The Role of Myeloid Cells in Immunity to Malaria
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

New Aspects of Human Trichinellosis: the Impact of New Trichinella Species F Bruschi, K D Murrell
15 REVIEW Postgrad Med J: first published as 10.1136/pmj.78.915.15 on 1 January 2002. Downloaded from New aspects of human trichinellosis: the impact of new Trichinella species F Bruschi, K D Murrell ............................................................................................................................. Postgrad Med J 2002;78:15–22 Trichinellosis is a re-emerging zoonosis and more on anti-inflammatory drugs and antihelminthics clinical awareness is needed. In particular, the such as mebendazole and albendazole; the use of these drugs is now aided by greater clinical description of new Trichinella species such as T papuae experience with trichinellosis associated with the and T murrelli and the occurrence of human cases increased number of outbreaks. caused by T pseudospiralis, until very recently thought to The description of new Trichinella species, such as T murrelli and T papuae, as well as the occur only in animals, requires changes in our handling occurrence of outbreaks caused by species not of clinical trichinellosis, because existing knowledge is previously recognised as infective for humans, based mostly on cases due to classical T spiralis such as T pseudospiralis, now render the clinical picture of trichinellosis potentially more compli- infection. The aim of the present review is to integrate cated. Clinicians and particularly infectious dis- the experiences derived from different outbreaks around ease specialists should consider the issues dis- the world, caused by different Trichinella species, in cussed in this review when making a diagnosis and choosing treatment. order to provide a more comprehensive approach to diagnosis and treatment. SYSTEMATICS .......................................................................... Trichinellosis results from infection by a parasitic nematode belonging to the genus trichinella. -

Pursuing Effective Vaccines Against Cattle Diseases Caused by Apicomplexan Protozoa
CAB Reviews 2021 16, No. 024 Pursuing effective vaccines against cattle diseases caused by apicomplexan protozoa Monica Florin-Christensen1,2, Leonhard Schnittger1,2, Reginaldo G. Bastos3, Vignesh A. Rathinasamy4, Brian M. Cooke4, Heba F. Alzan3,5 and Carlos E. Suarez3,6,* Address: 1Instituto de Patobiologia Veterinaria, Centro de Investigaciones en Ciencias Veterinarias y Agronomicas (CICVyA), Instituto Nacional de Tecnologia Agropecuaria (INTA), Hurlingham 1686, Argentina. 2Consejo Nacional de Investigaciones Cientificas y Tecnologicas (CONICET), C1425FQB Buenos Aires, Argentina. 3Department of Veterinary Microbiology and Pathology, Washington State University, P.O. Box 647040, Pullman, WA, 991664-7040, United States. 4Australian Institute of Tropical Health and Medicine, James Cook University, Cairns, Queensland, 4870, Australia. 5Parasitology and Animal Diseases Department, National Research Center, Giza, 12622, Egypt. 6Animal Disease Research Unit, Agricultural Research Service, USDA, WSU, P.O. Box 646630, Pullman, WA, 99164-6630, United States. ORCID information: Monica Florin-Christensen (orcid: 0000-0003-0456-3970); Leonhard Schnittger (orcid: 0000-0003-3484-5370); Reginaldo G. Bastos (orcid: 0000-0002-1457-2160); Vignesh A. Rathinasamy (orcid: 0000-0002-4032-3424); Brian M. Cooke (orcid: ); Heba F. Alzan (orcid: 0000-0002-0260-7813); Carlos E. Suarez (orcid: 0000-0001-6112-2931) *Correspondence: Carlos E. Suarez. Email: [email protected] Received: 22 November 2020 Accepted: 16 February 2021 doi: 10.1079/PAVSNNR202116024 The electronic version of this article is the definitive one. It is located here: http://www.cabi.org/cabreviews © The Author(s) 2021. This article is published under a Creative Commons attribution 4.0 International License (cc by 4.0) (Online ISSN 1749-8848). Abstract Apicomplexan parasites are responsible for important livestock diseases that affect the production of much needed protein resources, and those transmissible to humans pose a public health risk. -

