UI-FHS Mid-Program Review Full Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

An Analysis of the Afar-Somali Conflict in Ethiopia and Djibouti
Regional Dynamics of Inter-ethnic Conflicts in the Horn of Africa: An Analysis of the Afar-Somali Conflict in Ethiopia and Djibouti DISSERTATION ZUR ERLANGUNG DER GRADES DES DOKTORS DER PHILOSOPHIE DER UNIVERSTÄT HAMBURG VORGELEGT VON YASIN MOHAMMED YASIN from Assab, Ethiopia HAMBURG 2010 ii Regional Dynamics of Inter-ethnic Conflicts in the Horn of Africa: An Analysis of the Afar-Somali Conflict in Ethiopia and Djibouti by Yasin Mohammed Yasin Submitted in partial fulfilment of the requirements for the degree PHILOSOPHIAE DOCTOR (POLITICAL SCIENCE) in the FACULITY OF BUSINESS, ECONOMICS AND SOCIAL SCIENCES at the UNIVERSITY OF HAMBURG Supervisors Prof. Dr. Cord Jakobeit Prof. Dr. Rainer Tetzlaff HAMBURG 15 December 2010 iii Acknowledgments First and foremost, I would like to thank my doctoral fathers Prof. Dr. Cord Jakobeit and Prof. Dr. Rainer Tetzlaff for their critical comments and kindly encouragement that made it possible for me to complete this PhD project. Particularly, Prof. Jakobeit’s invaluable assistance whenever I needed and his academic follow-up enabled me to carry out the work successfully. I therefore ask Prof. Dr. Cord Jakobeit to accept my sincere thanks. I am also grateful to Prof. Dr. Klaus Mummenhoff and the association, Verein zur Förderung äthiopischer Schüler und Studenten e. V., Osnabruck , for the enthusiastic morale and financial support offered to me in my stay in Hamburg as well as during routine travels between Addis and Hamburg. I also owe much to Dr. Wolbert Smidt for his friendly and academic guidance throughout the research and writing of this dissertation. Special thanks are reserved to the Department of Social Sciences at the University of Hamburg and the German Institute for Global and Area Studies (GIGA) that provided me comfortable environment during my research work in Hamburg. -

Districts of Ethiopia
Region District or Woredas Zone Remarks Afar Region Argobba Special Woreda -- Independent district/woredas Afar Region Afambo Zone 1 (Awsi Rasu) Afar Region Asayita Zone 1 (Awsi Rasu) Afar Region Chifra Zone 1 (Awsi Rasu) Afar Region Dubti Zone 1 (Awsi Rasu) Afar Region Elidar Zone 1 (Awsi Rasu) Afar Region Kori Zone 1 (Awsi Rasu) Afar Region Mille Zone 1 (Awsi Rasu) Afar Region Abala Zone 2 (Kilbet Rasu) Afar Region Afdera Zone 2 (Kilbet Rasu) Afar Region Berhale Zone 2 (Kilbet Rasu) Afar Region Dallol Zone 2 (Kilbet Rasu) Afar Region Erebti Zone 2 (Kilbet Rasu) Afar Region Koneba Zone 2 (Kilbet Rasu) Afar Region Megale Zone 2 (Kilbet Rasu) Afar Region Amibara Zone 3 (Gabi Rasu) Afar Region Awash Fentale Zone 3 (Gabi Rasu) Afar Region Bure Mudaytu Zone 3 (Gabi Rasu) Afar Region Dulecha Zone 3 (Gabi Rasu) Afar Region Gewane Zone 3 (Gabi Rasu) Afar Region Aura Zone 4 (Fantena Rasu) Afar Region Ewa Zone 4 (Fantena Rasu) Afar Region Gulina Zone 4 (Fantena Rasu) Afar Region Teru Zone 4 (Fantena Rasu) Afar Region Yalo Zone 4 (Fantena Rasu) Afar Region Dalifage (formerly known as Artuma) Zone 5 (Hari Rasu) Afar Region Dewe Zone 5 (Hari Rasu) Afar Region Hadele Ele (formerly known as Fursi) Zone 5 (Hari Rasu) Afar Region Simurobi Gele'alo Zone 5 (Hari Rasu) Afar Region Telalak Zone 5 (Hari Rasu) Amhara Region Achefer -- Defunct district/woredas Amhara Region Angolalla Terana Asagirt -- Defunct district/woredas Amhara Region Artuma Fursina Jile -- Defunct district/woredas Amhara Region Banja -- Defunct district/woredas Amhara Region Belessa -- -
20210714 Access Snapshot- Tigray Region June 2021 V2
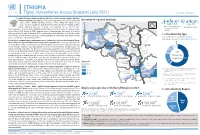
ETHIOPIA Tigray: Humanitarian Access Snapshot (July 2021) As of 31 July 2021 The conflict in Tigray continues despite the unilateral ceasefire announced by the Ethiopian Federal Government on 28 June, which resulted in the withdrawal of the Ethiopian National Overview of reported incidents July Since Nov July Since Nov Defense Forces (ENDF) and Eritrea’s Defense Forces (ErDF) from Tigray. In July, Tigray forces (TF) engaged in a military offensive in boundary areas of Amhara and Afar ERITREA 13 153 2 14 regions, displacing thousands of people and impacting access into the area. #Incidents impacting Aid workers killed Federal authorities announced the mobilization of armed forces from other regions. The Amhara region the security of aid Tahtay North workers Special Forces (ASF), backed by ENDF, maintain control of Western zone, with reports of a military Adiyabo Setit Humera Western build-up on both sides of the Tekezi river. ErDF are reportedly positioned in border areas of Eritrea and in SUDAN Kafta Humera Indasilassie % of incidents by type some kebeles in North-Western and Eastern zones. Thousands of people have been displaced from town Central Eastern these areas into Shire city, North-Western zone. In line with the Access Monitoring and Western Korarit https://bit.ly/3vcab7e May Reporting Framework: Electricity, telecommunications, and banking services continue to be disconnected throughout Tigray, Gaba Wukro Welkait TIGRAY 2% while commercial cargo and flights into the region remain suspended. This is having a major impact on Tselemti Abi Adi town May Tsebri relief operations. Partners are having to scale down operations and reduce movements due to the lack Dansha town town Mekelle AFAR 4% of fuel. -
Report on Evaluation of W SH
Report on Evaluation of WASH - Joint Action Plan (JAP) implementation in eight water insecure Woredas in Afar Regional state Submitted to UNICEF – Ethiopia WASH Section/Afar Field office Prepared by Tesfa Aklilu WASH - Consultant (CIPM, BSc, MPH, MSc (pending, AAU) November 13, 2015 Afar – Semera - Ethiopia | P a g e Table of contents Table of figures .............................................................................................................................................. i Tables ............................................................................................................................................................. i Acronyms ...................................................................................................................................................... ii WASHCOs: Water, Sanitation and Hygiene Committees ........................................................... ii Acknowledgement ........................................................................................................................................ ii Executive Summary ................................................................................................................................ iii 1. Introduction ........................................................................................................................................... 1 2. Objectives of Evaluation ............................................................................................................... 2 2.1. General -

