Whitehall Booklet
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Strand Walk Lma.Pdf
LGBTI HERITAGE WALK OF WHITEHALL Trafalgar’s Queer • In a 60 minute walk from Trafalgar Square to Aldwych you’ll have a conversation with Oscar Wilde, meet a transsexual Olympian, discover a lesbian ménage a trois in Covent Garden, find a transgender traffic light, walk over Virginia Woolf, and learn about Princess Seraphina who was less of a princess and more of a queen. • It takes about an hour and was devised and written by Andy Kirby. Directions – The walk starts at the statue This was the site of the Charing Cross, one of of King Charles I at the south side of the Eleanor Crosses commemorating Edward I’s Trafalgar Square. first wife. The replica is outside Charing Cross Station. Distances from London are measured here, where stood the pillory where many gay men were locked, mocked and punished. The Stop 1 – Charing Cross picture is of a similar incident in Cheapside. On 25 September 2009 Ian Baynham died following a homophobic attack in the square. Joel Alexander, 20, and Ruby Thomas, 19, were imprisoned for it. Directions – Walk to the front of the National At the top of these steps in the entrance to the Gallery on the north side of Trafalgar Square National Gallery are Boris Anrep’s marble mosaics directly in front of you. laid between 1928 and 1952. Two lesbian icons are the film star Greta Garbo as Melpomene, Muse of Stop 2 – National Gallery & Portrait Gallery Tragedy and Bloomsbury writer Virginia Woolf wielding an elegant pen as Clio, Muse of History. To the right of this building is the National Portrait Gallery with pictures and photographs of Martina Navratilova, K D Lang, Virginia again, Alan Turing, Harvey Milk and Joe Orton. -

London View Management Framework SPG MP26
26 Townscape View: St James’s Park to 219 Horse Guards Road 424 The St James’s Park area was originally a marshy water meadow, before being drained to provide a deer park for Henry VIII in the sixteenth century. The current form of the park owes much to Charles II, who ordained a new layout, incorporating The Mall, in the 1660s. The park was remodelled by John Nash in 1827-8 and his layout survives largely intact. St James’s Park is maintained to an extremely high standard and the bridge across the lake provides a frequently visited place from which to appreciate views through the Park. The landscape is subtly lit after dark. St James’s Park is included on English Heritage’s Register of Parks and Gardens of Special Historic Interest at Grade I. 425 There is one Viewing Location at St James’ Park 26A, which is situated on the east side of the bridge over the lake. 220 London View Management Framework Viewing Location 26A St James’s Park Bridge N.B for key to symbols refer to image 1 Panorama from Assessment Point 26A.1 St James’s Park Bridge – near the centre of the bridge 26 Townscape View: St James’s Park to Horse Guards Road 221 Description of the View 426 The Viewing Location is on the east side of the footbridge Landmarks include: across the lake. The bridge was built in 1956-7 to the designs Whitehall Court (II*) of Eric Bedford of the Ministry of Works. Views vary from Horse Guards (I) either end of the bridge and a near central location has been The Foreign Office (I) selected for the single Assessment Point (26A.1) orientated The London Eye towards Horse Guards Parade. -

