Athletes with Disability Handbook 2009
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Disability Classification System
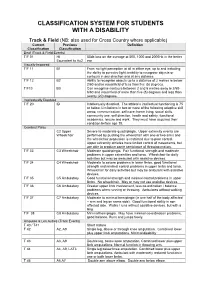
CLASSIFICATION SYSTEM FOR STUDENTS WITH A DISABILITY Track & Field (NB: also used for Cross Country where applicable) Current Previous Definition Classification Classification Deaf (Track & Field Events) T/F 01 HI 55db loss on the average at 500, 1000 and 2000Hz in the better Equivalent to Au2 ear Visually Impaired T/F 11 B1 From no light perception at all in either eye, up to and including the ability to perceive light; inability to recognise objects or contours in any direction and at any distance. T/F 12 B2 Ability to recognise objects up to a distance of 2 metres ie below 2/60 and/or visual field of less than five (5) degrees. T/F13 B3 Can recognise contours between 2 and 6 metres away ie 2/60- 6/60 and visual field of more than five (5) degrees and less than twenty (20) degrees. Intellectually Disabled T/F 20 ID Intellectually disabled. The athlete’s intellectual functioning is 75 or below. Limitations in two or more of the following adaptive skill areas; communication, self-care; home living, social skills, community use, self direction, health and safety, functional academics, leisure and work. They must have acquired their condition before age 18. Cerebral Palsy C2 Upper Severe to moderate quadriplegia. Upper extremity events are Wheelchair performed by pushing the wheelchair with one or two arms and the wheelchair propulsion is restricted due to poor control. Upper extremity athletes have limited control of movements, but are able to produce some semblance of throwing motion. T/F 33 C3 Wheelchair Moderate quadriplegia. Fair functional strength and moderate problems in upper extremities and torso. -

Concussion in Para Athletes (Kissick)
International Paralympic Committee Concussion in Para athletes Jamie Kissick, IPC Medical Committee March 8, 2018 Athletes and concussion: 6000+ Athletes with disability and concussion: 60 How to recognize the moods of an Irish Setter Van Mechelen W, Hlobil H, Kemper HC. Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Med 1992 Aug 14(2): 82-89 2012 London Paralympics Willick et al (BJSM 2013) 14/633 injuries to head and face 2.2 % 2010 Vancouver Paralympics Webborn et al (CJSM 2012) Sledge hockey: 118 athletes, 40 presented re injury, 2 head injuries (not defined specifically as concussion) Alpine: 194 athletes, 42 presented re injury, 3 new head injuries Nordic: 140 athletes, 26 presented re injury, 1 concussion 2014 Sochi Paralympics Derman et al (BJSM, 2016) Head, face and neck injuries 31/174 injuries 26/134 athletes with an injury (4.8 %) Incidence rate (IR) 4.7 injuries/1000 athlete days Rio 2016 Paralympic Games Injuries Football 5-a-side 25 High risk for collisions resulting in concussion No concussions reported 20 15 10 5 0 AT SW WB TT JU F7 F5 PO SV WR CY WF AR WT SH SA RO TR GO CA EQ BO % injury injury IR @CheriBlauwetMD Concussions in wheelchair basketball Wessels et al (Arch Phys Med Rehab 2012) 263 US wheelchair basketball players aged 18-60 6.1 % of players reported concussion in 09-10 season 44 % did not report to team staff 67 % of these because they did not want to be removed 50 % did not know it was a concussion Females had 2.5X higher concussion rate, but limited number of females Regular wheelchair users had less concussions Safety concerns in ice sledge hockey Hawkeswood et al (IJSPT 2011) Safety concerns in ice sledge hockey Hawkeswood et al (IJSPT 2011) Safety concerns in ice sledge hockey Hawkeswood et al (IJSPT 2011) SCAT5 Challenges SCAT5 Challenges Injury prevention The “3E” model Education Engineering Enforcement “OK, Mr Dittmars, remember that brain is only a temporary, so don’t think too hard with it.” Thank you! Photos ©: Getty Images . -

2018 Jessica Uniack Beach to Bay Race Long Beach Yacht Club
