphology of the study area clearly established not only the sea level oscillations but also variations in climatic conditions in this part of the coast. INTRODUCTION PHYSIOGRAPHY Coastal geomorphology by definition is the study of The study area is characterized by Eastern Ghat the morphological development and evolution of the mobile belt. This area covered with denudational coast as it acts under the influence of winds, waves, hills of range between 30 to 594m above mean currents and sea level changes. -

NTPC Pudimadaka Public Hearing on August 12
Search GO Home Today's Paper All Sections News National International Opinion Business Sport thREAD Features Sci-Tech Entertainment Cities Bengaluru Chennai Coimbatore Delhi Hyderabad Kochi Kozhikode Kolkata Madurai Mangaluru Visakhapatnam CIT IES » VISAKHAPAT NAM VISAKHAPATNAM, July 13, 2015 Updated: July 13, 2015 05:48 IST o2 Loop Freikarte NTPC Pudimadaka public hearing on August 12 Pro- Ject Audio Shop - Plattenspieler,HiFi Geräte,Zubehör günstig, schnell & versandfrei www.yourhifi.de/pro-ject_shop Ads by Google SANTOSH PATNAIK COMMENT · PRINT · T T Tweet 0 Four coal-based units of 1,000 MW each will be set up at one place with supercritical technology The A. P. Pollution Control Board has issued a notification for holding environmental public hearing for NTPC Pudimadaka Super Thermal Power Project on August 12. The project for which NTPC has been allotted 1,200 acres by the A. P. Industrial Infrastructure Corporation at Pudimadaka, about 60 km from here in Atchutapuram and Rambilli mandals, will involve an investment of Rs.26,828 crore — the first major investment post-bifurcation. The EIA study for the project has been done by Vimta Labs of Hyderabad. The APPCB would put everything about the project on its website on Monday, Environmental Engineer R. Lakshminarayana told The Hindu . NTPC is also scouting for suitable site near Simhadri Super Thermal Power Station at Parawada to expand its capacity from 2,000 MW to 3,600 MW. Asked to comment on the project, NTPC-Pudimadaka Group General Manager P.S. Radhakrishnan said: “It will be a green power project, as the total requirement of coal will be imported to ensure higher efficiency levels and to put emissions at bare minimum.” He said the project would not need any land acquisition as the APIIC had already handed over 1,200 acres of developed area. -

(Motor Driver) on 04.09.2016
Venue-wise list of eligible candidates for the written test for the post of Technician / Technician (Motor Driver) on 04.09.2016 Easo Bhavan, Ernakulam 1. Roll No 280170123 Mylapalli Anil, D.No.16-13-7, Kotha Jalaripeta, Visakhaptnam-530001 2. Roll No 280170124 Lotla Venkata Ramana, D.No. 32-3-28, Mahalakshmi street, Bowdara Road, Visakhapatnam-530004 3. Roll No 280170125 Ganta Nagireddy, D.No. 31-23-3, Simhaladevudu street, Allipuram, Visakhaptnam-530004 4. Roll No 280170126 Lotla Padmavathi, W/o. G. Nagireddy, D.No. 31-23-3, Simhaladevudu street, Allipuram, Visakhaptnam-530004 5. Roll No 280170127 SERU GOPINADH Pallepalem Ramayapatnam Vulavapadu(m) Prakasham (d), AP-523291 6. Roll No280180001 Ram Naresh Meena Vill Post Samidhi Teh. Nainina, Dist - Bundi State Rajasthan – 323801 7. Roll No280180002 Harikeshmeena Vill Post-Samidhi