Meta-Analysis Understanding Systematic Reviews
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Adaptive Clinical Trials: an Introduction
Adaptive clinical trials: an introduction What are the advantages and disadvantages of adaptive clinical trial designs? How and why were Introduction adaptive clinical Adaptive clinical trial design is trials developed? becoming a hot topic in healthcare research, with some researchers In 2004, the FDA published a report arguing that adaptive trials have the on the problems faced by the potential to get new drugs to market scientific community in developing quicker. In this article, we explain new medical treatments.2 The what adaptive trials are and why they report highlighted that the pace of were developed, and we explore both innovation in biomedical science is the advantages of adaptive designs outstripping the rate of advances and the concerns being raised by in the available technologies and some in the healthcare community. tools for evaluating new treatments. Outdated tools are being used to assess new treatments and there What are adaptive is a critical need to improve the effectiveness and efficiency of clinical trials? clinical trials.2 The current process for developing Adaptive clinical trials enable new treatments is expensive, takes researchers to change an aspect a long time and in some cases, the of a trial design at an interim development process has to be assessment, while controlling stopped after significant amounts the rate of type 1 errors.1 Interim of time and resources have been assessments can help to determine invested.2 In 2006, the FDA published whether a trial design is the most a “Critical Path Opportunities -

Cebm-Levels-Of-Evidence-Background-Document-2-1.Pdf
Background document Explanation of the 2011 Oxford Centre for Evidence-Based Medicine (OCEBM) Levels of Evidence Introduction The OCEBM Levels of Evidence was designed so that in addition to traditional critical appraisal, it can be used as a heuristic that clinicians and patients can use to answer clinical questions quickly and without resorting to pre-appraised sources. Heuristics are essentially rules of thumb that helps us make a decision in real environments, and are often as accurate as a more complicated decision process. A distinguishing feature is that the Levels cover the entire range of clinical questions, in the order (from top row to bottom row) that the clinician requires. While most ranking schemes consider strength of evidence for therapeutic effects and harms, the OCEBM system allows clinicians and patients to appraise evidence for prevalence, accuracy of diagnostic tests, prognosis, therapeutic effects, rare harms, common harms, and usefulness of (early) screening. Pre-appraised sources such as the Trip Database (1), (2), or REHAB+ (3) are useful because people who have the time and expertise to conduct systematic reviews of all the evidence design them. At the same time, clinicians, patients, and others may wish to keep some of the power over critical appraisal in their own hands. History Evidence ranking schemes have been used, and criticised, for decades (4-7), and each scheme is geared to answer different questions(8). Early evidence hierarchies(5, 6, 9) were introduced primarily to help clinicians and other researchers appraise the quality of evidence for therapeutic effects, while more recent attempts to assign levels to evidence have been designed to help systematic reviewers(8), or guideline developers(10). -

The Hierarchy of Evidence Pyramid
The Hierarchy of Evidence Pyramid Available from: https://www.researchgate.net/figure/Hierarchy-of-evidence-pyramid-The-pyramidal-shape-qualitatively-integrates-the- amount-of_fig1_311504831 [accessed 12 Dec, 2019] Available from: https://journals.lww.com/clinorthop/Fulltext/2003/08000/Hierarchy_of_Evidence__From_Case_Reports_to.4.aspx [accessed 14 March 2020] CLINICAL ORTHOPAEDICS AND RELATED RESEARCH Number 413, pp. 19–24 © 2003 Lippincott Williams & Wilkins, Inc. Hierarchy of Evidence: From Case Reports to Randomized Controlled Trials Brian Brighton, MD*; Mohit Bhandari, MD, MSc**; Downloaded from https://journals.lww.com/clinorthop by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3oaxD/v Paul Tornetta, III, MD†; and David T. Felson, MD* In the hierarchy of research designs, the results This hierarchy has not been supported in two re- of randomized controlled trials are considered cent publications in the New England Journal of the highest level of evidence. Randomization is Medicine which identified nonsignificant differ- the only method for controlling for known and ences in results between randomized, controlled unknown prognostic factors between two com- trials, and observational studies. The current au- parison groups. Lack of randomization predis- thors provide an approach to organizing pub- poses a study to potentially important imbal- lished research on the basis of study design, a hi- ances in baseline characteristics between two erarchy of evidence, a set of principles and tools study groups. There is a hierarchy of evidence, that help clinicians distinguish ignorance of evi- with randomized controlled trials at the top, con- dence from real scientific uncertainty, distin- trolled observational studies in the middle, and guish evidence from unsubstantiated opinions, uncontrolled studies and opinion at the bottom. -