The Ghost Bus Tour Route Record
APPENDIX A: LONDON SERVICE PERMIT LSP0666 THE GHOST BUS TOUR ROUTE RECORD Effective from 31 July 2017 STREETS TRAVERSED Route 1: From/to Northumberland Avenue via City Northumberland Avenue (westbound), Charing Cross, Whitehall (southbound), Parliament Street (southbound), Parliament Square (east, south, west and north sides), Parliament Street (northbound), Whitehall (northbound), Charing Cross, Strand, Aldwych, Drury Lane, Russell Street, Catherine Street, Aldwych, Fleet Street, Fetter Lane, New Fetter Lane, Holborn Circus, Holborn Viaduct, Giltspur Street (northbound), West Smithfield, Giltspur Street (southbound), Newgate Street, King Edward Street, Angel Street, St Martins le Grand, Cheapside, Poultry, Mansion House Street, King William Street, Monument Street, Fish Street Hill, Lower Thames Street, Byward Street, Tower Hill, Tower Bridge Approach, Tower Bridge, Tower Bridge Road, Tooley Street, Duke Street Hill, Borough High Street, Southwark Street, Blackfriars Road, Blackfriars Bridge, Victoria Embankment, Northumberland Avenue. Alternative route As main route to Fleet Street at Fetter Lane, then continue via Fleet Street, Ludgate Circus, Ludgate Hill, St Paul’s Churchyard, Cannon Street, Queen Victoria Street, Mansion House Street, then as main route. Route 2: From/to Northumberland Avenue via West End Northumberland Avenue (westbound), Charing Cross (circumnavigate King Charles Island), Northumberland Avenue (eastbound), Victoria Embankment (southbound), Horseguards Avenue, Whitehall, Charing Cross, Trafalgar Square (south side), -

Legal Notices a Copy of the Petition Will Be Supplied by the Under- the COMPANIES ACT 1948 Signed on Payment of the Prescribed Charge
THE LONDON GAZETTE, SlsT MARCH 1981 4659 VALE ROYAL DISTRICT COUNCIL Copies of the Order, statement of reasons and relevant plans may be inspected free of charge, at all reasonable HIGHWAYS ACT 1980, SECTION 14 hours from 31st March to 16th May 1981 at the Council The District of Vale Royal (Northwich Internal By-Pass Offices, Church Street, Northwich, the Council Offices, A 559 Chesterway Phase III Classified Road) (Side Roads) Whitehall, School Lane, Hartford and also at the Depart- Order 1981. ment of Transport, North-West Region, Sunley Buildings. Notice is hereby given that the Vale Royal District Council Piccadilly Plaza, Manchester. hereby give notice that they have made and submitted Any person wishing to make representations or objections to the Secretary of State for the Enviroment and Trans- to the confirmation of the Order may do so in writing port for confirmation an Order under section 14 of the before 16th May 1981, to the Minister of Transport at Highways Act 1980 and of all other enabling powers the office of the Regional Controller (Roads and Trans- which will authorise the Council: portation), North-West Region, Sunley Buildings, Piccadilly (a) To carry out the improvement of highways. Plaza, Manchester Ml 4BE, stating the grounds of (b) To stop-up highways. objection. (c) To construct a new highway which shall be a road. W. R. T. Woods, Chief Executive Officer and Secretary (d) To stop-up a private means of access to premises. (e) To provide a new means of access to premises. Council Offices, All on or in the vicinity of the route of the classified Whitehall, School Lane, road which the Council are proposing to construct between Hartford, Northwich. -