Hum Ethio Manitar Opia Rian Re Espons E Fund D
Hum anitarian Response Fund Ethiopia OCHA, 2011 OCHA, 2011 Annual Report 2011 Office for the Coordination of Humanitarian Affairs Humanitarian Response Fund – Ethiopia Annual Report 2011 Table of Contents Note from the Humanitarian Coordinator ................................................................................................ 2 Acknowledgements ................................................................................................................................. 3 1. Executive Summary ............................................................................................................................ 4 1.1 2011 Humanitarian Context ........................................................................................................... 4 1.2 Map - 2011 HRF Supported Projects ............................................................................................. 6 2. Information on Contributors ................................................................................................................ 7 2.1 Donor Contributions to HRF .......................................................................................................... 7 3. Fund Overview .................................................................................................................................... 8 3.1 Summary of HRF Allocations in 2011 ............................................................................................ 8 3.1.1 HRF Allocation by Sector ....................................................................................................... -
Examining Alternative Livelihoods for Improved Resilience and Transformation in Afar
EXAMINING ALTERNATIVE LIVELIHOODS FOR IMPROVED RESILIENCE AND TRANSFORMATION IN AFAR May 2019 Report photos: Dr. Daniel Temesgen EXAMINING ALTERNATIVE LIVELIHOODS FOR IMPROVED RESILIENCE AND TRANSFORMATION IN AFAR May 2019 This document has been produced with the financial assistance of the European Union. The views expressed herein can in no way be taken to reflect the official opinion of the European Union. Report authors: Daniel Temesga, Amdissa Teshome, Berhanu Admassu Suggested citation: FAO and Tufts University. (2019). Examining Alternative Livelihoods for Improved Resilience and Transformation in Afar. FAO: Addis Ababa, Ethiopia. Implemented by: Feinstein International Center Friedman School of Nutrition Science and Policy Tufts University Africa Regional Office www.fic.tufts.edu © FAO TABLE OF CONTENTS EXECUTIVE SUMMARY ............................................................................................................................... 6 I. BACKGROUND............................................................................................................................................ 8 The Afar Region: context and livelihoods ................................................................................................... 8 The purpose of the study ............................................................................................................................ 8 The study’s approaches and methods ......................................................................................................... -