Teh.Nainwa, Dist - Bundi Rajastan – 323801 8. Roll No280180003 Sabiq N.M Noor Mahal Kavaratti, Lakshadweep 682555 9. Roll No280180004 K Pau Biak Lun Zenhanglamka, Old Bazar Lt. Street, CCPur, P.O. P.S. Manipur State -795128 10. Roll No280180005 Athira T.G. Thevarkuzhiyil (H) Pazhayarikandom P.O. Idukki – 685606 11. Roll No280180006 P Sree Ram Naik S/o P. Govinda Naik Pedapally (V)Puttapathy Anantapur- 517325 12. Roll No280180007 Amulya Toppo Kokkar Tunki Toli P.O. Bariatu Dist - Ranchi Jharkhand – 834009 13. Roll No280180008 Prakash Kumar A-1/321 Madhu Vihar Uttam Nagar Newdelhi – 110059 14. Roll No280180009 Rajesh Kumar Meena VPO Barwa Tehsil Bassi Dist Jaipur Rajasthan – 303305 15. Roll No280180010 G Jayaraj Kumar Shivalayam Nivas Mannipady Top P.O. Ramdas Nagar Kasargod 671124 16. Roll No280180011 Naseefahsan B Beathudeen (H) Agatti Island Lakshasweep 17. -

LHA Recuritment Visakhapatnam Centre Screening Test Adhrapradesh Candidates at Mudasarlova Park Main Gate,Visakhapatnam.Contact No
LHA Recuritment Visakhapatnam centre Screening test Adhrapradesh Candidates at Mudasarlova Park main gate,Visakhapatnam.Contact No. 0891-2733140 Date No. Of Candidates S. Nos. 12/22/2014 1300 0001-1300 12/23/2014 1300 1301-2600 12/24/2014 1299 2601-3899 12/26/2014 1300 3900-5199 12/27/2014 1200 5200-6399 12/28/2014 1200 6400-7599 12/29/2014 1200 7600-8799 12/30/2014 1177 8800-9977 Total 9977 FROM CANDIDATES / EMPLOYMENT OFFICES GUNTUR REGISTRATION NO. CASTE GENDER CANDIDATE NAME FATHER/ S. No. Roll Nos ADDRESS D.O.B HUSBAND NAME PRIORITY & P.H V.VENKATA MUNEESWARA SUREPALLI P.O MALE RAO 1 1 S/O ERESWARA RAO BHATTIPROLU BC-B MANDALAM, GUNTUR 14.01.1985 SHAIK BAHSA D.NO.1-8-48 MALE 2 2 S/O HUSSIAN SANTHA BAZAR BC-B CHILAKURI PETA ,GUNTUR 8/18/1985 K.NAGARAJU D.NO.7-2-12/1 MALE 3 3 S/O VENKATESWARULU GANGANAMMAPETA BC-A TENALI. 4/21/1985 SHAIK AKBAR BASHA D.NO.15-5-1/5 MALE 4 4 S/O MAHABOOB SUBHANI PANASATHOTA BC-E NARASARAO PETA 8/30/1984 S.VENUGOPAL H.NO.2-34 MALE 5 5 S/O S.UMAMAHESWARA RAO PETERU P.O BC-B REPALLI MANDALAM 7/20/1984 B.N.SAIDULU PULIPADU MALE 6 6 S/O PUNNAIAH GURAJALA MANDLAM ,GUNTUR BC-A 6/11/1985 G.RAMESH BABU BHOGASWARA PET MALE 7 7 S/O SIVANJANEYULU BATTIPROLU MANDLAM, GUNTUR BC-A 8/15/1984 K.NAGARAJENDRA KUMAR PAMIDIMARRU POST MALE 8 8 S/O. -
M/S. MVV & MK HOUSING Site Address
BRIEF SUMMARY (CONSTRUCTION OF RESIDENTIAL AFFORDABLE APARTMENT ) M/s. MVV & MK HOUSING Site Address: 60-1, 59-1b, 58-3 Patta No: 61 & 62 Kurmannapalem Village, Zone –V, Ward No: 58, GVMC Limits, Visakhapatnam Office Address : Plot No 21, Near Lawsons Bay Post Office, Lawsons Bay Colony, Pedda Waltair, Visakhapatnam, Andhra Pradesh 530017 PREPARED BY SV ENVIRO LABS & CONSULTANTS ENVIRO HOUSE, B -1, BLOCK-B, IDA, AUTONAGAR, VISAKHAPATNAM Phone: 0891-2755528 Email: [email protected] Recognized by MoEF&CC, QCI Accredited S.No.141 CONCEPTUAL PLAN | 1 MAY’ 2018 1.0 INTRODUCTION M/s. MVV & MK Housing is located at Sy.No:60-1, 59-1b, 58-3, Patta no: 61 & 62, Kurmannapalem village, Zone –V, Ward no: 58, GVMC Limits, Visakhapatnam with its registered office at Plot No-21, Near Post Office, Lawson’s Bay colony, Visakhapatnam – 17. The total units under the proposed residential affordable project would be 2000 no. flats in Cellar+ Stilt + G + Upper 9 upper floors and amenities G+9 upper floors which comprise of Residential in an area of 39859.66Sq.mts or 9.849Acres. Table -1: Details about Project Site Site Location 60-1, 59-1B, 58-3 Patta no: 61 & 62, Kurmannapalem, Zone –V, Ward no: 58, GVMC Limits, Visakhapatnam Latitude 17°41'50.04"N Longitude 83° 9'57.96"E Nearest Highway AH-45 at a distance of 1.23 kms Nearest Habitation Within Kurmannapalem Nearest Airport Visakhapatnam Airport at 6.75 kms Nearest Railway station Duvvada Railway station at 1.69 Kms Marripalem Railway station – 9.96 Kms Nearest Water Bodies Kanithi Balancing Reservoir at 2.31 kms Eethapalem Cheruvu at 1.10 Kms Meghadri Gedda Reservoir at a distance of 6.98 kms from the project site. -

Preparation of Master Plan & Upgradation for Mudasarlova Park
RFP Visakhapatnam Urban Development Authority. 17TH March 2017 [SELECTION OF ARCHITECTURAL LANDSCAPE CONSULTING AGENCY FOR “PREPARATION OF MASTER PLAN & UPGRADATION FOR MUDASARLOVA PARK AS INTERNATIONAL TOURIST DESTINATION IN VISAKHAPATNAM, ANDHRA PRADESH.”] ISSUED BY: VISAKHAPATNAM URBAN DEVELOPMENT AUTHORITY ANDHRA PRADESH INDIA Selection of Consulting Agency for “Preparation of Master Planning and Upgradation of Mudasalova 1. DISCLAIMER Park, Visakhapatnam, Andhra Pradesh.” The information contained in the Request for Proposal document (“RFP”) is provided to Bidders on the terms and conditions set out in this RFP and such other terms and conditions subject to which such information is provided. The RFP is not an agreement and is neither an offer nor invitation by the Authority to the prospective Bidders or any other person. The purpose of the RFP is to provide interested parties with information that may be useful to them in the formulation of their Proposals pursuant to this RFP. The RFP includes statements, which reflect various assumptions and assessments arrived at by the Authority in relation to the Consultancy. Such assumptions, assessments and statements do not purport to contain all the information that each Bidder may require. The RFP may not be appropriate for all persons, and it is not possible for the Authority, its employees or advisers to consider the objectives, technical expertise and particular needs of each party who reads or uses the RFP. The assumptions, assessments, statements and information contained in the RFP, may not be complete, accurate, adequate or correct. Each Bidder should, therefore, conduct its own investigations and analysis and should check the accuracy, adequacy, correctness, reliability and completeness of the assumptions, assessments and information contained in the RFP and obtain independent advice from appropriate sources. -
SC / ST BACKLOG 2020 - TENTATIVE MERIT LIST of JUNIOR ACCOUNTANT DOB Belong Sl
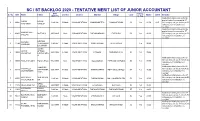