1/11/2006 Health in an Unequal World Michael Marmot This Is a Lightly
1/11/2006 Health in an Unequal World Michael Marmot This is a lightly edited version of the (October) 2006 Harveian Oration at the Royal College of Physicians. It will be published in Clinical Medicine and the Lancet. In poor countries, tragically, people die unnecessarily. In rich countries, too, the higher death rate of those in less fortunate social positions is unnecessary. Can there be a link between these two phenomena: inequalities in health among countries and inequalities within? Surely, it might be argued, the depredations of grinding poverty – lack of food, shelter, clean water, and basic medical care or public health – that ravage the lives of the poor in developing countries are different in kind from the way that social disadvantage leads to poor health in modern Britain, for example. The diseases of the slums of Nairobi are, to be sure, different in kind from the diseases that affect the disadvantaged in east London or Harlem, and have different proximate causes. There is, however, a link. The unnecessary disease and suffering of the disadvantaged, whether in poor countries or rich, is a result of the way we organise our affairs in society. I shall argue, in this oration, that failing to meet the fundamental human need of autonomy, empowerment, or human freedom is a potent cause of ill-health. In making this case, I shall bring together two rather disparate streams of work. The first is a report of my own research endeavour. I have sought explanations for the social gradient in health, as observed in the Whitehall studies, pointing to the fundamental importance of the circumstances in which people live and work. -
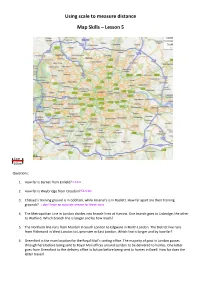
Using Scale to Measure Distance Map Skills – Lesson 5
Using scale to measure distance Map Skills – Lesson 5 1cm 10km Questions: 1. How far is Barnet from Enfield? 2. How far is Weybridge from Croydon? 3. Chelsea’s training ground is in Cobham, while Arsenal’s is in Radlett. How far apart are their training grounds? 4. The Metropolitan Line in London divides into branch lines at Harrow. One branch goes to Uxbridge, the other to Watford. Which branch line is longer and by how much? 5. The Northern line runs from Morden in South London to Edgware in North London. The District line runs from Richmond in West London to Upminster in East London. Which line is longer and by how far? 6. Greenford is the main location for the Royal Mail’s sorting office. The majority of post in London passes through here before being sent to Royal Mail offices around London to be delivered to homes. One letter goes from Greenford to the delivery office in Sutton before being sent to homes in Ewell. How far does the letter travel? The map below zooms in on the area of Westminster. 1cm 75m QUESTIONS: 1. The Houses of Parliament is shown by its proper name of the Palace of Westminster on this map. How far does the Prime Minister have to travel to get from 10 Downing Street to Parliament? 2. Horse Guards Parade will be the venue of the Beach Volleyball at this summer’s Olympic Games. How far is it from Charing Cross station? 3. How long is Westminster Bridge? 4. A walking tour of the government buildings starts at Big Ben, goes up Parliament St and Whitehall, along Northumberland Avenue, and back down the Victoria Embankment. -

Middle Saxon and Later Archaeological Remains in Whitehall
MIDDLE SAXON AND LATER ARCHAEOLOGICAL REMAINS IN WHITEHALL Paw Jorgensen With contributions by Jonathan Butler, Kevin Hayward, Chris Jarrett and Kevin Rielly SUMMARY Guards Road to the west, the Embankment to the east, Parliament Square to the south Archaeological investigations undertaken during the and Great Scotland Yard to the north (Figs streetscape improvements in Whitehall revealed the 2, 2a, 2b). Bordering upon the site are remains of several periods of activity. Middle Saxon governmental offices, mostly dating to the activity most likely associated with that previously late 19th and 20th centuries, many of which found at the Old Treasury Building in the 1960s was are Listed Buildings. In total 78 Listed revealed on Whitehall opposite the west end of Horse Buildings are located immediately adjacent Guards Avenue. Elsewhere masonry associated with to the site; of these, 14 are Grade I listed, York Place, the Archbishop of York’s official residence 17 Grade II* listed, and 47 Grade II listed; in London, and Whitehall Palace was found. Later these include Queen Mary’s Steps, the Ban- remains consisted of buildings which were constructed queting House, the Ministry of Defence in the 18th and 19th century following the destruction Main Building, and the Cabinet Office, Privy of Whitehall Palace in two fires at the end of the 17th Council and Treasury Building, all of which century. to varying degrees have incorporated part of the fabric of Whitehall Palace into the INTRODUCTION current buildings and structures. Furthermore, the entire site lies within the Pre-Construct Archaeology was commiss- Lundenwic and Thorney Island Area of Spec- ioned by Atkins Heritage acting on behalf ial Archaeological Priority and immediately of the City of Westminster to undertake a to the south is the World Heritage Site of watching-brief during streetscape improve- Westminster Palace, Westminster Abbey and ments along Whitehall and the adjoining St Margaret’s Church (WHS number 462). -