FEDERAL DEMOCRATIC REPUBLIC of ETHIOPIA El 320 Public Disclosure Authorized
FEDERAL DEMOCRATIC REPUBLIC OF ETHIOPIA El 320 Public Disclosure Authorized ETHIOPIAN ELECTRIC AND POWER CORPORATION (EEPCO) UNIVERSAL ELECTRIFICATION ACCESS PROGRAM Public Disclosure Authorized (UEAP) ENVIRONMENTAL AND SOCIAL MANAGEMENT FRAMEWORK (ESMF) Public Disclosure Authorized February 2006 Beza Consulting Engineers, PLC BCEn 1 I b@2 xYgi m/NA!iC 'Ayt'AyGY4ThbR Public Disclosure Authorized BCE' ~ dll Consultant in Road, Building, Water & Energy Sectors Tel. 6 632861 /6 632862 Fax: 6 627809 P. O. Box: 41292 E-mail: [email protected] Addis Ababa, Ethiopia EEPCO - Environmental and Social Management Framework (ESMF) Table of Contents List of Acronyms ....................................... 4 EXECUTIVE SUMMARY ....................................... 6 1. Introduction ....................................... 10 1.] Background and General....................................... 10 1.2 Objective of the ESMF........................................ 11 1.3 Scope of Programand the Assessment ....................................... 12 1. 4 Environmental and Social Planning....................................... 12 1.5 Study Methodology ....................................... 14 2. Legislative and Regulatory Framework ....................................... 15 2. Legislative and Regulatory Framework ....................................... 15 2.1 The Federal Democratic Republic of Ethiopia....................................... 15 2.1.1 Legal Framework ....................................... 15 2.1.2 Institutional Framework ....................................... -

ETHIOPIA - National Hot Spot Map 31 May 2010
ETHIOPIA - National Hot Spot Map 31 May 2010 R Legend Eritrea E Tigray R egion !ª D 450 ho uses burned do wn d ue to th e re ce nt International Boundary !ª !ª Ahferom Sudan Tahtay Erob fire incid ent in Keft a hum era woreda. I nhabitan ts Laelay Ahferom !ª Regional Boundary > Mereb Leke " !ª S are repo rted to be lef t out o f sh elter; UNI CEF !ª Adiyabo Adiyabo Gulomekeda W W W 7 Dalul E !Ò Laelay togethe r w ith the regiona l g ove rnm ent is Zonal Boundary North Western A Kafta Humera Maychew Eastern !ª sup portin g the victim s with provision o f wate r Measle Cas es Woreda Boundary Central and oth er imm ediate n eeds Measles co ntinues to b e re ported > Western Berahle with new four cases in Arada Zone 2 Lakes WBN BN Tsel emt !A !ª A! Sub-city,Ad dis Ababa ; and one Addi Arekay> W b Afa r Region N b Afdera Military Operation BeyedaB Ab Ala ! case in Ahfe rom woreda, Tig ray > > bb The re a re d isplaced pe ople from fo ur A Debark > > b o N W b B N Abergele Erebtoi B N W Southern keb eles of Mille and also five kebeles B N Janam ora Moegale Bidu Dabat Wag HiomraW B of Da llol woreda s (400 0 persons) a ff ected Hot Spot Areas AWD C ases N N N > N > B B W Sahl a B W > B N W Raya A zebo due to flo oding from Awash rive r an d ru n Since t he beg in nin g of th e year, Wegera B N No Data/No Humanitarian Concern > Ziquala Sekota B a total of 967 cases of AWD w ith East bb BN > Teru > off fro m Tigray highlands, respective ly. -
Early Warning and Response Analysis August 2014
Early Warning and Response Directorate DRMFSS, MoA Early Warning and Response Analysis August 2014 This bulletin is prepared by the Early Warning and Response Directorate to coordinate and disseminate early warning and food security information. For any comments, questions or suggestions and/or to receive the bulletin on your email please write to [email protected] If you are planning to contribute to the response effort, please inform DRMFSS by writing to [email protected] Released on August, 2014 2 Early Warning and Response Analysis August, 2014 Contents Acronyms .......................................................................................................................................................... 3 Early Warning and ResponseSummary………..………………………………………………………………4 Weather Conditions ........................................................................................................................................... 5 Agriculture……………………….…………………………………………………………………………….6 Nutrition ............................................................................................................................................................ 7 Appendix ......................................................................................................................................................... 10 Early Warning and Response Directorate, MoA 3 Early Warning and Response Analysis August, 2014 ACRONYMS: CPI: Consumer Price Index CSA: Central Statistical Agency DRMFSS: Disaster Risk Management and Food Security Sector: -