SC / ST BACKLOG 2020 - TENTATIVE MERIT LIST OF JUNIOR ACCOUNTANT DOB belong Sl. No SNO Name Father Gender District Mandal Village Caste Marks CGPA Remarks (M/D/YY) to Vsp Notification initially issued for the post of Junior Accountant in ST NISANI NISANI 1 10042 3/4/1996 FeMale VISAKHAPATNAM MAHARANIPETA GHNANAPURAM SC Yes 91.50 9.15 (W) category, as you belong to SC POORNIMA GANESH category your candidature is rejected. Notification initially issued for the post of Junior Accountant in ST GURAMPALLI 2 10401 MUTYALU 6/15/1985 Male VISHAKAPATNAM PADMANABHAM POTNURU SC Yes 90.00 (W) category, as you belong to SC SREENU category your candidature is rejected. KORABU KORABU 3 11794 YEDUKONDA 1/9/1997 FeMale VISAKHAPATNAM CHINTHAPALLI CHITHAPALLI Yes 90.00 VARDHINI LA SWAMY JARRA JARRA APPALA 4 12044 6/28/1994 FeMale VISAKHAPATNAM PADERU SUNDRUPUTTU ST Yes 89.00 VASANTHA KONDALARA O Notification initially issued for ST (W) category, as you belong to SC 5 10003 POTLA RAJESH POTLA RAJU 7/12/1995 Male VISAKHAPATNAM GOLUGONDA PAPPUSETTIAPLEM SC Yes 89.00 category your candidature is rejected. Notification initially issued for ST VAKAPALLI VAKAPALLI (W) category, as you belong to SC 6 10114 SATYANARA 6/21/1987 FeMale VISAKHAPATNAM S RAYAVARAM PETTUGOLLAPALLI SC Yes 86.00 GOVINDAMMA category your candidature is YANA rejected. Notification initially issued for ST KOTTHALA SIMHACHAL (W) category, as you belong to SC 7 10551 2/1/1988 FeMale VISAKHAPATNAM SABBAVARAM MALLUNAIDUPALEM SC Yes 85.00 VARALAKSHMI AM category your candidature is rejected. MEDA 8 11970 MEDA MADHAVI 5/20/1998 FeMale VISAKHAPATNAM. -

48434-003: Visakhapatnam-Chennai
Land Acquisition and Resettlement Due Diligence Report Document stage: Final Project Number: 48434-003 Loan and Grant Numbers: L3430; G0495 September 2018 India: Visakhapatnam-Chennai Industrial Corridor Development Program (VCICDP) - Project 1 Subproject: Development and Rejuvenation of Mudasarlova Reservoir Catchment Area Prepared by Greater Visakhapatnam Municipal Corporation, Government of Andhra Pradesh for the Asian Development Bank This due diligence report is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, Management, or staff, and may be preliminary in nature. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgments as to the legal or other status of any territory or area. CURRENCY EQUIVALENTS (as of 01 September 2018) Currency unit = Rupee (INR) INR 1.00 = USD 0.0141 USD 1.00 = INR 70.6800 ABBREVIATIONS ADB – Asian Development Bank BRTS – Bus Rapid Transit System DPR – Detailed Project Report DDR – Due diligence report DoI – Department of Industries GHG – Green House Gas GoAP – Government of Andhra Pradesh GVMC – Greater Visakhapatnam Municipal Corporation MFF – Multitranche Financing Facility PIU – Project Implementation Unit PMU – Project Management Unit R&R – Rehabilitation and Resettlement UCCRTF – Urban Climate Change Resilience Trust Fund VCICDP – Visakhapatnam Chennai Industrial Corridor Development Program CONTENTS Page I. INTRODUCTION 1 A. Background 1 B. Scope of this report 1 II. SUBPROJECT DESCRIPTION 2 A. Proposed components 2 III. FIELD WORK AND CONSULTATION 4 A. -

ROADS & BUILDINGS DEPARTMENT From
ROADS & BUILDINGS DEPARTMENT From : To Sri M.Venugopala Rao The Chief Engineer, (R&B), M.Tech. M.D., APRDC Superintending Engineer (R&B) Errummunzil, Seethammadhara, Andhra Pradesh, Visakhapatnam – 530 013, Hyderabad. e-mail : [email protected] Fax : 0891-2553265 Lr.No.3042/AP second Highway Report/2005, dated: 10 -12-2005. Sir, Sub:- A. P. Second Highway Project-Justification for qualifying the roads- Particulars submitted-Reg. Ref:- 1. Circular Memo.No.AP SM.II/RR/GM.I/2002 dt.29.11.2005 of Chief