2018 Jessica Uniack Beach to Bay Race Long Beach Yacht Club Results for 2018 Jessica Uniack Beach to Bay Race CFJ Class Sailed: 1, Discards: 0, To count: 1, Entries: 25, Scoring system: Appendix A Class SailNo Club HelmName CrewName R1 Total Nett CFJ HHSF Jack Haliday Nicholas Ridout CFJ HHSF Trae Sanchez Ben Hagadorn CFJ LBYC 7 LBYC Nicky Lech Kai Bramble 1.0 1.0 1.0 CFJ 22 ABYC Nicholas Muller Ulises Lewis 2.0 2.0 2.0 CFJ LBYC 10 LBYC Preston Woodworth Alex Lech 3.0 3.0 3.0 CFJ 43 ABYC Summer Drake Paige Odell 4.0 4.0 4.0 CFJ 23 ABYC Nikhil Stewart Jamarcus Parker 5.0 5.0 5.0 CFJ 42 ABYC Sean colley Thomas Dobson 6.0 6.0 6.0 CFJ 44 ABYC Nicolas Sanchez Nicole Morikawa 7.0 7.0 7.0 CFJ 24 ?? 8.0 8.0 8.0 CFJ 0 HHSF Trae Sanchez Ben H 9.0 9.0 9.0 CFJ LBYC 2 LBYC Kyer Fox Isaure Chalandon 10.0 10.0 10.0 CFJ LBYC 9 LBYC Sawyer Bambam-Moak Katin Cathey 11.0 11.0 11.0 Class SailNo Club HelmName CrewName R1 Total Nett CFJ 46 ABYC Elisabeth Rossbach Troy Davidson 12.0 12.0 12.0 CFJ 00 HHSF Jack Haliday Nicholas 13.0 13.0 13.0 CFJ 41 ABYC Michael Colley Emilia Anctil 14.0 14.0 14.0 CFJ 6161 DPYC Riley Lenthall 15.0 15.0 15.0 CFJ 9PYSF HHYC Jack Busche Nolan Davis 16.0 16.0 16.0 CFJ 1510 DPYC Ryan Brown Colin Sekerka 17.0 17.0 17.0 CFJ 5151 DPYC Christopher Andersen Hunter Laws 18.0 18.0 18.0 CFJ LBYC 3 LBYC Luke Bramble Rio Dumont 19.0 19.0 19.0 CFJ LBYC 5 LBYC Jack Snow Reese Lapham 26.0 DSQ 26.0 26.0 CFJ 6161 DPYC Carsen Lenthall 26.0 DNC 26.0 26.0 CFJ 6161 DPYC Riley Lenthall 26.0 DNC 26.0 26.0 CFJ 5151 DPYC Hunter Laws Christopher Anderson -

Presenting the Paralympics: Affective Nationalism and the 'Able-Disabled'
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Bournemouth University Research Online (Re-)presenting the Paralympics: Affective Nationalism and the 'able-disabled' Emma Pullen, Daniel Jackson and Michael Silk Communication & Sport (2019, in press) *To cite this article: Pullen, E., Jackson, D., and Silk, M. (2019). (Re-)presenting the Paralympics: Affective Nationalism and the 'able-disabled'. Communication & Sport Corresponding author: [email protected] Abstract The relationship between media, sport, nations and nationalism is well established, yet, there is an absence of these discussions at the intersection of communication, Paralympics and disability studies. This omission is particularly significant considering the rapid commodification of the Paralympic spectacle, exacerbated by the entry of Channel 4 (C4) as the UK Paralympic rights holders, that has seen the games become an important site of disability (re-)presentation. In this article, we focus on the construction of national, normative, disabled bodies in Paralympic representation drawn from an analysis of three integrated datasets from Channel 4’s broadcasting of the Rio 2016 Paralympics: interviews with C4 production and editorial staff; quantitative content analysis, and qualitative moving image analysis. We highlight the strategic approach taken by C4 to focus on successful medal winning athletes; the implications this has on the sports and disability classifications given media coverage; and the role of affective high-value production practices. We also reveal the commercial tensions and editorial decisions that broadcasters face with respect to which disabilities / bodies are made hyper-visible - and thereby those which are marginalized - as national disability sport icons that inculcate preferred notions of disability and the (re)imagined nation. -

Outstanding Performances at the Viii Paralympic Games
Paralympic Games The opening ceremony was OUTSTANDING PERFORMANCES a breathtaking celebration of Paralympic sport based on the AT THE VIII PARALYMPIC GAMES Games' theme "Awaken the Mind - Free the Body - Inspire the Spirit". Actor Louis Gossett Jr.'s narration he extinguishing of the the position of a watch hand. "Go 11 by Susanna Reiff* based on this motto reached a high Olympic flame in Salt Lake and up, up, up," one can hear a point when Rudy Garcia-Tolson, a TCity was an emotional guide shout on the cross-country 13 year-old boy who has lost both of moment. "It's all over now," is what track. In biathlon competitions, visu his legs and competes in triathlon, many felt. But that was not quite true ally impaired athletes use an spoke about his dream of participat as the second part of the Salt Lake acoustic rifle system, which allows ing in the 2004 Paralympics in 2002 celebrations was yet to come: them to adjust the rifle aim according Athens. "My spirit thinks I'm a regu the VIII Paralympic Winter Games. to audio cues heard through a head lar boy - and an athlete," said Immediately after the end of the set. As the athlete aims the rifle Garcia-Tolson. "My spirit soars." Eric Olympic events the crucial transition towards the target, the frequency of Weihenmeyer, the first blind man to period began for the Salt Lake the sound signal increases. The successfully climb Mount Everest Organizing Committee (SLOC). The Paralympic version of ice hockey is carried the Paralympic torch to a Olympic Village was transformed into played on sledges and is therefore podium - guided by his dog - to then the Paralympic Village, called ice sledge hockey. -

