What Our Local Data Tells Us Contents
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

COMPASS Research Centre Barry Milne and Nichola Shackleton
New New Zealand Data Quality of the 2018 New Zealand Census Barry Milne COMPASS Seminar Tuesday, 3 March 2020 The University of Auckland The University of Outline Background to the Census What happened with Census 2018? Why did it happen? What fixes were undertaken? What are the data quality implications? New New Zealand 1. Population counts 2. Electoral implications 3. Use of alternative data sources 4. Poor/very poor quality variables Guidelines for users of the Census The University of Auckland The University of Some recommendations that (I think) should be taken on board 2 Background New Zealand Census of Population and Dwellings Official count of how many people and dwellings there are in the country at a set point in time (by age, sex, ethnicity, region, community) Detailed social, cultural and socio-economic information about the total New Zealand population and key groups in the population Undertaken since 1851, and every five years since 1881, with exceptions New New Zealand • No census during the Great Depression (1931) • No census during the Second World War (1941) • The 1946 Census was brought forward to September 1945 • The Christchurch earthquakes caused the 2011 Census to be re-run in 2013 Since 1966, held on first Tuesday in March of Census year The most recent census was undertaken on March 6, 2018 The University of Auckland The University of http://archive.stats.govt.nz/Census/2013-census/info-about-the-census/intro-to-nz-census/history/history-summary.aspx 3 Background Census is important for Electorates and electoral boundaries Central and local government policy making and monitoring Allocating resources from central government to local areas Academic and market research Statistical benchmarks New New Zealand A data frame to select samples for social surveys Many other things beside… “every dollar invested in the census generates a net benefit of five dollars in the economy” (Bakker, 2014, Valuing the census, p. -

Kapiti Coast District / [email protected] / P
APRIL 2019 KAPITI COAST DISTRICT WWW.INTEREST.CO.NZ / [email protected] / P. 09 3609670 KAPITI COAST DISTRICT HOME LOAN AFFORDABILITY REPORT April 2019 Home loan affordability is a measure of the proportion of take-home pay that is needed to make the mortgage payment for a typical household. If that is less than 40%, then a mortgage is considered ‘affordable’. The following are typical assessments for households at three stages of home ownership. FIRST HOME BUYERS 25-29 YOUNG FAMILY 30-34 OLDER FAMILY 35-39 First home buyers earn a medi- Young family buyers earn medi- Older family buyers earn medi- an income for their age group, an incomes in their age bracket, an incomes in their age brack- and buy a first quartile house and buy a median house in et, and buy a median house in in their area. Both parties work their area. One partner works their area. Both partners work full-time. half-time. full-time. Mortgage payment as a Mortgage payment as a Mortgage payment as a percentage of the take home pay percentage of the take home pay percentage of the take home pay Take Home April 19 29.7% Take Home April 19 29.2% Take Home Pay Pay Pay April 19 17.6% April 18 30.3% April 18 26.8% $1,517.11 $1,334.99 $1,856.59 April 18 17.1% per Week April 17 26.9% per Week April 17 29.2% per Week April 17 19.4% April 14 - April 14 26.0% April 14 33.3% This report estimates how affordable it would be for a couple This report estimates how affordable it would be for a couple This report estimates how affordable it would be for a couple where both are aged 25–29 and are working full time, to buy a with a young family to move up the property ladder and buy their who are both aged 35-39 and working full time, to move up the home at the lower quartile price in Kapiti Coast District. -