Humanitarian Bulletin 28 January 2013.Pdf (English)
Relief Food Update As of 23 January, distribution of seventh round relief food, targeting 2.8 million people countrywide, reached 84 per cent. Dispatch of the “bridging” round, targeting 1.5 million people in Afar, Amhara, Oromia, Somali and Harari Regions, reached 33 per cent as of the same date, including 47 per cent to areas covered by the Disaster Risk Management and Food Security Sector (DRMFSS), 28 per cent to areas covered by the NGO consortium joint emergency operation (JEOP) and 17 per cent to WFP-covered areas. Beneficiaries in areas covered by WFP (Somali Region) and JEOP will receive a full basket and full ration, while those in areas covered by the DRMFSS will receive a half-ration of vegetable oil and full rations of all other commodities. For more information, contract [email protected] WASH Update A multi-agency rapid assessment in Barey woreda (Afder zone, Somali Region), conducted from 13 to 17 January, has verified the reported drought conditions that have prompted serious water shortages and high levels of malnutrition in parts of the woreda. According to the assessment team, an immediate start to water trucking is required in two of the five kebeles identified by the local authorities as ‘priority 1 water hot-spots’, including Dudun and Harhodey. In total, 15 kebeles were identified as water hot-spots: five “priority 1” kebeles requiring water trucking in February; six “priority 2” kebeles likely to need water trucking from early March; and four ‘priority 3” kebeles where water supplies are expected to last through the end of March. -

Periodic Monitoring Report Working 2016 Humanitarian Requirements Document – Ethiopia Group
DRMTechnical Periodic Monitoring Report Working 2016 Humanitarian Requirements Document – Ethiopia Group Covering 1 Jan to 31 Dec 2016 Prepared by Clusters and NDRMC Introduction The El Niño global climactic event significantly affected the 2015 meher/summer rains on the heels of failed belg/ spring rains in 2015, driving food insecurity, malnutrition and serious water shortages in many parts of the country. The Government and humanitarian partners issued a joint 2016 Humanitarian Requirements Document (HRD) in December 2015 requesting US$1.4 billion to assist 10.2 million people with food, health and nutrition, water, agriculture, shelter and non-food items, protection and emergency education responses. Following the delay and erratic performance of the belg/spring rains in 2016, a Prioritization Statement was issued in May 2016 with updated humanitarian requirements in nutrition (MAM), agriculture, shelter and non-food items and education.The Mid-Year Review of the HRD identified 9.7 million beneficiaries and updated the funding requirements to $1.2 billion. The 2016 HRD is 69 per cent funded, with contributions of $1.08 billion from international donors and the Government of Ethiopia (including carry-over resources from 2015). Under the leadership of the Government of Ethiopia delivery of life-saving and life- sustaining humanitarian assistance continues across the sectors. However, effective humanitarian response was challenged by shortage of resources, limited logistical capacities and associated delays, and weak real-time information management. This Periodic Monitoring Report (PMR) provides a summary of the cluster financial inputs against outputs and achievements against cluster objectives using secured funding since the launch of the 2016 HRD. -

Annual Results Report to USAID
Productive Safety Net Programme Pilot Area Programme (PSNP-PAP) Afar National Regional State, Ethiopia Chifra, Gulina and Teru woredas Award No. FFP-A-00-08-00034-00 Annual Results Report to USAID Resubmission, 21 November 2008 Submitted by: The PSNP-PAP Programme, SCUK, Ethiopia 1 Acronyms ARDPFSB Afar Regional Disaster Prevention and Food Security Bureau KA Kebele Administration KFSTF Kebele Food Security Task Force DA Development Agent FSTF Food Security Task Force HH House Hold LBPW Labour Based Public Works DS Direct Support M&E Monitoring & Evaluation PSNP PAP Productive Safety Net Programme Pastoral Areas Pilot SWC Soil and Water Conservation USAID United States Agency for International Development WFSTF Woreda Food Security Task Force WPARDO Woreda Pastoral Agriculture and Rural Development office M3 Cubic Meter RDIR Reducing Dependency and Increasing Resiliency SSI SSI – Small Scale Irrigation SWC Soil & Water Conservation MOU Memorandum of Understanding ToT Training of Trainers FSTF Food Security Task Force Ha Hectare HH Household WFSTF Woreda Food Security Task Force 2 Table of content page 1. Background/context 4 2. Executive Summary 5 2.1 Key progress made during the period 5 3. Programme start up activities 6 4. Progress to date of programme activities 7 4.1. Government and Community Capacity Building 7 4.2. Targeting approaches 9 4.3. Public works 10 4.4. Methods of food distribution 11 5 PSNP-PAP success stories 12 6. Programme closeout Status 13 7. Lessons learnt 14 8. Important issues during programme implementation 14 Appendices Appendix 7: Standardized annual performance questionnaire (SAPQ) Appendix 8: Summarized commodity and beneficiary status report Appendix 9: Financial Report for Afar PSNP-PAP 3 1.