New Patient Questionnaire – 3 Page Document Read and Completed
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
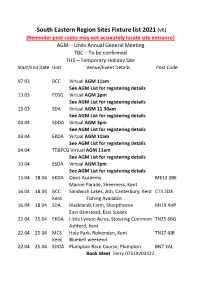
South Eastern Region Sites Fixture List 2021 (V6)
-South Eastern Region Sites Fixture list 2021 (v6) (Reminder post codes may not accurately locate site entrance} AGM – Units Annual General Meeting TBC – To be confirmed THS – Temporary Holiday Site Start/End Date Unit Venue/Event Details Post Code 07.03 BCC Virtual AGM 11am See AGM List for registering details 13.03 FDSG Virtual AGM 3pm See AGM List for registering details 13.03 SDA Virtual AGM 11.30am See AGM List for registering details 03.04 SDDA Virtual AGM 3pm See AGM List for registering details 03.04 EKDA Virtual AGM 11am See AGM List for registering details 04.04 TT&FCG Virtual AGM 11am See AGM List for registering details 10.04 ESDA Virtual AGM 2pm See AGM List for registering details 15.04 18.04 EKDA Oasis Academy ME12 2BE Marine Parade, Sheerness, Kent 16.04 18.04 BCC Sandwich Lakes, Ash, Canterbury, Kent CT3 2DA Kent Fishing Available 16.04 18.04 SDA Blacklands Farm, Sharpthorne RH19 4HP East Grinstead, East Sussex 22.04 25.04 EKDA Little Lynton Acres, Stowting Commom TN25 6BG Ashford, Kent 22.04 25.04 MCS Hole Park, Rolvenden, Kent TN17 4JB Kent Bluebell weekend 22.04 25.04 SDDA Plumpton Race Course, Plumpton BN7 3AL Book Meet Terry 07519203422 23.04 25.04 BCC Kent Fir Tree Farm, Rhodes Minnis, Kent CT4 6XR 29.04 04.05 MCS Orchard Farm, Chidham, Bosham PO18 8PP Southern West Sussex. PH/Bus close by BHM 29.04 03.05 EKDA Jemmet Farm, Mersham, Kent BHM TN25 7HB 29.04 04.05 MCS Kent Quex Park, Birchington, Kent BHM CT7 0BH 29.04 04.05 SDA Pierrepont Farm, Tilford, Surrey BHM GU10 3BS 29.04 03.05 ESDA Laughing Fish, Isfield, -

Agenda 4Th March 2019 Final Page to ALL COUNCILLORS 27Th
TO ALL COUNCILLORS 27th February 2019 THERE IS TO BE A MONTHLY MEETING OF THE ABOVE PARISH COUNCIL ON MONDAY 4th MARCH 2019. IT WILL BE HELD IN THE VILLAGE HALL STARTING 7.30pm. YOU ARE HEREBY SUMMOND TO ATTEND. THE AGENDA IS AS FOLLOWS: 41/19 To record those present and list any apologises. 42/19 To declare any Disclosable Pecuniary Interests (DPI), Other significant Interests (OSI’s) or a Voluntary interest relating to items on the agenda. A member who declares a DPI in relation to any item on the agenda will need to leave the meeting for the whole of that item and will not be able to speak or take part unless a relevant Dispensation has been granted. A member who declares an OSI will be able to speak on the item but will be required to leave the meeting for the vote. Councillors may also declare a voluntary interest if they are unsure of their position. Inclusion and voting will be decided at the time of the declaration, unless this has been discussed with the clerk prior to the meeting. 43/19 To note and agree minutes of a) The February 2019 PC meeting. b) The Extraordinary meeting February 2019. 44/19 To consider any matters arising from the Minutes not on the agenda elsewhere. 45/19 Core Strategy Review Submission Draft 1) To discuss and agree action. 46/19 Folkestone and Hythe Heritage Strategy Public Consultation 1) To discuss and agree action. 47/19 Public Contribution (For members of the public to ask questions – This item will last no more than 15 minutes) 1 . -
Some Problems of the North Downs Trackway in Kent
http://kentarchaeology.org.uk/research/archaeologia-cantiana/ Kent Archaeological Society is a registered charity number 223382 © 2017 Kent Archaeological Society SOME PROBLEMS OF THE NORTH DOWNS TRACKWAY IN KENT By REV. H. W. R. Liman, S.J., M.A.