Chapter 28 – Mental Health: State Operated Facilities and Services
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

APPENDIX E. LIST of PETTY OFFENSES and MINIMUM FINES APPLICABLE THERETO PURSUANT to L.CR.R. 58.1(C) Table of Contents SUBJECT H
APPENDIX E. LIST OF PETTY OFFENSES AND MINIMUM FINES APPLICABLE THERETO PURSUANT TO L.CR.R. 58.1(c) Table of Contents SUBJECT HEADINGS REFERENCE Motor Vehicle Violations …..…………………………………………………………………..1 Motor Carrier Safety Violations ……..………………………………………………………..2 U.S. Fish and Wildlife Service Statutory and Regulatory Offenses ………….……………..3 Security and Law Enforcement at VA Facilities ……………………………………………..4 1. Motor Vehicle Violations Persons charged with violations of the offenses set forth below may be required to pay the fines set forth below. Certain offenses may also carry a jail term, which is listed in the applicable section of the New Jersey Statutes Annotated. In certain instances, persons charged with such violations may, in lieu of appearance post collateral in the amount indicated for the offense, waive appearance before a Magistrate Judge, and consent to forfeiture of collateral. Persons charged with offenses not listed must appear for trial as in the case of other petty offenses. The collateral and minimum fine for motor vehicle violations committed on the federal enclaves, including military installations, except as otherwise provided by federal law, such as Titles 36 and 50 of the Code of Federal Regulations, is fixed as follows: N.J.S.A Pursuant to New Jersey Statutes Annotated Penalty 39:3-4 Driving or parking unregistered motor vehicle $54 39:3-9a Failure to notify change in name $55 39:3-9a Failure to endorse license $55 39:3-10 Driving with an expired license $54 Driving without a license where offender never licensed in N.J. or $200-500 elsewhere 39:3-10.18(a) Failure to possess a valid CDL $250-500 39:3-10.18(b) Driving a commercial vehicle after license suspended $500-5000 Accident with personal injury while violating this section $5000 39:3-10.24 Refusal to consent to breath samples after arrest for operation of $250-500 commercial vehicle while under influence (N.J.S.A. -

Driver's Licensing Handbook
DRIVER’SDRIVER’S LICENSING HANDBOOK STATE OF WEST VIRGINIA Revised 02/2021 DEPARTMENT OF TRANSPORTATION DIVISION OF MOTOR VEHICLES PO Box 17010 5707 MacCorkle Avenue, SE Charleston, WV 25317 Before you call, please have your license plate number, driver’s license number, and/or your file number ready so that we can assist you as quickly as possible. For Vehicle Title, License Plate, Driver’s License issues, or for General Information (304) 926‑3499 / (800) 642‑9066 | Hearing‑Impaired ‑ (800) 742‑6991 Other Important Telephone Numbers (Area Code 304) Driver’s License ................................................................................................. 926‑3801 Point System .................................................................................................... 926‑2505 Student Attendance ......................................................................................... 926‑2505 Unpaid Tickets .................................................................................................. 926‑2505 Driving Records ................................................................................................ 926‑3952 Compulsory Insurance ...................................................................................... 926‑3802 Driving Under the Influence .............................................................................. 926‑2506 Driving Under the Influence “Interlock” ............................................................ 926‑2507 Visit us on the web at dmv.wv.gov. Need help with reading -

Traffic, Parking and Pedestrian Rules & Regulations