Quasi-Experimental Studies in the Fields of Infection Control and Antibiotic Resistance, Ten Years Later: a Systematic Review
HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Infect Control Manuscript Author Hosp Epidemiol Manuscript Author . Author manuscript; available in PMC 2019 November 12. Published in final edited form as: Infect Control Hosp Epidemiol. 2018 February ; 39(2): 170–176. doi:10.1017/ice.2017.296. Quasi-experimental Studies in the Fields of Infection Control and Antibiotic Resistance, Ten Years Later: A Systematic Review Rotana Alsaggaf, MS, Lyndsay M. O’Hara, PhD, MPH, Kristen A. Stafford, PhD, MPH, Surbhi Leekha, MBBS, MPH, Anthony D. Harris, MD, MPH, CDC Prevention Epicenters Program Department of Epidemiology and Public Health, University of Maryland School of Medicine, Baltimore, Maryland. Abstract OBJECTIVE.—A systematic review of quasi-experimental studies in the field of infectious diseases was published in 2005. The aim of this study was to assess improvements in the design and reporting of quasi-experiments 10 years after the initial review. We also aimed to report the statistical methods used to analyze quasi-experimental data. DESIGN.—Systematic review of articles published from January 1, 2013, to December 31, 2014, in 4 major infectious disease journals. METHODS.—Quasi-experimental studies focused on infection control and antibiotic resistance were identified and classified based on 4 criteria: (1) type of quasi-experimental design used, (2) justification of the use of the design, (3) use of correct nomenclature to describe the design, and (4) statistical methods used. RESULTS.—Of 2,600 articles, 173 (7%) featured a quasi-experimental design, compared to 73 of 2,320 articles (3%) in the previous review (P<.01). Moreover, 21 articles (12%) utilized a study design with a control group; 6 (3.5%) justified the use of a quasi-experimental design; and 68 (39%) identified their design using the correct nomenclature. -

A Guide to Systematic Review and Meta-Analysis of Prediction Model Performance
RESEARCH METHODS AND REPORTING A guide to systematic review and meta-analysis of prediction model performance Thomas P A Debray,1,2 Johanna A A G Damen,1,2 Kym I E Snell,3 Joie Ensor,3 Lotty Hooft,1,2 Johannes B Reitsma,1,2 Richard D Riley,3 Karel G M Moons1,2 1Cochrane Netherlands, Validation of prediction models is diagnostic test accuracy studies. Compared to therapeu- University Medical Center tic intervention and diagnostic test accuracy studies, Utrecht, PO Box 85500 Str highly recommended and increasingly there is limited guidance on the conduct of systematic 6.131, 3508 GA Utrecht, Netherlands common in the literature. A systematic reviews and meta-analysis of primary prognosis studies. 2Julius Center for Health review of validation studies is therefore A common aim of primary prognostic studies con- Sciences and Primary Care, cerns the development of so-called prognostic predic- University Medical Center helpful, with meta-analysis needed to tion models or indices. These models estimate the Utrecht, PO Box 85500 Str 6.131, 3508 GA Utrecht, summarise the predictive performance individualised probability or risk that a certain condi- Netherlands of the model being validated across tion will occur in the future by combining information 3Research Institute for Primary from multiple prognostic factors from an individual. Care and Health Sciences, Keele different settings and populations. This Unfortunately, there is often conflicting evidence about University, Staffordshire, UK article provides guidance for the predictive performance of developed prognostic Correspondence to: T P A Debray [email protected] researchers systematically reviewing prediction models. For this reason, there is a growing Additional material is published demand for evidence synthesis of (external validation) online only. -