Engineer(R&B) & M.D.,APRDC, Hyderabad ### I submit herewith the particulars in the prescribed Proforma (a) to (k) of roads identified under Ist phase of A.P. Second High way Project pertaining to (R&B) circles (i) Visakhapatnam (ii) Vizianagaram (iii) Srikakulam for favour of taking further necessary action. Yours faithfully Sd/- Superintending Engineer(R&B) Visakhapatnam Encl: Project Report for For six roads along With maps and combined map INDEX S.No Name of the Road Page No. 1 Narsipatnam-Sabbavaram-Kottavalasa- 1 to 6 Vizianagaram-Palakonda-Haddubangi 2 Polavaram-Narsipatnam-Tallapalem 7 to 9 3 Calingapatnam-Parlakhemudi 10 to 11 4 Nrsipatnam-Devipatnam 12 to 13 5 Anakapalli-Anandapuram 14 to 15 6 Kakinada - Polamanipeta,Venkatanagaram- 16 to 19 Pentakota-Pudimadaka-Atchutapuram- Gajuwaka-Visakhapatnam(Item 7 of C E.Circular dt.24.11.05) 7 Combined Map 20 1) NARSIPATNAM- SABBAVARAM- KOTHAVALASA - VIZIANGARAM- PALAKONDA-HADDUBANGI ROAD A.P. SECOND HIGHWAY PROJECT - PARTICULARS ON ROADS Pavement Traffic values Constraints Classifica- Land Pavement Road Sections Distances from Major river and in terms of S. regarding tion of Homogeneous part of road/ acquisition roughness sections Name of the Road requiring four NH or improved crossings/ ROBs/ shoulder Commercial No. -

Annexure to Trade Notice No. 01/2017 (General No
Annexure to Trade Notice No. 01/2017 (General No. 1/2017) Dated. 21.06.2017 issued from F.No. V/39/16/2017-CC(VZ)Estt.P.F.I ANNEXURE - I Visakhapatnam Zone : Visakhapatnam Commissionerate and Kakinada Sub-Commissionerate No. of Sl.No. Commissionerate Name Jurisdiction Divisions Divisions This Commissionerate will have the jurisdiction over (i) Visakhapatnam North Visakhapatnam Srikakulam, Vizianagaram, (ii) Visakhapatnam Central 01 4 Commissionerate Visakhapatnam & East Godavari (iii) Visakhapatnam South Districts of Andhra Pradesh (iv) Vizianagaram Division State Kakinada Sub- This Sub-Commissionerate will (i) Kakinada Division Commissionerate have the jurisdiction over East 02 2 (ii) Rajamahendravaram (stationed at Rajamahendravaram) Godavari District of Andhra (Under Visakhapatnam Division Commissionerate) Pradesh State Page 1 of 13 Annexure to Trade Notice No. 01/2017 (General No. 1/2017) Dated. 21.06.2017 issued from F.No. V/39/16/2017-CC(VZ)Estt.P.F.I Sl. GST Division Name Jurisdiction No. of Ranges Ranges No. (i) Bheemunipatnam This Division will have jurisdiction over GVMC (Greater (ii) Madhurawada Visakhapatnam Municipal Corporation) ward Nos. 1 to 19 & (iii) Muvvalavanipalem Bheemunipatnam, Padmanabham & Anandapuram Mandals (iv) Maddilapalem Visakhapatnam (v) Akkayyapalem 01 of Visakhapatnam District. This Division will also have 10 North (vi) Seethammapeta residuary jurisdiction over any other area which is not (vii) Dwarakanagar mentioned or existing in any division under Visakhapatnam (viii) Srinagar District. (ix) Aseelmetta -

Quarantine Centre - Andhra Pradesh