Town of Concord, Massachusetts Traffic, Parking and Pedestrian Rules & Regulations September, 2015 Prepared by: Concord Public Works Engineering Division 133 Keyes Road Concord, MA 01742 The following vote was duly passed: The Select Board of the Town of Concord acting by virtue of the power given to it by Section 22 of Chapter 40 of the General Laws of Massachusetts and by virtue of any other power it hereto enabling, hereby adopts and makes the rules and orders for the regulation of carriages and vehicles used in the said town for regulating traffic upon the streets and highways of said Town of Concord ; insofar as the said rules and orders or any of them are the same as the regulations, rules and orders now in force they shall be deemed to be a continuation thereof. Table of Contents ARTICLE I DEFINITIONS ....................................................................................................................................... 1 ARTICLE II AUTHORITY AND DUTIES OF POLICE ....................................................................................... 5 ARTICLE III TRAFFIC SIGNS, SIGNALS, MARKINGS AND ZONES ............................................................ 7 ARTICLE IV ZONE OF QUIET ............................................................................................................................... 8 ARTICLE V STOPPING, STANDING, PARKING ................................................................................................ 9 ARTICLE VI ONE-WAY STREETS ..................................................................................................................... -
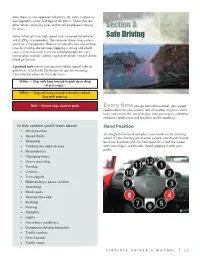
Section 3: Safe Driving
Slow down as you approach toll plazas. Be extra cautious as you approach, enter, and depart toll plazas. There may be other drivers changing lanes and/or toll employees crossing the lanes. Section 3: Some toll roads have high speed lanes reserved for vehicles Safe Driving with E-ZPass transponders. Do not enter those lanes unless you have a transponder. However, if you do enter one of those lanes by mistake, do not stop. Stopping is unsafe and could cause a rear-end crash. Cameras will photograph the car’s license plate number and the registered vehicle’s owner will be billed for the toll. A painted curb means that you must follow special rules to park there. Check with the locality for specific meanings. Generally, the colors on the curb mean: White — Stop only long enough to pick up or drop off passengers. Yellow — Stop only long enough to load or unload. Stay with your car. Red — Do not stop, stand or park. Every time you get behind the wheel, you accept responsibility for your actions. You must obey Virginia’s traffic laws, and ensure the safety of you, your passengers, and other motorists, pedestrians and bicyclists on the roadways. In this section you’ll learn about: Hand Position Hand position Sit straight but relaxed and place your hands on the steering Speed limits wheel. If your steering wheel were a clock, your hands should Stopping be at the 8 o’clock and 4 o’clock positions. Hold the wheel Yielding the right-of-way with your fingers and thumbs. -

School Zone Traffic Laws
Who Receives City of a Ticket? Laguna Niguel Police Services Parking Laws School Zone California Vehicle Code (21458a) Describes Rules for Curb Markings: Parking Enforcement: Traffic RED Curb – indicates no stopping, standing, or parking, The Registered Owner (RO) is the person receiving Laws whether the vehicle is attended or unattended. (No Student the citation, not the driver. The RO is responsible Drop Off or Pick Up in Red Zone). to resolve the citation. If parking citations are not YELLOW Curb – indicates stopping for the loading or unloading cleared, either by dismissal or payment, the RO of passengers or freight, (20 minutes for material & 3 minutes may not be able to renew vehicle registration for passengers). until the citation has been cleared by DMV. Vehicles WHITE Curb – indicates stopping for the loading or unloading that have five or more citations on file are subject What are important traffic of passengers (3 minutes for passengers). to impound, per (CVC 22651i)(1). Compliance laws? with parking restrictions and traffic laws helps GREEN Curb – indicates time limit parking specified by local ordinance (24 & 30 minute zones). provide a safe roadway network in the City of Laguna Niguel. How can I safely drive and BLUE Curb – indicates parking limited exclusively to the vehicle park near schools? of disabled persons Laguna Niguel Police Services (administered by Who is responsible for traffic the Orange County Sheriff’s Department), is violations? responsible for enforcing traffic laws within the City of Laguna Niguel. City of Laguna Niguel Contact Us Police Services for More 30111 Crown Valley Parkway This brochure is designed to answer Information Laguna Niguel, CA 92677 your questions and more. -