Marelli D6C & D5C ATEX Motor Technical Catalogue
Motors for This catalogue refers to ATEX Motors belonging to Group I Category M2 and Group II Category 2G, 2D, 2GD as described. STANDARDS ® BEARINGS Hazardous Areas The ATEX Motors described in this catalogue are manufactured in accordance with IEC 60034-1-5-6-7-8-9-12-14, IEC 60072-1, EN 50347, EN 60079- D5, D6 SERIES Frame Size (mm) D - end N - end Frame Size Poles B 3 V 1 MarelliMotori 0-1-7, EN 61241-0-1. 71* 6202-2Z 6202-2Z D - end N - end D - end N - end I M2, II 2G, II 2D EUROPEAN DIRECTIVES 355-400 2 6217-C3 6217-C3 6217-C3 7217 B 80* 6204-2Z 6204-2Z Ex d/de I, Ex d/de IIB, Ex tD A21 IP65 Title Directive 90* 6205-2Z 6205-2Z 355 4 NU222-C3 6217-C3 NU222-C3 6217-C3 + 7217 B Equipment and protective system intended for use in potentially explosive atmospheres (ATEX) 94/9/EC 100* 6206-2Z 6206-2Z 400 4 NU222-C3 6222-C3 NU222-C3 6222-C3 + 7222 B Electromagnetic Compatibility (EMC) 2004/108/IEC 112* 6206-2Z 6206-2Z Low Voltage Directive (LVD) 2006/95/EC 132* 6308-2Z 6308-2Z HEADQUARTERS ITALIAN OFFICES Machinery Directive (MD) 98/37/EC 160 - 180M 6310-Z-C3 6209-Z-C3 Marelli Motori S.p.A. Milan CERTIFICATES 180L 6310-Z-C3 6210-Z-C3 Via Sabbionara, 1 Via Cesare Cantù, 29 200 6312-Z-C3 6210-Z-C3 Frame size Number Temperature Limits 36071 Arzignano (VI) Italy 20092 Cinisello Balsamo (MI) Italy 225 6313-Z-C3 6213-Z-C3 71-132 BVI 08 ATEX 0001 -20°C +40°C* 160-315 CESI 02 ATEX 071 -20 C +40 C* 250 6314-Z-C3 6213-Z-C3 (T) +39.0444.479711 (T) +39.02.660.131.66 ° ° These tables describe the bearing types used in standard configurations. -
The Use of Next Generation Sequencing to Study the Environmental Mycobiome and Its Potential Health Effects
The use of next generation sequencing to study the environmental mycobiome and its potential health effects Emma Marczylo Bioaerosols – June 2017 Overview • Brief Background: • Why are CRCE interested in fungal bioaerosols? • Mycobiome analysis: • Why use next generation sequencing? • Ongoing work • What is the current focus of CRCE’s bioaerosol research? 2 Bioaerosols – June 2017 Why bioaerosols? • Respiratory health/toxicology a big focus within our department & bioaerosols represent a current respiratory health concern 3 Bioaerosols – June 2017 Why bioaerosols? • Common sources relevant to public health 4 Bioaerosols – June 2017 Why bioaerosols? • Public concern over health effects of living near composting and intensive farming sites • Systematic reviews on exposures and health outcomes related to bioaerosol emissions from composting facilities (published 2015*) or intensive farming (ongoing) in collaboration with SAHSU • Evidence on both exposure assessment and health effects are limited • A big unknown is the microbial composition of such bioaerosols *Pearson et al, 2015, J Toxicol Environ Health B Crit Rev,18:43-69 5 Bioaerosols – June 2017 Why fungi? Normally die rapidly due to water evaporation, although increased humidity and clumping can prolong survival • Can remain viable for much longer periods, even at low humidity & high/low temperatures • Much less known about the fungal composition of bioaerosols (and other samples) • Fungi linked with development and exacerbation of asthma symptoms 6 Bioaerosols – June 2017 Mycobiome -

Framework for In-Field Analyses of Performance and Sub-Technique Selection in Standing Para Cross-Country Skiers