T Cell and Antibody Responses in Plasmodium Falciparum Malaria and Their Relation To
Doctoral thesis from the Department of Immunology, the Wenner-Gren Institute, Stockholm University, Stockholm, Sweden T cell and antibody responses in Plasmodium falciparum malaria and their relation to disease susceptibility Salah Eldin Farouk Stockholm 2005 SUMMARY Malaria antigen-induced polarization of T cells into effectors Th1 and/or Th2 cells and their subsequent release of cytokines is known to affect antibody production. This thesis includes studies on early innate responses to the parasite, with a focus on γδ T cells, and acquired specific responses in African sympatric ethnic tribes. In the last part of this thesis, a method for enrichment for the asexual blood stages of P. falciparum and their use in in vitro T-cell studies is presented. To investigate mechanisms involved in parasite growth inhibition by γδ T cells, an in vitro system was set up using blood stage parasites co-cultured with differently treated γδ T cells. The results showed that V γ9/ δ2+ γδ T cells inhibited the in vitro growth of P. falciparum parasites whereas CD4 + and CD8 + T cells did not. This inhibition was positively correlated with the expression of cytolytic molecules in the cell lines tested. Anti-granulysin antibodies reversed γδ T cell-mediated inhibition, suggesting a role for granulysin in the parasite growth inhibition. Thus, our data suggest that V γ9/V δ2+ γδ T cells inhibit the parasite growth by a granulysin-exocytosis dependent cytotoxic pathway that needs perforin. To study the humoral responses and their relation to Th1/Th2 cytokine profiles, antibody levels, numbers of cytokine-producing cells and spleen rates were measured in two sympatric tribes living in Mali, the Fulani and the Dogon. -

Humoral Immune Responses of Solomon Islanders to the Merozoite
INFECTION AND IMMUNITY, Mar. 1997, p. 1098–1100 Vol. 65, No. 3 0019-9567/97/$04.0010 Copyright q 1997, American Society for Microbiology Humoral Immune Responses of Solomon Islanders to the Merozoite Surface Antigen 2 of Plasmodium falciparum Show Pronounced Skewing towards Antibodies of the Immunoglobulin G3 Subclass CHRISTINE M. RZEPCZYK,1* KATE HALE,2 NICK WOODROFFE,2 ALBINO BOBOGARE,3 1 4 2 PETER CSURHES, AKIRA ISHII, AND ANTONIO FERRANTE Australian Centre for International and Tropical Health and Nutrition, Queensland Institute of Medical Research, Herston, Brisbane, 4029,1 and Department of Immunopathology, Women’s and Children’s Hospital, and Department of Paediatrics, University of Adelaide, Adelaide, South Australia, 5006,2 Australia; Institute of Medical Training and Research, Honiara, Solomon Islands3; and Department of Medical Zoology, Jichi Medical School, Tochigi 329-04, Japan4 Received 12 August 1996/Returned for modification 2 October 1996/Accepted 11 December 1996 The immunoglobulin G (IgG) subclass distribution of antibodies to merozoite surface antigen 2 of Plasmo- dium falciparum in Solomon Islanders showed marked skewing towards the IgG3 subclass. This was not observed with crude P. falciparum schizont antigen. IgG3 responses may be short-lived and require repeated restimulation for their maintenance. This may be provided by persistent infection (premunition) or new infections. Several antigens of asexual blood-stage Plasmodium falcipa- The significance of these IgE antibodies is unclear. There is no rum have been identified as vaccine candidates because of their evidence that such antibodies are protective. ability to protect against malaria in animal model systems A high proportion of villagers in the Solomon Islands and in and/or because antibodies to them inhibit parasite multiplica- Papua New Guinea (PNG), where P. -