The Old War Office Building
MINISTRY OF DEFENCE The Old War Office Building A history The Old War Office Building …a building full of history Foreword by the Rt. Hon Geoff Hoon MP, Secretary of State for Defence The Old War Office Building has been a Whitehall landmark for nearly a century. No-one can fail to be impressed by its imposing Edwardian Baroque exterior and splendidly restored rooms and stairways. With the long-overdue modernisation of the MOD Main Building, Defence Ministers and other members of the Defence Council – the Department’s senior committee – have moved temporarily to the Old War Office. To mark the occasion I have asked for this short booklet, describing the history of the Old War Office Building, to be published. The booklet also includes a brief history of the site on which the building now stands, and of other historic MOD headquarters buildings in Central London. People know about the work that our Armed Forces do around the world as a force for good. Less well known is the work that we do to preserve our heritage and to look after the historic buildings that we occupy. I hope that this publication will help to raise awareness of that. The Old War Office Building has had a fascinating past, as you will see. People working within its walls played a key role in two World Wars and in the Cold War that followed. The building is full of history. Lawrence of Arabia once worked here. I am now occupying the office which Churchill, Lloyd-George and Profumo once had. -

The Great Plague 1665- 1666 How Did London Respond to It?
The National Archives Education Service The Great Plague 1665- 1666 How did London respond to it? London scenes of the Plague 1665-1666 – Museum of London The Great Plague 1665-1666 How did London respond? Introduction Lesson at a Glance The Plague This was the worst outbreak of plague in England since the black death Suitable For: KS3 of 1348. London lost roughly 15% of its population. While 68,596 deaths were recorded in the city, the true number was probably over Time Period: 100,000. Other parts of the country also suffered. Early Modern 1485-1750 The earliest cases of disease occurred in the spring of 1665 in a parish outside the city walls called St Giles-in-the-Fields. The death rate Curriculum Link: began to rise during the hot summer months and peaked in September The development of when 7,165 Londoners died in one week. Church, state and society Rats carried the fleas that caused the plague. They were attracted by in Britain 1509-1745 city streets filled with rubbish and waste, especially in the poorest areas. Society, economy and culture across the period Those who could, including most doctors, lawyers and merchants, fled Learning Objective: the city. Charles II and his courtiers left in July for Hampton Court and then Oxford. Parliament was postponed and had to sit in October at Oxford, the increase of the plague being so dreadful. Court cases were To closely examine a also moved from Westminster to Oxford. document in order to discover information. The Lord Mayor and aldermen (town councillors) remained to enforce the King’s orders to try and stop the spread of the disease. -
Whitehall Mini Guide
TO VIEW CONSERVATION AREA MAP CLICK HERE FOR LINK TO WESTMINSTER MAPPING SYSTEM DEPARTMENT OF PLANNING AND CITY DEVELOPMENT DEVELOPMENT PLANNING SERVICES MAY 2004 Designation: First designated as a Conservation Area in 1969 as part of pedestrian route to St James’s Park and a large open arena where the larger Government Precinct Conservation Area. Redesignated in 1987 annually the Trooping of the Colour takes place. The Cenotaph, positioned as the Whitehall Conservation Area. in the middle of Whitchall is an international memorial to those who died for their country in armed conflicts, and the annual Remembrance Service is Historical Background: Throughout the medieval period, the held in front of it. The Conservation Area includes the tree lined public Palace of Whitehall grew as a complex of buildings housing the Royal open spaces of Victoria Embankment Gardens, containing a number of Family. It was substantially extended by Henry VIII who also acquired St. statues of important statesmen, as well as the Embankment itself which James’s Park and other land for hunting, thus assuring the continuing affords panoramic views across the Thames. There is more open space in close relationship of open space to Royal and government buildings. The Raleigh Green, on the east side of Whitehall. eastern portion of the Palace was a rambling mixture of buildings and, as the first instalment of a grandiose rebuilding scheme by Inigo Jones, the The area contains many buildings of national importance, in both Banqueting House was begun in 1617. In 1698 a fire destroyed almost the architectural and historic terms. Some of the most important buildings in whole of the Palace; the plans to rebuild the area as Royal Residence and terms of the townscape of the Conservation Area are the Banqueting Courts were abandoned, and Jones’s scheme was never implemented. -