sensors Article Framework for In-Field Analyses of Performance and Sub-Technique Selection in Standing Para Cross-Country Skiers Camilla H. Carlsen 1,*, Julia Kathrin Baumgart 1, Jan Kocbach 1,2, Pål Haugnes 1 , Evy M. B. Paulussen 1,3 and Øyvind Sandbakk 1 1 Centre for Elite Sports Research, Department of Neuromedicine and Movement Science, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology, 7491 Trondheim, Norway; [email protected] (J.K.B.); [email protected] (J.K.); [email protected] (P.H.); [email protected] (E.M.B.P.); [email protected] (Ø.S.) 2 NORCE Norwegian Research Centre AS, 5008 Bergen, Norway 3 Faculty of Health, Medicine & Life Sciences, Maastricht University, 6200 MD Maastricht, The Netherlands * Correspondence: [email protected]; Tel.: +47-452-40-788 Abstract: Our aims were to evaluate the feasibility of a framework based on micro-sensor technology for in-field analyses of performance and sub-technique selection in Para cross-country (XC) skiing by using it to compare these parameters between elite standing Para (two men; one woman) and able- bodied (AB) (three men; four women) XC skiers during a classical skiing race. The data from a global navigation satellite system and inertial measurement unit were integrated to compare time loss and selected sub-techniques as a function of speed. Compared to male/female AB skiers, male/female Para skiers displayed 19/14% slower average speed with the largest time loss (65 ± 36/35 ± 6 s/lap) Citation: Carlsen, C.H.; Kathrin found in uphill terrain. -
Field Indicators of Hydric Soils
United States Department of Field Indicators of Agriculture Natural Resources Hydric Soils in the Conservation Service United States In cooperation with A Guide for Identifying and Delineating the National Technical Committee for Hydric Soils Hydric Soils, Version 8.2, 2018 Field Indicators of Hydric Soils in the United States A Guide for Identifying and Delineating Hydric Soils Version 8.2, 2018 (Including revisions to versions 8.0 and 8.1) United States Department of Agriculture, Natural Resources Conservation Service, in cooperation with the National Technical Committee for Hydric Soils Edited by L.M. Vasilas, Soil Scientist, NRCS, Washington, DC; G.W. Hurt, Soil Scientist, University of Florida, Gainesville, FL; and J.F. Berkowitz, Soil Scientist, USACE, Vicksburg, MS ii In accordance with Federal civil rights law and U.S. Department of Agriculture (USDA) civil rights regulations and policies, the USDA, its Agencies, offices, and employees, and institutions participating in or administering USDA programs are prohibited from discriminating based on race, color, national origin, religion, sex, gender identity (including gender expression), sexual orientation, disability, age, marital status, family/parental status, income derived from a public assistance program, political beliefs, or reprisal or retaliation for prior civil rights activity, in any program or activity conducted or funded by USDA (not all bases apply to all programs). Remedies and complaint filing deadlines vary by program or incident. Persons with disabilities who require alternative means of communication for program information (e.g., Braille, large print, audiotape, American Sign Language, etc.) should contact the responsible Agency or USDA’s TARGET Center at (202) 720-2600 (voice and TTY) or contact USDA through the Federal Relay Service at (800) 877-8339. -

Supporting Information Modular Control of L-Tryptophan Isotopic Substitution Via an Efficient Biosynthetic Cascade
Electronic Supplementary Material (ESI) for Organic & Biomolecular Chemistry. This journal is © The Royal Society of Chemistry 2020 Supporting Information Modular Control of L-Tryptophan Isotopic Substitution via an Efficient Biosynthetic Cascade Thompson, C. M.; McDonald, A. D.; Yang, H.; Cavagnero, S.*; Buller, A. R.* Department of Chemistry, University of Wisconsin-Madison 1101 University Avenue Madison, WI 53706 *corresponding authors: Andrew R. Buller, email:[email protected]; Silvia Cavagnero, email: [email protected] Table of contents 1. General information 2 2. Experimental section 2 2.1 Materials 2 2.2 Methods 2 2.2.1 Cloning, expression, and purification of PfTrpB2B9 and TmLTA 2 2.2.2 Optimization of TmLTA-TrpB2B9 cascade 3 2.2.3 Preparative-scale synthesis of Trp isotopologs 4 2.2.4 Analytical- and preparative-scale chromatography 5 2.2.5 Determination of enantiopurity of Trp isotopologs 5 2.2.6 NMR analysis 6 3. Characterization of Trp and Trp isotopologs 7 4. Supporting references 10 5. Supporting tables and figures 11 - 17 − 1 − 1. General information The glassware used in the reactions carried out in this work was thoroughly washed, and all experiments were executed following necessary safety precautions. Evaporation of solvents was performed at reduced pressure using a rotary evaporator. Electronic-absorption measurements were done with a UV-2600 spectrophotometer (Shimadzu). 