Brief History of Important Immunologic Discoveries and Developments
Brief History of Important Immunologic Discoveries and Developments Year Event Author(s) 1798 Cowpox vaccination Edward Jenner 1866 Wound disinfection Joseph Lister 1876 Discovery of B. antracis, foundation of Robert Koch bacteriology 1880 Discovery of attenuated vaccine by Louis Pasteur invitro passages 1883 Phagocytosis, cellular immunity theory Elie I. I. Metchnikoff 1888 Discovery of bacterial toxins P. P. Emile Roux and Alexandre E. J. Y ersin 1890 Discovery of antitoxins, foundation of Emil A. von Behring and serotherapy Shibasaburo Kitasato 1894 Immunologic bacteriolysis Richard F. J. Pfeiffer and Vasily I. Isaeff 1894 Discovery of antibody and complement Jules J.B. V. Bordet activity as the active factors in bacteriolysis 1896 Discovery of specific agglutination Herbert E. Durham and Max von Gruber 1896 Agglutination test for the diagnosis of Georges F. I. Widal and typhoid (Widal test) Jean-Marie-Athanase Sicard 1900 Formulation of side-chain theory of anti- Paul Ehrlich body formation 1900 Discovery of A, B, 0 blood groups Karl Landsteiner 1900 Development of complement fixation Jules J.B. V. Bordet and reaction Octave Gengou 1902 Discovery of anaphylaxis Charles R. Richet and Paul Portier 1903 Local anaphylaxis due to antibody- Nicholas M. Arthus antigen complex: Arthus reaction 1903 Discovery of opsonization Almroth E. Wright and Steward R. Douglas 440 Brief History of Important Immunologic Discoveries and Developments Year Event Author(s) 1905 Description of serum sickness Clemens von Pirquet and Bela Schick 1910 Introduction of salvarsan, later neo- Paul Ehrlich and Sahachiro Hata salvarsan, foundation of chemotherapy of infections 1910 Development of anaphylaxis test William Schultz (Schultz-Dale) 1914 Formulation of genetic theory of tumor Clarence C. -
WSC 14-15 Conf 25 Layout
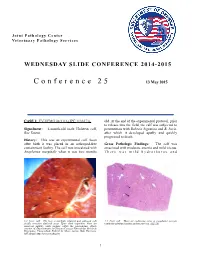
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2014-2015 Conference 25 13 May 2015 CASE I: EV-UFMG 08/1116 (JPC 3136273). old. At the end of the experimental protocol, prior to release into the field, the calf was subjected to Signalment: 4-month-old male Holstein calf, premunition with Babesia bigemina and B. bovis, Bos Taurus. after which it developed apathy and quickly progressed to death. History: This was an experimental calf. Soon after birth it was placed in an arthropod-free Gross Pathologic Findings: The calf was containment facility. The calf was inoculated with emaciated with moderate anemia and mild icterus. Anaplasma marginale when it was two months There was mild hydrothorax and 1-1. Liver, calf: The liver is markedly enlarged and yellowish with 1-2. Liver, calf: There are coalescing areas of coagulative necrosis focally extensive dark-red areas. Upon close inspection, there are within the submitted section of liver (arrows). (HE 5X) numerous military white nodules within the parenchyma. (Photo courtesy of: Departamento de Clínica e Cirurgia Veterinárias, Escola de Veterinária, Universidade Federal de Minas Gerais, Belo Horizonte, MG, Brazil. http://www.vet.ufmg.br) 1 WSC 2014-2015 hydroperitoneum. In the lung there were thickening of the alveolar wall with interstitial multifocal mildly consolidated areas ranging from infiltration of macrophages, lymphocytes and a 0.3 to 0.5 cm in diameter distributed in all few neutrophils. There was multifocal intra- pulmonary lobes. The liver was markedly alveolar accumulation of fibrin and a few enlarged yellowish with focally extensive dark- neutrophils. red areas. -

The Garki Project : Research on the Epidemiology
THE GARKI PROJECT Research on the Epidemiology and Control of Malaria in the Sudan Savanna of West Africa by L. MOLINEAUX and G. GRAMICCIA Medical Officer, Formerly, Chief, Research Coordination, Epidemiological Evaluation Epidemiology and Training, and Assessment, Division of Malaria and Other Parasitic Diseases, World Health Organization ~,~ WORLD HEALTH• ORGANIZATION GENEVA 1980 ISBN 92 4 156061 4 © World Health Organization 1980 Publications of the World Health Organization enjoy copyright protection in accord ance with the provisions of Protocol 2 of the Universal Copyright Convention. For rights ofreproduction or translation of WHO publications, in part or in toto, application should be made to the Office of Publications, World Health Organization, Geneva, Switzerland. The World Health Organization welcomes such applications. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the World Health Organization concerning the legal status of any country, terriiory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. The mention of specific companies or of certain manufacturers' products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. The authors alone are responsible for the views expressed in this publication. TYPESET IN ENGLAND PRINTED IN SWITZERLAND 78/ 4320/ I -6000-ACCENTI AT AR TABLE OF CONTENTS Chapter 1. - Introduction Chapter 2. - The Study Design and Study Area Chapter 3. -