A Persuasive Interior: Reconstructing the Whitehall Palace Privy Chamber
A Persuasive Interior: Reconstructing the Whitehall Palace Privy Chamber A Persuasive Interior: Reconstructing the Whitehall Palace Privy Chamber Miranda L. Elston One of the most distinguishable features of Henry VIII’s reign was the meticulous use of architecture and the interior to instatiate his supremacy as King of England. This research uses the king’s Privy Chamber, a private apartment in the royal apartments, at Whitehall Palace as the paradigmatic example to critically assess the Henrician interior in an interdisciplinary study. Through an examination of the primary accounts and records, inventories, archaeological studies and visual evidence from extant interiors and visual representations, this essay digitally reconstructs the Whitehall Privy Chamber to analyze its function. The creation of digital reconstructions of the Whitehall Privy Chamber reveals tangible evidence allowing us to understand the Henrician interior as a holistic space that simultaneously aligned Henry VIII with his historic ancestry and imagery of the virtuous Renaissance Prince. Institute for European and Mediterranean Archaeology 89 Miranda L. Elston Introduction for important audiences and ceremonies. In March 1542, the ennoblement of Sir John Dudley as Viscount Lisle took place in the Once situated along the banks of the Privy Chamber, and in February 1544 the Thames River, just north of Westminster, 4 Whitehall Palace epitomized the Duke of Najera was received there as well. architectural magnificence of the court Furthermore, the shift in function of the Privy of Henry VIII (1491-1547, ruling from Chamber can be seen in that a new extended 1509 until his death). Unfortunately, the privy lodging that was subsequently built at splendor of Whitehall was lost when Whitehall.5 The Privy Chamber in Whitehall a fire destroyed most of the palace Palace was therefore a space designed to in 1698. -

Obesity and Overweight in Relation to Mortality in Men with and Without Type 2 Diabetes/Impaired Glucose Tolerance the Original Whitehall Study
Cardiovascular and Metabolic Risk BRIEF REPORT Obesity and Overweight in Relation to Mortality in Men With and Without Type 2 Diabetes/Impaired Glucose Tolerance The original Whitehall Study 1 2 G. DAVID BATTY, PHD MICHAEL G. MARMOT, FRCP IGT (n ϭ 1,030) and in those with type 2 2 2 MIKA KIVIMAKI, PHD MARTIN J. SHIPLEY, MSC diabetes (n ϭ 195) was very similar. That 3 GEORGE DAVEY SMITH, MD is, there was no suggestion that the all- cause weight-mortality relation differed between the IGT (hazard ratio [HR] per n studies of apparently healthy individ- ernment employees aged 40–69 years increase in weight category 1.12 [95% CI uals, overweight and obesity, typically when examined between 1967 and 1970, 1.00–1.25]) and diabetes group (1.19 I assessed using BMI, have been consis- representing a 74% response (22). Height [0.94–1.49], P ϭ 0.64 for difference in tently associated with an increased risk of and weight were measured using stan- gradient between groups). Similar results all-cause mortality, cardiovascular dis- dard protocols, and BMI was computed were apparent when CVD was the out- ease (CVD), and select cancers (1–4). (weight [kg]/height2 [m2]) and catego- come of interest (P ϭ 0.98). Therefore, we However, extrapolating these results to rized according to current guidelines combined the IGT and type 2 diabetes individuals with type 2 diabetes is com- (23): normal weight (18.5 to Ͻ25.0), groups, an approach we have taken else- plex and perhaps inappropriate. Studies over weight (25.0–29.99), and obesity where (26).