(0xon.) THE importance of this pre-historic route from the Continent to the ancient habitat of man in Wiltshire has long been recognized. In the Surrey Archceological Collections of 1964 will be found an attempted re-appraisal of its route through the county of Surrey. Although the problems connected with its passage through Kent are fewer owing to its being better preserved, there are some points which I think still deserve attention—the three river crossings of the Darenth, the Medway and the Stour; the crossing of the Elham valley; and the passage to Canterbury of the branch route from Eastwell Park, known as the Pilgrims' Way. It may be worth while, before dealing with the actual crossings, to note a few general characteristics. Mr. I. D. Margary—our most eminent authority on ancient roads in Britain—has pointed out the dual nature of this trackway. It com- prises a Ridgeway and a Terraceway. The first runs along the crest of the escarpment. The second runs parallel to it, usually at the point below the escarpment where the slope flattens out into cultivation. In Kent for the most part the Terraceway has survived more effectually than the Ridgeway. It is for much of its length used as a modern road, marked by the familiar sign 'Pilgrims' Way'. Except at its eastern terminus the Ridgeway has not been so lucky, although it can be traced fairly accurately by those who take the trouble to do so. -
THE LYMINGE NEWSLETTER for the Communities of LYMINGE, ETCHINGHILL, RHODES MINNIS and POSTLING
THE LYMINGE NEWSLETTER For the communities of LYMINGE, ETCHINGHILL, RHODES MINNIS and POSTLING http://www.lyminge.org.uk/ Produced by THE LYMINGE ASSOCIATION February 2013 LYMINGE ASSOCIATION NEWS Garage Safari ~ is being held on Saturday April 20th. Save all those things that you sorted out at the start of the year - Save all those things that you find in your Spring Sort Out and even, dare we say - unwanted Christmas presents ! Turn them all into cash for your Summer Holiday. Don’t forget that you can have a table at the Village Hall for the same price - and there will be refreshments available there, at very reasonable prices, during the day !! Garden Safari and Lyminge Festival is due to take place over the week-end of 15th and 16th June. Also planned is a Flower Festival at the Parish Church and an Art Exhibition at the Tayne Centre. Did you know - that as a resident in Lyminge, Etchinghill, Rhodes Minnis and Postling you are automatically a member of the Lyminge Association ? The Association is very keen to welcome anyone who would like to help with one of the many events that it organises. Would you like to help maintain the TROUGHS that the Lyminge Association has positioned at the Woodland Road/Brady Road crossroads and Yew Tree Cross or help on our stall on Lyminge Day on 11th May or perhaps the Coronation Variety Show being planned for September might be just what you would like to do. We need people to perform and to assist with the production. Do we have a local Magician ? Are you in a local pop group or do you have Performing Ferrets ! Please call Adrian on 862699. -
The Lyminge Newsletter
THE LYMINGE NEWSLETTER For the communities of LYMINGE, ETCHINGHILL, RHODES MINNIS and POSTLING May 2008 Produced by The Lyminge Association DON'T FORGET...The Village Clean-Up Day on Sunday 18th May starting at 9.00am at The Village Hall All help is very welcome - help keep our Village neat and tidy. Lyminge Heritage Questions and Answers This month we have a summary of all the questions posed so far and a new one. If you have any answers or other local heritage questions let me know through the editor. These questions are now posted on the Lyminge Online website at www.lyminge.org.uk/forums (click on the General Chat link). Rather than contacting the editor, you can post your responses there if you wish. Q1 Why is the crossroads between Lyminge and Etchinghill called New Barn? Q2 Why does the Nailbourne flow continually in Lyminge yet at Elham, it is dry during the summer? Q3 How did Lyminge Football Club start and what is its history? Q4 Did the dilapidated gates at Yew Tree Cross have a use and is there another set? Q5 Did Lyminge ever have a village band? Q6 Why is Lyndon Hall situated so close to Canterbury Road? Q7 Have buzzards ever been seen in the parish? Q8 Who was the most notable local inhabitant? Q9 What is the history of the local cricket clubs? A4 Writing about the Lyminge Online website reminds me about the gates at Yew Tree Cross. Posted in one of the forums is an explanation about the gates. Apparently, they are not in their original position and have been moved. -