Acquired Immunity to Malaria Denise L
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by DigitalCommons@University of Nebraska University of Nebraska - Lincoln DigitalCommons@University of Nebraska - Lincoln Public Health Resources Public Health Resources 2009 Acquired Immunity to Malaria Denise L. Doolan Queensland Institute of Medical Research, The Bancroft Centre, 300 Herston Road, Post Office Royal Brisbane Hospital, Brisbane, Queensland 4029, Australia Carlota Dobaño Barcelona Centre for International Health Research, Hospital Clínic/IDIBAPS, Universitat de Barcelona, Spain J. Kevin Baird Eijkman-Oxford Clinical Research Unit, Jalan Diponegoro No. 69, Jakarta, Indonesia, [email protected] Follow this and additional works at: http://digitalcommons.unl.edu/publichealthresources Doolan, Denise L.; Dobaño, Carlota; and Baird, J. Kevin, "Acquired Immunity to Malaria" (2009). Public Health Resources. 336. http://digitalcommons.unl.edu/publichealthresources/336 This Article is brought to you for free and open access by the Public Health Resources at DigitalCommons@University of Nebraska - Lincoln. It has been accepted for inclusion in Public Health Resources by an authorized administrator of DigitalCommons@University of Nebraska - Lincoln. CLINICAL MICROBIOLOGY REVIEWS, Jan. 2009, p. 13–36 Vol. 22, No. 1 0893-8512/09/$08.00ϩ0 doi:10.1128/CMR.00025-08 Copyright © 2009, American Society for Microbiology. All Rights Reserved. Acquired Immunity to Malaria Denise L. Doolan,1* Carlota Doban˜o,2 and J. Kevin Baird3,4 Queensland Institute of Medical Research, The Bancroft Centre, 300 Herston Road, Post Office Royal Brisbane Hospital, Brisbane, Queensland 4029, Australia1; Barcelona Centre for International Health Research, Hospital Clínic/IDIBAPS, Universitat de Barcelona, Spain2; Eijkman-Oxford Clinical Research Unit, Jalan Diponegoro No. -
Contributions to the Immunology and Serology of Schistosomiasis Irving G
CONTRIBUTIONS TO THE IMMUNOLOGY AND SEROLOGY OF SCHISTOSOMIASIS IRVING G. KAGAN Commz~nicableDisease Center, Public Health Seruice, Department of Health Education 6 Welfare, Atlanta, Georgia HE superfamily Schistosomatoidea (Stiles & Hassall, 1926: LaRue, T 1957) comprises a large group of trematodes with species parasitizing many classes of the phylum Chordata. What were formerly thought to be three distinct human species, Schistosoma haematobiurn, Schistosoma mansoni and Schistosoma japonicum, are believed today to be complexes of closely related species or varieties which infect man and lower animals (Kuntz, 1955). With the incidence of malaria decreasing in the world, schistosorniasis is becoming one of the more important parasitic diseases of the human race. MilIions of people are infected in the Middle East, the Orient, Africa, and South America. The economic toll and loss of productivity which schistosomiasis causes in these areas of the world makes it important that we study and understand the biology, physiology, epidemiology and host-parasite relationships of these parasites. Armed with this knowledge we may hope to establish effective control procedures to eradicate or alleviate manifestations of this disease. In recent years advances made in the chemotherapy of schistosomiasis make it important the Immunology of the disease be better understood. Increasingly larger groups of people are being treated in endemic areas and the effect of treatment on resistance and immunity toward this infec- tion has not been thoroughly evaluated. To this day, the mechanisms of immunity against schistosomiasis in man and animals are still obscure. In this paper contributions made on the immunology and serology of schistosomiasis by the author and his co-workers will be reviewed. -
Lesson 55. Immunity
MODULE Immunity Microbiology 55 Notes IMMUNITY 55.1 INTRODUCTION The term “immunity” is referred to the resistance of an individual towards injury caused by microorganisms and their products. Immunity against infections is of different types which will be dealt in detail in following sections. OBJECTIVES After reading this lesson, you will be able to: z describe the concepts of innate immunity and acquired immunity z list the types of innate immunity and acquired immunity z explain the mechanism of innate immunity z explain the differences between active and passive immunity 55.2 INNATE IMMUNITY : RESISTANCE TO INFECTIONS THAT AN INDIVIDUAL POSSESSES DUE TO HIS GENETIC MAKEUP Nonspecific immunity – It indicates a degree of resistance to infections in general. z Species immunity – Refers to the resistance to a pathogen shown by all members of a species for example all human beings are totally unsusceptible to plant pathogens. z Racial immunity – Different races within a species, may show differences in susceptibility to infections for example in some parts of Africa resistance to Plasmodium falciparum malaria is seen. 484 MICROBIOLOGY Immunity MODULE z Individual immunity – It is the difference in innate immunity shown by Microbiology different individuals within a race. Several factors such as age, hormones and nutrition influence the level of innate immunity in an individual. Age: The very young and very old are more prone to infectious diseases than the rest. The fetus in utero is normally protected by placental barrier. But some pathogens cross this barrier. Some, such as rubella virus, herpes viruses, cytomegaloviruses and parasite Toxoplasma gondii, can lead to congenital Notes infections. -