Making a Community: Filipinos in Wellington
Making a Community: Filipinos in Wellington September 2017 ISBN 978-0-9941409-4-4 (PDF) Making a Community: Filipinos in Wellington About the Author As an American living in New Zealand, I’ve been observing the debate here on immigration and multiculturalism. I arrived in Wellington last year with my Kiwi husband and three-year old son – and while settling in we’ve spent a lot of time discovering the delights of the city and its people. The experience also gave me some perspective on being a migrant far from home. I have a professional interest in South East Asian history, languages and culture - I just completed a PhD on the subject. I speak some Filipino, and am fascinated by the Philippines’ complex history. One of the major phenomena in the Philippines since the 1970s has been the growth of the global Filipino diaspora. That story has often been full of sadness. So I was intrigued by anecdotes of positivity and success from Wellington. Writing about how the migrant Filipino community has settled in New Zealand has been more than just a research project. It has highlighted how migration plays a role in community building. It also has meaning for me and my family’s future here. I really wanted to share some of the stories that I think reflect successful outcomes from immigration over the past thirty years. By Dr Rebecca Townsend 1 Key Points 1. 2. 3. Filipinos comprise 1 percent of Filipinos are a vital part of Most Filipinos in New Zealand are New Zealand’s population – the New Zealand’s dairy, healthcare, not Overseas Filipino Workers third largest Asian ethnic group construction, nursing, aged care, (OFW). -
Memorandum of Understanding Between
Attachment 1 to Report 06.583 Page 1 of 5 MEMORANDUM OF UNDERSTANDING BETWEEN CAPITAL AND COAST DISTRICT HEALTH BOARD AND KAPITI COAST DISTRICT COUNCIL, PORIRUA CITY COUNCIL, WELLINGTON CITY COUNCIL, AND WELLINGTON REGIONAL COUNCIL PURPOSE The parties to this Memorandum of Understanding (MoU) share a common obligation to enhance the well being and health of people in Kapiti, Porirua and Wellington, and to work with them in building strong, vibrant and healthy communities. This MoU will assist in achieving the Regional Community Outcome: "Healthy Community" as outlined in the Wellington Regional Strategy. This MoU sets out a process to assist co-operation between the above organisations. It is intended that this MoU will: • ensure that resources (people, funding and materials) are used to improve the well being of the communities in Kapiti, Porirua and Wellington • ensure communication between the organisations is open and timely. PROTOCOLS AND PRINCIPLES • the parties will work together on issues where it is agreed that the population of Kapiti, Porirua and Wellington will benefit from a collaborative approach • the MoU acknowledges each organisation's unique accountability and contribution to shared processes • the parties agree to act in good faith on issues of information and disclosure • the parties agree to work collaboratively in an open and transparent manner • the parties agree to build on work currently undertaken within Kapiti, Porirua and Wellington. • the parties acknowledge the role of Regional Public Health (RPH) in delivering regional public health services, and that this MoU will not preclude the development of such relationships by each party with RPH As signatories of this MoU each party will ensure: • early notification to affected parties through the distribution of draft documentation, of major policy discussions, which may have implications beyond the boundaries of the decision-making party. -

The Politics and Practice of Counting
THE POLITICS AND PRACTICE OF COUNTING: Ethnicity in official statistics in Aotearoa/New Zealand Opinions expressed in this report are those of the authors only and do not necessarily reflect policy advice provided by the Ministry of Health, nor represent the views of the peer reviewers or the University of Otago. ISBN 978-0-9583608-9-0 Suggested citation: Cormack D. (2010). The practice and politics of counting: ethnicity data in official statistics in Aotearoa/New Zealand. Wellington: Te Rōpū Rangahau Hauora a Eru Pōmare. This document is available on the website: www.ethnicity.maori.nz Acknowledgments Many thanks to those whose prior work and theorising contributed to the direction of this paper. Thanks also to Bridget Robson and Statistics New Zealand for comments on early drafts of this paper. Thank you to the individuals who provided comment on ethnicity data collection in other key sectors. Thank you to the peer reviewers for valuable comments and feedback: Melissa McLeod, Allanah Ryan, Paula Searle and Natalie Talamaivao. Any errors are the authors. Thank you to Julian Apatu for design of the logo, and to Flax Digital for layout, design and production. This discussion paper is part of a series of discussion papers developed as part of an ethnicity data project funded by Te Kete Hauora at the Ministry of Health. Ngā mihi nui ki a koutou katoa. Table of Contents Introduction ..............................................................................................................................1 Talking ethnicity: definitions -