South Eastern Region Sites Fixture List 2021 (V2)
-South Eastern Region Sites Fixture list 2021 (v2) (Reminder post codes may not accurately locate site entrance} AGM – Units Annual General Meeting TBC – To be confirmed THS – Temporary Holiday Site Start/End Date Unit Venue/Event Details Post Code 06-02 FSDG St Nicholas Youth Centre RH9 8DT Godstone Surrey Dance/Am supper 2pm 29.01 31.01 EKDA Palm Bay Primary School, Cliftonville, Kent CT9 3PP Scottish Rally 18.02 21.02 EKDA Reculver School, Hillborough, Herne Bay CT6 6TA Kent 26.02 28.02 MCS Cranleigh First/Middle School, Surrey GU6 7AN S/SL Booked Meet- contact committee Spring Nosh OPEN 5pm 04.03 07.03 EKDA Canterbury CC Site Working Party CT4 4AB Hard standing /EHU Booked Meet 05.03 07.03 MCS Greatstone Primary School, Kent TN28 8SY Kent Hard standing-Hall Open 5pm Booked Meet 07951063401 07.03 BCC Lower bell PH, Old Chatham Road, Aylesford ME2 7EF Kent Kent AGM 11am 12.03 14.03 MCS Tillingbourne Schl, Tillingbourne, Guildford GU4 8NB S/SL Hall/Social 13.03 FSDG St Nicholas Youth Centre, Godstone, Surrey RH9 8DT Dance/Am Super AGM 3pm 13.03 SDA Weald School, Beare Green, Surrey RH5 4QW AGM 11.30am 18.03 21.03 EKDA Canterbury CC Site CT4 4AB Conservation Rally /Book Meet 18.03 23.03 TT&FCG White House Farm, Budletts, Uckfield TN22 2EA East Sussex 26.03 28.03 SDA Graffham CC Site Pre- season tidy up GU28 0QF 26.03 30.03 SDDA White House Farm, Budletts, TN22 2EA Uckfield, East Sussex. Booked Meet Terry 07519203422 01.04 06.04 SDDA Willingdon School, Eastbourne, BHM BN20 9QX East Sussex Booked Meet Terry 07519203422 Sat. -

(Public Pack)Agenda Document for Folkestone and Hythe Joint
Public Document Pack Agenda Meeting: Folkestone and Hythe Joint Transportation Board Date: 22 February 2021 Time: 6.00 pm Place: Remote Meeting via Zoom To: The members of the Folkestone & Hythe Joint Transportation Board The Board will consider the matters listed below at the date and time shown above. The meeting is open to the press and public and streamed live at bit.ly/YouTubeMeetings. Members of the Board who wish to have information on any matter arising on the Agenda which is not fully covered in these papers are requested to give notice prior to the meeting to the Chairman or appropriate officer. 1. Apologies for absence 2. Declarations of interest (Pages 3 - 4) Members of the Board should declare any discloseable pecuniary interest or any other significant interests in any item/s on this agenda. 3. Minutes (Pages 5 - 8) To consider and approve the minutes of the meeting held on 23 November 2020. 4. Proposed Parking Restrictions 2021 (Pages 9 - 12) A report by the FHDC Highway Engineer to the Joint Transportation Board. 5. Highway Works Programme 2020/21 (Pages 13 - 26) Report JTB/20/05 updates members on the identified schemes approved for construction. Queries about the agenda? Need a different format? Contact Kate Clark – Tel: 01303 853267 Email: [email protected] or download from our website www.folkestone-hythe.gov.uk Date of Publication: Thursday, 11 FebruaryPage 20211 This page is intentionally left blank Agenda Item 2 Declarations of Interest Disclosable Pecuniary Interest (DPI) Where a Member has a new or registered DPI in a matter under consideration they must disclose that they have an interest and, unless the Monitoring Officer has agreed in advance that the DPI is a 'Sensitive Interest', explain the nature of that interest at the meeting. -

Sandling Station (June 2019) I Onward Travel Information Local Area Map