QUARANTINE CENTRE - ANDHRA PRADESH Room rate(includi Contact Name of Number of ng meals Person(government Contact District: Type: Hotel/Quarantine Center: Rooms and taxes): Contact Number: offcial in-charge) Number: Remarks: VISAKHAPATNAM On Gratis Vikas Junior College Category Category 1:0 9052782060 Dr. Padma Priya 9052782060 1:74 VISAKHAPATNAM On Gratis Viajaya Residency Category Category 1:0 6300538289 Dr.Satyanarayana 6300538289 1:38 VISAKHAPATNAM On Payment The Park Hotel Category Category 9849121197 Anitha 9000782783 Single Occupancy for 14 1:20 1:35000 days VISAKHAPATNAM On Payment TAJ GATEWAY Category Category 7892142134 Anitha 9000782783 Single Occupancy for 14 1:40 1:35000 days VISAKHAPATNAM On Gratis Srikanth Lodge Category Category 1:0 9100064946 B.Ravikumar 9100064946 1:20 VISAKHAPATNAM On Gratis Sri Sai Brundavan grand Category Category 1:0 6300538289 Dr.Satyanarayana 6300538289 inn 1:28 VISAKHAPATNAM On Gratis SRI PALIMAR Category Category 1:0 9441207504 Dr.SUJATHA 9441207504 1:24 VISAKHAPATNAM On Gratis Post Metric Hostel G) Category 1:8 Category 1:0 9676376031 SDr.S.Vinnila 9676376031 VISAKHAPATNAM On Gratis NARAYANA IIT GIRLS Category Category 1:0 8985356024 Dr.Rajesh Naidu 8985356024 CAMPUS BLOCK 1) 1:140 VISAKHAPATNAM On Gratis Narayana IIT Category Category 1:0 8332954588 Dr.Amaleswari 8332954588 1:92 VISAKHAPATNAM On Gratis NARAYANA CAMPUS Category Category 1:0 9966994015 Dr.Dhanalakshmi 9966994015 1:93 VISAKHAPATNAM On Payment MEGHALAYA Category Category 8008200120 Anitha 9000782783 Single Occupancy for 14 1:45 -

Effect of Flyash on Compaction Characteristics of Expansive Soils, Near Anandapuram, Visakhapatnam, Andhra Pradesh, India
International Journal of Engineering Research & Technology (IJERT) ISSN: 2278-0181 Vol. 4 Issue 03, March-2015 Effect of FlyAsh on Compaction Characteristics of Expansive Soils, Near Anandapuram, Visakhapatnam, Andhra Pradesh, India Sudheer Choudari1 Y. Bhargava Gopi Krishna 2 1 Research Scholar, 2 Assistant Manager(Engineering), Department of Civil Engineering, Larsen & Turbo, Andhra University, Visakhapatnam. Chennai,India. Abstract: - In the present Investigation, an attempt has been 2. IDENTIFICATION OF THE PROBLEM made to assess the changes in the strength characteristics of The black cotton soils are highly argillaceous and expansive soils such as optimum moisture content, maximum contain clay fraction varying between 50 – 70 %. The high dry density, cohesion, angle of internal friction due to addition percentage of clay content with predominant of flyash in different proportions. The results indicate that the montmorillonite mineral is responsible for high volumetric flyash has a noticeable influence on the strength characteristics of expansive soils with addition of flyash. changes during wetting and drying. These volume changes cause huge damages to almost all civil engineering 1. INTRODUCTION: structures resting on / in them. 1.1Expansive Soils: The problems associated with these soils are Expansive soils are well known by the term black heave, cracks in lightly loaded building foundations, cotton soils in India and they cover almost one fifth to one pavements, earth retaining structures and canal linings. sixth of the total area. These expansive soils are colloidal Inadequate bearing capacity and differential settlements are soils containing two micron clay fraction varying between 50 not true causes of foundation failure in such soils, but high to 70% consisting of significant portion of montmorillonite swelling pressure and differential heaves are the causes.