Causality in Medicine with Particular Reference to the Viral Causation of Cancers
Causality in medicine with particular reference to the viral causation of cancers Brendan Owen Clarke A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy of UCL Department of Science and Technology Studies UCL August 20, 2010 Revised version January 24, 2011 I, Brendan Owen Clarke, confirm that the work presented in this thesis is my own. Where information has been derived from other sources, I confirm that this has been indicated in the thesis. ................................................................ January 24, 2011 2 Acknowledgements This thesis would not have been written without the support and inspiration of Donald Gillies, who not only supervised me, but also introduced me to history and philosophy of science in the first instance. I have been very privileged to be the beneficiary of so much of his clear thinking over the last few years. Donald: thank you for everything, and I hope this thesis lives up to your expectations. I am also extremely grateful to Michela Massimi, who has acted as my second supervisor. She has provided throughout remarkably insightful feedback on this project, no matter how distant it is from her own research interests. I’d also like to thank her for all her help and guidance on teaching matters. I should also thank Vladimir Vonka for supplying many important pieces of both the cervical cancer history, as well as his own work on causality in medicine from the perspective of a real, working medical researcher. Phyllis McKay-Illari provided a critical piece of the story, as well as many interesting and stim- ulating discussions about the more philosophical aspects of this thesis. -
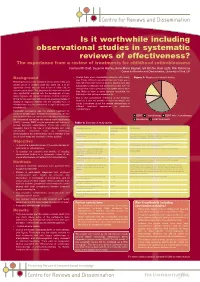
Is It Worthwhile Including Observational Studies in Systematic Reviews of Effectiveness?
CRD_mcdaid05_Poster.qxd 13/6/05 5:12 pm Page 1 Is it worthwhile including observational studies in systematic reviews of effectiveness? The experience from a review of treatments for childhood retinoblastoma Catriona Mc Daid, Suzanne Hartley, Anne-Marie Bagnall, Gill Ritchie, Kate Light, Rob Riemsma Centre for Reviews and Dissemination, University of York, UK Background • Overall there were considerable problems with quality Figure 1: Mapping of included studies (see Table). Without randomised allocation there was a Retinoblastoma is a rare malignant tumour of the retina and high risk of selection bias in all studies. Studies were also usually occurs in children under two years old. It is an susceptible to detection and performance bias, with the aggressive tumour that can lead to loss of vision and, in retrospective studies particularly susceptible as they were extreme cases, death. The prognoses for vision and survival less likely to have a study protocol specifying the have significantly improved with the development of more intervention and outcome assessments. timely diagnosis and improved treatment methods. Important • Due to the considerable limitations of the evidence clinical factors associated with prognosis are age and stage of identified, it was not possible to make meaningful and disease at diagnosis. Patients with the hereditary form of robust conclusions about the relative effectiveness of retinoblastoma may be predisposed to significant long-term different treatment approaches for childhood complications. retinoblastoma. Historically, enucleation was the standard treatment for unilateral retinoblastoma. In bilateral retinoblastoma, the eye ■ ■ ■ with the most advanced tumour was commonly removed and EBRT Chemotherapy EBRT with Chemotherapy the contralateral eye treated with external beam radiotherapy ■ Enucleation ■ Local Treatments (EBRT). -