Sandling Station (June 2019) i Onward Travel Information Local area map Contains Ordnance Survey data © Crown copyright and database right 2018 & also map data © OpenStreetMap contributors, CC BY-SA Buses Main destinations by bus (Data correct at June 2019) DESTINATION BUS ROUTES BUS STOP Ashford ^ 10, 10A A Bossingham 18 A Brabourne Lees 10, 10A A Canterbury 18 A Cheriton 10 A Folkestone ^ 10, 10A A Golden Valley (Shopping Centre) 10 A Hythe (Red Lion Square) 10, 10A, 18 A Hythe (RH&D Station) 10, 10A, 18 A Lower Hardres 18 A Lyminge 18 A Lympne 10, 10A A Nackington 18 A Naildown Estate (Seabrook) 10 A Newingreen 10, 10A A Port Lympne Wild Animal Park 10 A Rhodes Minnis 18 A Saltwood 10, 10A, 18 A 10A (or change buses Sandgate at Hythe Red Lion A Square) Seabrook 10, 10A A Sellindge (Ashford Road) 10, 10A A Sellindge (Greenfields) 10 A Shorncliffe 10 A Stelling Minnis 18 A Upper Hardres 18 A Wheelbarrow Town 18 A Willesborough/William Harvey Hospital 10, 10A A Bus route 10 operates a frequent service daily. Bus routes 10A and 18 operate a limited service on Mondays to Saturdays only. Notes ^ Direct trains operate to this destination from this Station. Rail replacement buses depart from the station forecourt. Change at Hythe for the Romney, Hythe & Dymchurch Railway (phone 01797 362 353 for more information). Sandling Station has no taxi rank or cab office. Advance booking is Folkestone Taxi Co Premier Taxis JJ Taxis essential, please consider using the following local operators: (Inclusion of Taxis this number doesn’t represent any endorsement of the taxi firm) 01303 252 000 01303 270 000 01303 244 442 Further information about all onward travel Local Cycle Info National Cycle Info Bus Times PlusBus See timetable shepway.gov.uk sustrans.org.uk displays at bus Find the bus times for your stop. -
Newsletter.Pdf
E L H A M NEWSLETTE R Published by the Elham Village Hall Association, Charity No 1024757 Also available to read on the EVHA website, www.elhamvillagehall.co.uk. For further information www.elham.co.uk/ visit Elham OCTOBER 2021 Summer Meadow, picture by Hugh Carson, originally sent for ‘Talk on the Wild Side, 2020. What’s On, In and Around ELHAM Date Event Time Location Contact Page Saturday 2nd Elham Gardening Society Coffee Doug Martin 01303 tbc Elham Village Hall 13 October Morning and Bulb Sale 840276 Maggie Tappenden Monday 4th October Short Mat Bowls Begins Again 15.30 -18.00 Elham Village Hall 01303 862467 25 Anna Clayton Jim Clements Monday 4th October Table Tennis for All 19.00 25 Room EVH 01303840295 Wednesday 6th Social, Snacks and Cinema Peggy Pike Room Jan Stanyon 19.00 5 October EVHA Elham Village Hall 01303 840820 ST MARY’S CHURCH HALL Nicki’s Garden Design and Maintenance For parties, for the smaller function Hadlow Horticultural College and for Meetings trained and qualified More than fifteen years experience £12.00 for Mornings and Afternoons Garden Designing and planting from whole garden project to re-designing tired borders £15.00 for Evenings and Saturdays General Maintenance, Weeding, Pruning, Use of Kitchen included Planting, Lawn Mowing, Hedge Cutting Gardening can be provided on a weekly, fortnightly or Bookings: Mrs Pat Holmes seasonal basis 01303 840647 Call Nicki on 07748628993 Email: [email protected] Do you need a helping hand? Garden & Domestic Work House & Pet Sitting Small Animal Care Then please ’phone Fiona Johnson 01303 840507 (working locally for 28 years) Air Link Cars Airport, Seaport & Long Distance Travel Specialist The family run business where service really counts. -
THE LYMINGE NEWSLETTER for the Communities of LYMINGE, ETCHINGHILL, RHODES MINNIS and POSTLING
THE LYMINGE NEWSLETTER For the communities of LYMINGE, ETCHINGHILL, RHODES MINNIS and POSTLING Produced by THE LYMINGE ASSOCIATION November 2017 www.lyminge.org.uk News from The Lyminge Association Forthcoming Events ● Christmas Tree Lights Switch On - 23rd November, outside Laing Bennett Estate Agents. We gather about 4.30pm and sing some carols in the warm up to the arrival of Father Christmas who will switch on the lights at 5pm. ● Delivery of Christmas Parcels - As in previous years, Father Christmas has offered to deliver presents in our area on Friday 22nd December. To help him, we would be grateful if all parcels for delivery were left at Laing Bennett’s Estate Agents in Station Road between 1st December and the FINAL