Of the Antigenicanalysis of Plasmodia*
Bull. Org. mond. Sant) 1969, Bull. Wld Hlth Org. 40, 55-56 Current Status of the Immunology of Malaria and of the Antigenic Analysis of Plasmodia* A Five-Year Review AVIVAH ZUCKERMAN 1 The immunology of malaria has been intensively studied, and many reviews ofseparate topics have appeared. Among hostfactors contributing to susceptibility to malaria, thefol- lowing are studied in the present paper: (1) genetic factors affecting susceptibility to human and rodent plasmodia; (2) physiological and nutritional factors affecting suscep- tibility of vertebrate and vector hosts; (3) sterile immunity in malaria as exemplified by radical cure and by modification of challenge infection following exposure to non-living parasiteproducts; (4) the role ofthe lymphoid-macrophage system in malaria ; and (S) the excessive anaemia of malaria and its etiology. Gamma-globulin levels rise in malaria and remain high during latency. Protection is associated with IgG, which ispassively transferable via the human placenta. Not allgamma- globulin is antibody, and not all antibody is protective. The fluorescent antibody technique and double diffusion in gel have been extensively used in exploring the kinetics ofantibody production. New methods of harvesting plasmodia attempt to avoid protein degradation and to minimize contamination by host antigens. Plasmodia have proven to consist ofa mosaic of antigens, and comparative studies by most of the accepted techniques have been started. Exoantigens have been described in fowl- and rodent-malarias. Relapse-variants of primate plasmodia have been shown to differ antigenicallyfrom their parent strains. INTRODUCTION Reed Army Institute of Research, Washington, USA; 3 and the report of a WHO Scientific During the past 5 years there has been very Group on the Immunology of Malaria (1968). -

On the Immunology of Trypanosomiasis
Bull. Org. mond. Sante 1967, 37, 167-175 Bull. Wld Hlth Org. Trends in Research on the Immunology of Trypanosomiasis W. H. R. LUMSDEN 1 It was thought timely, in view of the increasingly close association between immunology and parasitology, to attempt a synthesis of research on trypanosomiasis immunology- research which may be expected both to lead to the solution ofpractical problems in this disease and to provide models for the study of basic immunological problems. The author's discussion is based onfour main applications ofimmunological knowledge: for diagnosis, for immunization of hosts, for explanation ofpathological effects, and as a contribution to the understanding of cell function. Stress is laid on the importance of determining the range and extent of antigenic variation in trypanosome material, whether with a view to the development ofreliable diagnostic tests (although quantitative estimation of IgM in serum and cerebrospinal fluid is a useful diagnostic tool circumventing the difficulties caused by antigenic variation during an infection) or for assessment of the possibility of developing antitrypanosomal vaccines. Emphasis is also placed, inter alia, on the need for standardization and determination of the purity of stabilate material exchanged between research laboratories. The history of research into immunological for the measurement of the infective potentiality, as aspects of trypanosomiasis is a long one; it is not to distinct from the organismal concentration, of be thought that interest in these aspects has only trypanosomes (Lumsden et al., 1963). These latter arisen contemporaneously with the extraordinary innovations derive directly from fields of research enlargement of interest in immunology as an indi- other than the purely protozoological-namely, vidual discipline which has occurred in the last artificial insemination and virology--which fact decade.