Kapiti Coast District Council and Other Councils, Including Population Forecasts
Housing and Business Development Capacity Assessment Kāpiti Coast District Council November 2019 Housing and Business Land Capacity Assessment 229 230 Housing and Business Land Capacity Assessment Contents Executive Summary 232 5.0 Infrastructure 270 Background 233 5.1 Three Waters 270 Residential demand 233 5.2 Local Road Network 271 Residential capacity 233 5.3 State Highway Network 272 Business demand 234 5.4 Public Transport 272 Business capacity 234 5.5 Open Space 273 Infrastructure capacity 234 5.6 Education 273 1.0 Introduction 237 6.0 Relationship between Housing and Business Land 274 2.0 Existing Policy Context 238 7.0 Monitoring 275 2.1 Kāpiti Coast District Plan 238 7.1 Historic Development Activity 275 2.2 Development Management Strategy 2007 238 7.2 Market Indicators 278 2.3 Infrastructure Strategy 2018-2048 238 7.3 Price Efficiency Indicators 285 2.4 Roads of National Significance and Town Centres Transformation 239 8.0 Conclusion 293 3.0 Residential Demand and Capacity 240 9.0 Next Actions 294 3.1 Historic urban growth and settlement 240 3.2 Current growth and settlement trends 240 3.3 Future Housing Demand 241 3.4 Housing Development Capacity 248 3.5 Housing Feasibility, Realisation and Sufficiency 251 4.0 Business Demand and Capacity 258 4.1 Business Development Context 258 4.2 Current Economic and Business Drivers 259 4.3 Future Business Demand 260 4.4 Business Development Capacity 264 4.5 Business Feasibility, Realisation and Sufficiency 266 Housing and Business Land Capacity Assessment 231 Executive Summary This report presents the results from the Wellington Region Housing and Business Development Capacity Assessment (HBA) for the Kāpiti Coast District Council. -
STUDENT LIFE HANDBOOK Your Reference Guide As a New Student at IPU New Zealand
STUDENT LIFE HANDBOOK Your reference guide as a new student at IPU New Zealand IPU EMERGENCY CONTACT NUMBER (STUDENT SUPPORT/SECURITY) 0800 355 050 UPDATED JANUARY 2019 WELCOME TO haere mai! CONTENTS INTRODUCTION Campus Map 2 Academic Calendar 2018 4 President’s Welcome 5 Palmerston North and the Manawatu Area 6 Reception & Student Services 8 Academic Learning Support Centre 9 IT Support 10 CAMPUS FACILITIES Dining Hall 12 Junior Common Room 13 Health Clinic – D Block and Medical Facilities 14 Healthy Lifestyle Habits 16 The Importance of Health Insurance 17 Community Support Services 18 Recreation Centre + KAN (Performing Arts Centre) 20 Library 21 Study Centre, Prayer Room, Computer Lab and Bus Stop 22 Security 24 Hall Life 26 Recycling on Campus 29 IMPORTANT POLICY Enrolment 30 Refund Policy 32 Overdue Accounts & Fee Payment Policy 33 English Language Requirements 35 Student Visa 36 Assessment 37 Campus Rules and Regulations 41 Regulations for Driving & Vehicles 43 RULES, ADVICE & GUIDELINES Personal Safety 44 Health & Safety 46 Harassment & Bullying 47 New Zealand Law – What international students need to know 48 IPU Complaints Process 55 NZQA - International Students - How to make a complaint 56 Emergency and Contact Details 62 IPU NEW ZEALAND CAMPUS MAP CAMPUS MAP HALL 6 ADMINISTRATION VISITOR PARKING AREAS HALL 5 STUDENT SUPPORT CAR PARK SP HEALTH CLINIC GATE 5 DISABLED CAR PARK HALL 3 SC STUDY CENTRE HALL 4 SP STUDENT CAR PARK S SECURITY OFFICE LIBRARY B BUS STOP HALL 7 HALL 9 SMOKING AREA BICYCLE PARK Senior HALL 2 Common Room -