date of 3pm on 20th December. Last year 60+ presents were delivered, so the sooner you drop them off the better. Please ensure the gifts are well wrapped, clearly labelled with the recipients name and address. A small charge of £2 is made per address; so if there is more than one child at that particular address, or Mum and Dad are lucky enough to get a present too, it is still just £2. And hey- presto, Father Christmas delivers them to each address in the early evening of Friday 22nd December. The Magic and Wonder of Christmas aint Nicholas £100 1st Prize Grand S Fayre Draw Saturday 25th November 2017 in St Mary & St. Ethelburga Church Lyminge 11.00am until 2.30pm Bacon Rolls ~ Barbecue ~ Light Lunches ~ Mulled Wine ~ Christmas Gifts ~ Crafts Children’s Games ~ Books ~ Mince Pies ~ Cakes ~ Jams ~ Christmas Music A Traditional Village Christmas Fayre Raising funds for St. -

18 Bus Time Schedule & Line Route
18 bus time schedule & line map 18 Canterbury View In Website Mode The 18 bus line (Canterbury) has 2 routes. For regular weekdays, their operation hours are: (1) Canterbury: 7:15 AM - 5:10 PM (2) Hythe: 8:55 AM - 6:15 PM Use the Moovit App to ƒnd the closest 18 bus station near you and ƒnd out when is the next 18 bus arriving. Direction: Canterbury 18 bus Time Schedule 45 stops Canterbury Route Timetable: VIEW LINE SCHEDULE Sunday Not Operational Monday 7:15 AM - 5:10 PM Hythe Light Railway Station Hythe (DA) Tuesday 7:15 AM - 5:10 PM Sir John Moore Avenue, Hythe Wednesday 7:15 AM - 5:10 PM Red Lion Square, Hythe Thursday 7:15 AM - 5:10 PM Dymchurch Road, Hythe Civil Parish Friday 7:15 AM - 5:10 PM Old Prospect Road, Hythe Prospect Road, Hythe Civil Parish Saturday 7:20 AM - 5:10 PM Douglas Avenue, Hythe A259, Hythe Civil Parish Saltwood Care Centre, Hythe 18 bus Info Tanners Hill, Hythe Civil Parish Direction: Canterbury Stops: 45 Tanner's Hill Gardens, Hythe Trip Duration: 61 min Tanners Hill, Hythe Civil Parish Line Summary: Hythe Light Railway Station Hythe (DA), Sir John Moore Avenue, Hythe, Red Lion School Road, Hythe Square, Hythe, Old Prospect Road, Hythe, Douglas Avenue, Hythe, Saltwood Care Centre, Hythe, Quarry Road, Hythe Tanner's Hill Gardens, Hythe, School Road, Hythe, Quarry Road, Hythe, Hillcrest Road Middle, Hythe, Hillcrest Road Middle, Hythe Hillcrest Road, Saltwood, Brockhill Road, Saltwood, Seaton Avenue, Saltwood, Bartholomew Lane, Hillcrest Road, Saltwood Saltwood, Brockhill Park, Saltwood, Railway Station, Sandling, -

February 2018
FEBRUARY 2018 Published by the Elham Village Hall Association, Charity No 1024757 Lavender House, High Street, Elham CT4 6TB T: 01303 840577 E: [email protected] W: www.bournephysio.co.uk Professional Physiotherapy for multiple conditions and Sports Injuries Julie Perkins, Chartered Physiotherapist MSc, BSc (Hons), BA (Hons), MCSP, MPF, MSOM HCPC registered ETCHINGHILL GOLF Canterbury Road, Etchinghill, Folkestone Licensed for Civil Ceremonies, Weddings, Christenings, Renewal of Wedding Vows and Baby Naming Open to the public for Breakfast, Lunch and Afternoon Tea We have a large function room overlooking our beautiful golf course, perfect for birthday or family celebrations Every Sunday - come and try our delicious carvery in our panoramic restaurant with a creative menu that changes weekly For further details email: [email protected] or telephone 01303 862929 Nicki’s Garden Design Wilco Plumbing & Heating and Maintenance Central Heating Installations & Repairs Hadlow Horticultural College Gas & Oil Boiler repairs & replacements trained and qualified LPG, Solar & Unvented hot water specialist More than fifteen years experience Landlords Gas Safety Inspections Garden Designing and planting from whole garden Local Experienced Engineer project to re-designing tired borders General Maintenance, Weeding, Pruning, Planting Registered with the Institute of Plumbing Lawn Mowing, Hedge Cutting Gas Safe Registered Gardening can be provided on a weekly, fortnightly or 01303 862173 / 07860 452640 seasonal basis Call Nicki on 07748628993