Driver Manual Presents Instructions and General Information Relating to the Operation of Motor Vehicles in the State of Oklahoma
NOT TO BE SOLD OklahomaOKLAHOMA DRIVER'S MANUAL September 2017 OurOur studentsstudents don’tdon’t fearfear thethe realreal world.world. They’veThey’ve alreadyalready beenbeen there.there. Real world experience to prepare for life and work— that’s what CareerTech is all about. Whether it is health, marketing, computer technology, agriculture or another career, you can learn skills and gain practical experience to be successful in whatever you choose. You can even earn college credit! Are you ready for the real world? Talk to your counselor about CareerTech, or visit your local technology center today. www.okcareertech.org FOREWORD This handbook is written to help you qualify for an Oklahoma Driver License and become a safe driver. It is not an official legal reference to Oklahoma traffic laws, but explains in everyday language the knowledge and skills you will need to drive safely and legally on Oklahoma’s roads and highways. Good drivers know, understand, and respect the laws and safe-driving practices. They drive defensively and courteously, always seeking to improve their driving skills and habits. If you are an Oklahoma resident, you must have an Oklahoma Driver License to operate a car, truck, or motorcycle. You must pass the required tests for the type of vehicle you want to drive. The tests will be given and evaluated by a professional driver examiner of the Oklahoma Department of Public Safety, according to state and national standards. Your license to operate a motor vehicle on Oklahoma’s streets and highways is a privilege granted by the state under certain conditions. -
Arkansas Driver License Study Guide
ARKANSAS DRIVER LICENSE STUDY GUIDE VOLUME 1 – EDITION 7 August 2015 LITTERING: IT’S AGAINST THE LAW. With a driver license comes the responsibility of being familiar with the laws of the road. As a driver you are accountable for what may be thrown from the vehicle onto a city street or state highway. 8-6-404 PENALTIES (a)(1)(A)(i) A person convicted of a violation of § 8-6-406 or § 8-6-407 for a first offense shall be guilty of an unclassified misdemeanor and shall be fined in an amount of not less than one hundred dollars ($100) and not more than one thousand dollars ($1,000). (ii) An additional sentence of not more than eight (8) hours of community service shall be imposed under this subdivision (a) (1) (A). (B)(i) A person convicted of a violation of § 8-6-406 or § 8-6- court pursuant to this section. 407 for a second or subsequent offense within three (3) years 8-6-407 COMMERCIAL REFUSE HAULING BY of the first offense shall be guilty of an unclassified UNCOVERED VEHICLES misdemeanor and shall be fined in an amount of not less than It shall be unlawful for any person engaged in commercial or two hundred dollars ($200) and not more than two thousand for-hire hauling to operate any truck or other vehicle within dollars ($2,000). this state to transport litter, trash, or garbage unless the (ii) An additional sentence of not more than twenty-four (24) vehicle is covered to prevent its contents from blowing, hours of community service may be imposed under this dropping, falling off, or otherwise departing from the vehicle. -
School Zone Traffic Laws