Manawatu -Wanganui
Venue No Venue Name Venue Physical Address 98 FOXTON RETURNED SERVICES ASSOCIATION 1 EASTON STREET,FOXTON, MANAWATU 4814,NEW ZEALAND 136 TAUMARUNUI COSMOPOLITAN CLUB CORNER KATARINA AND MIRIAMA STREETS,TAUMARUNUI CENTRAL, TAUMARUNUI 3920,NEW ZEALAND 192 CASTLECLIFF CLUB INC 4 TENNYSON STREET,CASTLECLIFF, WANGANUI DISTRICT 4501,NEW ZEALAND 222 THE OFFICE 514-516 MAIN STREET EAST, PALMERSTON NORTH CENTRAL, PALMERSTON NORTH 5301 223 WILLOW PARK TAVERN 820 TREMAINE AVENUE, PALMERSTON NORTH CENTRAL, PALMERSTON NORTH 5301 225 THE COBB 522-532 MAIN STREET EAST, PALMERSTON NORTH CENTRAL, PALMERSTON NORTH 5301 261 TAUMARUNUI RSA CLUB 10 MARAE STREET,TAUMARUNUI CENTRAL, TAUMARUNUI 3946,NEW ZEALAND 272 DANNEVIRKE SERVICES AND CITIZENS CLUB 1 PRINCESS STREET, DANNEVIRKE, MANAWATU 5491 293 Ohakune Tavern 66-72 CLYDE STREET,OHAKUNE, MANAWATU 4625,NEW ZEALAND 308 THE EMPIRE HOTEL 8 STAFFORD STREET, FEILDING, MANAWATU 5600 347 WANGANUI EAST CLUB 101 WAKEFIELD STREET, WANGANUI, WANGANUI DISTRICT 4540 356 TARARUA CLUB 15 TARARUA STREET, PAHIATUA, MANAWATU 5470 365 OHAKUNE CLUB 71 GOLDFINCH STREET, OHAKUNE, MANAWATU 5461 389 ALBERT SPORTS BAR 692-700 MAIN STREET EAST, PALMERSTON NORTH CENTRAL, PALMERSTON NORTH 5301 394 STELLAR BAR 2 VICTORIA STREET, WANGANUI, WANGANUI DISTRICT 4540 395 FATBOYZ BAR COBB AND CO CORNER DURHAM AND OXFORD STREETS, LEVIN, MANAWATU 5500 410 ASHHURST MEMORIAL RSA 74 CAMBRIDGE AVENUE,ASHHURST, MANAWATU 4847,NEW ZEALAND 431 ST JOHN'S CLUB 158 GLASGOW STREET,WANGANUI, WANGANUI DISTRICT 4500,NEW ZEALAND 439 LEVIN COSMOPOLITAN CLUB 47-51 -

The New Zealand Census– Mortality Study
The New Zealand Census– Mortality Study Socioeconomic inequalities and adult mortality 1991–94 Published in June 2002 by the Ministry of Health PO Box 5013, Wellington, New Zealand ISBN 0-478-27048-8 (Book) ISBN 0-478-27049-6 (Internet) Blakely T. The New Zealand Census–Mortality Study: Socioeconomic inequalities and adult mortality 1991–94. Wellington: Ministry of Health, 2002. This document is available on the Ministry of Health’s website: http://www.moh.govt.nz/phi and the NZCMS website: http:/www.wnmeds.ac.nz/nzcms-info.html Foreword The New Zealand Census - Mortality Study (NZCMS) is the principal instrument by which the Ministry of Health monitors social inequalities in health. This report provides the technical background to the study, as well as illustrative substantive results. The NZCMS is hosted by the Wellington School of Medicine and Health Sciences, University of Otago, and is led by Dr Tony Blakely. The study has been funded by the Health Research Council since 1998, and co-funded by the Ministry of Health since 2001. The study involves anonymous and probabilistic linkage of census and mortality records, thereby creating cohort (or follow-up) studies of the entire New Zealand population for the three years following each census. The NZCMS is conducted in conjunction with Statistics New Zealand. The linking of the two datasets was undertaken by Statistics New Zealand staff, and access to the linked data was provided by Statistics New Zealand under conditions designed to give effect to the security and confidentiality provisions of the Statistics Act 1975. As a census-based cohort study, the NZCMS offers several advantages over other study designs: • direct linkage of exposures to outcomes at the individual level • rich exposure data • great statistical power (because of the large ‘sample’ size). -