2. Experimental section 2.1. Materials Chemicals and solvents were obtained from commercial suppliers and used without further 13 purification: formaldehyde-D2 (Cambridge Isotope Laboratories, Inc.); (2- C)glycine (Cambridge Isotope Laboratories, Inc.); D2O 99.9% (Sigma-Aldrich); indole (Sigma- Aldrich); pyridoxal 5’ monophosphate; (Sigma-Aldrich) L-serine (Sigma-Aldrich). -

The Impact of Lower-Limb Prosthetic Limb Use in International C4 Track Para-Cycling
The impact of lower-limb prosthetic limb use in international C4 track para-cycling An investigation was undertaken to ascertain any impact or significance of athletes within the C4 paracycling classification between those who use a lower- limb prostheses and those who do not. A statistical evaluation of event completion time was undertaken to assess C4 cyclists when competing at the World Championships and the Paralympic Games in the 1km track time trial. The C4 athletes who utilise a prostheses consistently outperformed non-amputees in the C4 classification from 2011-2016 on a competition-to-competition basis. However, when the participations were grouped as a whole together and an identified outlier athlete was removed, it was then demonstrated that there was no statistical significance between those who required the use of a lower-limb prostheses to those that did not when either evaluated on a competition-by- competition or on an amputee and non-amputee group-by-group basis (P=>0.05). As a result, this study proposes that those requiring the use of lower-limb prostheses are neither advantaged nor disadvantaged in the C4 classification category when competing in the 1km time trial at this time. Implications for Rehabilitation • This analysis indicates that at this time, there is no evidence to suggest that use of such technology is advantageous in this category or should be seen as controversial. • The design of lower-limb prosthetic limb technology in cycling should continue to be developed and optimized unabated. • This study begins to address the cited lack of peer reviewed information regarding paracycling with limb absence available to practitioners. -
HC Core Training & Stretching Manual
Sledge Hockey core Training & STreTcHing Manual INTRODUCTION Sledge hockey is a fast-paced, aggressive sport which is extremely demanding physically. In order to play the sport at the elite level, excellent physical conditioning is required. Even playing the sport recreationally, a strong level of conditioning will allow the participant to succeed and enjoy their experience more. Due to the nature of the sport, strength in the body’s core is of particular importance. This manual is designed in order to give sledge hockey players and coaches a resource to use in order to improve their own core strength and help them enjoy and achieve a higher level of success in the sport of sledge hockey. The activities described in this manual are designed specifically with sledge hockey players in mind. However, these activities may also prove useful to other disabled and able-bodied sports. For more information about sledge hockey visit www.hockeycanada.ca/sledgehockey. TABLE OF CONTENTS Beginner ...................................................................................................................1 Seated Sledge Position .........................................................................................2 Seated Lateral Tilts .............................................................................................3 Seated Side Touches ............................................................................................4 Seated Ball Rotations ...........................................................................................5