ARCADIA POLICE DEPARTMENT SCHOOL ZONE TRAFFIC LAWS The Arcadia Police Department Traffic Bureau hopes this 2011‐2012 school year will be exciting and successful. With that in mind, we would like to remind all students and parents of the shared responsibility they have in understanding and obeying traffic laws that help maintain safety in and around our school zones. For this purpose, we have provided a list of the most commonly violated traffic laws in our City’s school zones, allowing you to make a conscious and informed effort to create a safe environment for your fellow students, and or your children. PARKING LAWS California Vehicle Code section 21458(a) describes rules for curb markings. 1. RED Curb indicates no stopping, standing, or parking, whether the vehicle is attended or unattended, (No Student Drop Off or Pick Up in Red Zones) 2. YELLOW Curb indicates stopping for the loading or unloading of passengers or freight (20 Minutes For Material & 3 Minutes For Passengers) 3. WHITE Curb indicates stopping for the loading or unloading of passengers (3 Minutes for Passengers) 4. GREEN Curb indicates time limit parking specified by local ordinance (24 & 30 Minute Zones) 5. BLUE Curb indicates parking limited exclusively to the vehicles of disabled persons V.C. 22500(H) DOUBLE PARKING Prohibits stopping, parking, or standing of any attended/unattended vehicle on the roadway side of any vehicle stopped, parked or standing at the curb or edge of a highway (Often seen as parents drop off/pick up children in the lanes of traffic) V.C. 22500(b) Park in Cross Walk Prohibits the stopping, parking, or standing of any attended/unattended vehicle in a crosswalk V.C. -
Traffic Rules and Orders Table of Contents
TRAFFIC RULES AND ORDERS TABLE OF CONTENTS ARTICLE I DEFINITIONS ARTICLE II AUTHORITY AND DUTIES OF THE POLICE ARTICLE III TRAFFIC SIGNS, SIGNALS, MARKINGS AND ZONES ARTICLE IV ZONES OF QUIET ARTICLE V STOPPING, STANDING AND PARKING ARTICLE V-A TOW AWAY ZONE REGULATION ARTICLE VI ONE-WAY STREETS ARTICLE VII OPERATION OF MOTOR VEHICLES ARTICLE VII-A PEDESTRIAN CONTROL REGULATIONS ARTICLE VIII PENALTIES AND REPEALS SCHEDULE I PARKING SCHEDULE I-A SECTION 1: ON STREET PARKING METER ZONES SECTION 2: OFF-STREET PARKING METER ZONES SECTION 3: PERMIT PARKING ZONES SCHEDULE I-B TOW-AWAY ZONES SCHEDULE II TAXICAB STANDS SCHEDULE III ONE-WAY STREETS SCHEDULE IV ISOLATED STOP SIGNS SCHEDULE V ESTABLISHED PARKING PENALTIES SCHEDULE VI SPEED REGULATIONS SCHEDULE VII TURN RIGHT ON RED PROHIBITED SCHEDULE VIII MUST TURN RIGHT OR LEFT SCHEDULE IX YIELD SIGNS SCHEDULE X FOUR WAY STOP SIGNS WATERTOWN STREET DIRECTORY PRIVATE WAYS APPENDIX 1 CAUTIONARY/INFORMATIONAL SIGNS APPENDIX 2 CHILDRENS SIGNS APPENDIX 3 MISCELLANEOUS SIGNS APPENDIX 4 IN-STREET PEDESTRIAN SAFETY SIGNS APPENDIX 5 TRO FIRE LANES APPENDIX 6 HP PARKING ZONES APPENDIX 7 NO PARKING HERE TO CORNER APPENDIX 8 SCHOOL ZONE SIGNS APPENDIX 9 TRAFFIC SIGNALS APPENDIX 10 CROSSWALKS APPROVED TOWN OF WATERTOWN TRAFFIC RULES AND ORDERS Acting by authority of General Laws Chapter 40, 55 22 and 22A, General Laws Chapter 9OC, and Section 7 of Chapter XI of the Watertown Ordinances, the Town Manager hereby adopts and promulgates the rules and orders for the regulation of motor vehicles used in Watertown and of traffic upon the streets, ways and public places of Watertown which are hereto annexed, the being known as the Traffic Rules and Orders, which shall replace and supersede any prior Traffic Rules and Orders. -

11 ARTICLE 513 Vehicle Operation and Parking
11 ARTICLE 513 Vehicle Operation and Parking View Parking Fines A View Parking Fines B 513.01 Compliance with lawful orders. 513.14 Parking prohibited in specified 513.02 Police and fire police to places. direct traffic. 513.15 Parking at City Hall. 513.03 Towing vehicles obstructing work 513.16 Loading and unloading parked areas; liability for expense. vehicles. 513.04 Stop signals and turns. 513.17 Double parking. 513.05 Driving through procession; 513.18 Handicapped parking. backing and u-turns. 513.19 Compliance with parking signs. 513.06 One-way streets; operation 513.20 Buses and taxicabs; parking and parking. in stands. 513.07 Weight restrictions. 513.21 Repairing of vehicles. 513.08 Oversize or overweight vehicles; 513.22 Disposition of fines and permit fee. forfeitures. 