The Case of Kapiti Coast District Council
THE NEW ZEALAND MEDICAL JOURNAL Journal of the New Zealand Medical Association Getting an outdoor smokefree policy: the case of Kapiti Coast District Council Leigh Halkett, George Thomson Abstract Aim To explore how a smokefree parks policy was conceived, accepted and developed by and for Kapiti Coast District Council (KCDC). Method Thirteen people involved in the smokefree parks policy process for KCDC were interviewed in person during November–December 2008. Supporting documentation and websites were accessed and reviewed. Results In September 2008 the KCDC agreed to adopt a smokefree parks and playground policy, following an initiative from a smokefree coalition of several public health organisations. The policy was developed collaboratively by this coalition with input from the council, and was supported by key local organisations. The KCDC appears to have adopted a smokefree outdoor areas (SFOA) policy because of demonstrated public support, the relative simplicity and low cost of the policy, the success of similar policies elsewhere, and because of the alignment with desired community outcomes. The challenges included finding funding and allocating staff time for this project. There were also concerns with how the policy would be enforced. Conclusions A collaborative approach amongst health and community groups for achieving SFOA policies works well. The experience with council SFOA policies has considerable impact on the adoption of similar policies by other councils. To maximise this influence, information about the policies needs to be spread nationally by the health and local government sectors. Legislative efforts to reduce smoking and the exposure to secondhand smoke (SHS) in New Zealand have included the Smoke-free Environments Act 1990 (SEA) and the Smoke-free Environments Amendment Act 2003 (SEAA). -
Submitter Contact Details
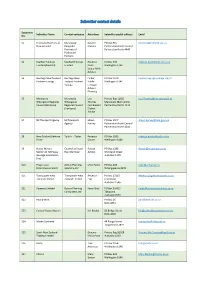
Submitter contact details Submitter Submitter Name Contact company Attention: Submitter postal address Email No. S1 Federated Farmers of Manawatu- Coralee PO Box 945 [email protected] New Zealand Rangitikei Matena Palmerston North Central Province of Palmerston North 4440 Federated Farmers S2 KiwiRail Holdings KiwiRail Holdings Rebecca PO Box 593 [email protected] Limited (KiwiRail) Limited Beals Wellington 6140 Senior RMA Advisor S3 Heritage New Zealand Heritage New Finbar PO Box 2629 [email protected] Pouhere Taonga Zealand Pouhere Kiddle Wellington 6140 Taonga Heritage Adviser- Planning S5 Manawatu- Manawatu- Lisa Private Bag 11025 [email protected] Whanganui Regional Whanganui Thomas Manawatu Mail Centre Council (Horizons) Regional Council Coordinator Palmerston North 4442 (Horizons) District Advice S7 NZ Transport Agency NZ Transport Shaun PO Box 1947 [email protected] Agency Harvey Palmerston North Central Palmerston North 4440 S8 New Zealand Defence Tonkin + Taylor Rebecca PO Box 2083 [email protected] Force Davies Wellington 6140 S9 House Movers Counsel at Stuart Rowan PO Box 1296 [email protected] Section of NZ Heavy Ryan Barrister Ashton Shortland Street Haulage Association Auckland 1140 (Inc) S10 Progressive Zomac Planning Mike Foster PO Box 103 [email protected] Enterprises Limited Solutions Ltd Whangaparoa 0943 S11 Transpower New Transpower New Rebecca PO Box 17215 [email protected] Zealand Limited Zealand Limited Eng Greenlane Auckland 1546 S21 Powerco -

Historic Places in Palmerston North
Historic Places In Palmerston North An inventory of places listed on the Register of the New Zealand Historic Places Trust Pouhere Taonga Historic Places Manawatu-Horowhenua Incorporated 2013 Historic Places in Palmerston North A project of Historic Places Manawatu-Horowhenua Inc. ISSN: 2357-1861 Prepared by: Rosemary Harris Margaret Tate Pat Scrivens First published in Palmerston North 2007; revised 2013. Design: Ess’Dee Associates Ltd. Copyright: Historic Places Manawatu-Horowhenua Inc. You are free to copy this material for non-commercial use. For all other purposes permission is required from Historic Places Manawatu-Horowhenua Inc., PO Box 732, Palmerston North. Historic Places Manawatu-Horowhenua Inc. revised 2013 1 Contents Introduction ........................................................................................................................................................3 Palmerston North Central Business District Regent Theatre .......................................................................................................................................................5 All Saints' Church (Anglican) ...................................................................................................................................7 Cathedral of the Holy Spirit (Catholic) ....................................................................................................................9 Grand Hotel Building (Former)..............................................................................................................................11