513.09 Spring Garden Memorial Park. 513.23 Enforcement. 513.10 Pedestrians at controlled 513.24 Speed zones. intersections and at Continental 513.25 Parking of inoperable or illegally Square. registered vehicles. 513.11 School children crossing 513.99 Penalty. streets. 513.12 Use of coaster, roller skates and similar devices restricted. 513.13 Boarding or alighting from vehicles. CROSS REFERENCES Rules of the road - see Vehicle Code 75 Pa. C.S.A. §3301 et seq. Prohibited stopping, standing and parking places - see Vehicle Code 75 Pa. C.S.A. §3353 Local police powers - see Vehicle Code 75 Pa. C.S.A. §6109(a) 513.01 COMPLIANCE WITH LAWFUL ORDERS. No person shall refuse or fail to comply with any lawful order, signal or direction of a police officer or of any member of the Fire Department duly appointed or designated by the Director of Public Safety to direct traffic in case of fire or other emergency. -
Traffic Enforcement and Management
BRAINTREE POLICE DEPARTMENT Policy and Procedure Traffic Enforcement and Management 2018-30 Date of Issue: 07/23/2018 Issuing Authority: Review Date : Revised: Chief Paul Shastany Certification Standards: 61.1.2 a-c; 61.1.7 a-c; 61.1.11 Accreditation Standards: 1.2.6; 1.2.7; 61.1.3 a-e; 61.1.4 b-d; 61.1.9 a-e; 61.1.12; 61.2.1 f; 61.3.3 a, b; 61.4.1a-d; 61.4.2; 81.2.4 a Optional Accreditation Standards: 61.1.1 a-f; 61.1.5 a-i; 61.1.6; 61.1.8; 61.1.10; 61.1.13 61.3.2 a-g; 61.4.4; 82.3.5 Policy It is the Braintree Police Department’s policy to accomplish roadway safety goals through traffic law enforcement, investigation, direction, and control. These goals include but are not limited to the following: - Reduction of traffic collisions, fatalities, injuries. - Facilitation of the safe and efficient movement of vehicular and pedestrian traffic. The department will accomplish these goals through a combination of education, enforcement, engineering, and public support. In an effort to limit the frequency of crashes, comprehensive crash investigation and reporting is required. Data gathered from crash reports are the prime source of information for crash prevention programs. It is therefore imperative that proper information be gathered for use in planning, evaluating, and implementing efforts to achieve highway safety goals. Enforcement The ultimate objective of enforcement is to favorably alter the violator’s future driving behavior, thus fostering a climate of safe driving throughout the community. -

Arlington County Code Chapter 14.2 Motor Vehicles and Traffic
ARLINGTON COUNTY CODE MOTOR VEHICLES AND TRAFFIC ARLINGTON COUNTY CODE Chapter 14.2 MOTOR VEHICLES AND TRAFFIC* __________ * Editors Note: Ord. No. 92-33, adopted July 11, 1992, amended former Ch. 14, relative to motor vehicles and traffic, to read as herein set out in Ch. 14.2. The provisions of former Ch. 14 derived from those ordinances listed in the Code Comparative Table as amendatory of Ch. 14. __________ Article I. Motor Vehicle Code Division 1. Generally § 14.2-1. Adoption of State Law. § 14.2-1.1. Definitions. § 14.2-2. Prohibition Against Parking of Vehicles under Certain Conditions. § 14.2-3. Removal and Disposition of Unattended or Abandoned Vehicle. § 14.2-3.1. Authority to Provide for Temporary Removal and Disposition of Vehicles Involved in Accidents. § 14.2-3.2. Leaving Vehicles upon Private Property Prohibited. § 14.2-3.3. Removal or Immobilization of Motor Vehicles Against Which There Are Outstanding Parking Violations; Notice; Repossession. § 14.2-3.4. Disposition of Inoperable Abandoned Vehicles. § 14.2-4. Reserved. § 14.2-5. Unauthorized Displaying Upon a Motor Vehicle of Any Button, Insignia, or Emblem of Certain Associations or Societies. § 14.2-6. Breaking, Injuring, Defacing, Destroying, or Preventing the Operation of a Motor Vehicle, Trailer, or Semitrailer. § 14.2-7. Entering Motor Vehicle or Trailer, or Setting Same in Motion; Exceptions. § 14.2-7.1. Fines for Nonmoving Violations. Division 2. Regulation of Traffic Subdivision A. General Provisions § 14.2-8. Drivers to Obey Signs. § 14.2-8.1. Fine for Use of Commuter Lanes. § 14.2-9.