How to Get Started with a Systematic Review in Epidemiology: an Introductory Guide for Early Career Researchers
Denison et al. Archives of Public Health 2013, 71:21 http://www.archpublichealth.com/content/71/1/21 ARCHIVES OF PUBLIC HEALTH METHODOLOGY Open Access How to get started with a systematic review in epidemiology: an introductory guide for early career researchers Hayley J Denison1*†, Richard M Dodds1,2†, Georgia Ntani1†, Rachel Cooper3†, Cyrus Cooper1†, Avan Aihie Sayer1,2† and Janis Baird1† Abstract Background: Systematic review is a powerful research tool which aims to identify and synthesize all evidence relevant to a research question. The approach taken is much like that used in a scientific experiment, with high priority given to the transparency and reproducibility of the methods used and to handling all evidence in a consistent manner. Early career researchers may find themselves in a position where they decide to undertake a systematic review, for example it may form part or all of a PhD thesis. Those with no prior experience of systematic review may need considerable support and direction getting started with such a project. Here we set out in simple terms how to get started with a systematic review. Discussion: Advice is given on matters such as developing a review protocol, searching using databases and other methods, data extraction, risk of bias assessment and data synthesis including meta-analysis. Signposts to further information and useful resources are also given. Conclusion: A well-conducted systematic review benefits the scientific field by providing a summary of existing evidence and highlighting unanswered questions. For the individual, undertaking a systematic review is also a great opportunity to improve skills in critical appraisal and in synthesising evidence. -

Guidelines for Reporting Meta-Epidemiological Methodology Research
EBM Primer Evid Based Med: first published as 10.1136/ebmed-2017-110713 on 12 July 2017. Downloaded from Guidelines for reporting meta-epidemiological methodology research Mohammad Hassan Murad, Zhen Wang 10.1136/ebmed-2017-110713 Abstract The goal is generally broad but often focuses on exam- Published research should be reported to evidence users ining the impact of certain characteristics of clinical studies on the observed effect, describing the distribu- Evidence-Based Practice with clarity and transparency that facilitate optimal tion of research evidence in a specific setting, exam- Center, Mayo Clinic, Rochester, appraisal and use of evidence and allow replication Minnesota, USA by other researchers. Guidelines for such reporting ining heterogeneity and exploring its causes, identifying are available for several types of studies but not for and describing plausible biases and providing empirical meta-epidemiological methodology studies. Meta- evidence for hypothesised associations. Unlike classic Correspondence to: epidemiological studies adopt a systematic review epidemiology, the unit of analysis for meta-epidemio- Dr Mohammad Hassan Murad, or meta-analysis approach to examine the impact logical studies is a study, not a patient. The outcomes Evidence-based Practice Center, of certain characteristics of clinical studies on the of meta-epidemiological studies are usually not clinical Mayo Clinic, 200 First Street 6–8 observed effect and provide empirical evidence for outcomes. SW, Rochester, MN 55905, USA; hypothesised associations. The unit of analysis in meta- In this guide, we adapt the items used in the PRISMA murad. mohammad@ mayo. edu 9 epidemiological studies is a study, not a patient. The statement for reporting systematic reviews and outcomes of meta-epidemiological studies are usually meta-analysis to fit the setting of meta- epidemiological not clinical outcomes. -

A Meta-Review of Transparency and Reproducibility-Related Reporting Practices in Published Meta- Analyses on Clinical Psychological Interventions (2000-2020)
A meta-review of transparency and reproducibility-related reporting practices in published meta- analyses on clinical psychological interventions (2000-2020). Rubén López-Nicolás1, José Antonio López-López1, María Rubio-Aparicio2 & Julio Sánchez- Meca1 1 Universidad de Murcia (Spain) 2 Universidad de Alicante (Spain) Author note: This paper has been published at Behavior Research Methods. The published version is available at: https://doi.org/10.3758/s13428-021-01644-z. All materials, data, and analysis script coded have been made publicly available on the Open Science Framework: https://osf.io/xg97b/. Correspondence should be addressed to Rubén López-Nicolás, Facultad de Psicología, Campus de Espinardo, Universidad de Murcia, edificio nº 31, 30100 Murcia, España. E-mail: [email protected] 1 Abstract Meta-analysis is a powerful and important tool to synthesize the literature about a research topic. Like other kinds of research, meta-analyses must be reproducible to be compliant with the principles of the scientific method. Furthermore, reproducible meta-analyses can be easily updated with new data and reanalysed applying new and more refined analysis techniques. We attempted to empirically assess the prevalence of transparency and reproducibility-related reporting practices in published meta-analyses from clinical psychology by examining a random sample of 100 meta-analyses. Our purpose was to identify the key points that could be improved with the aim to provide some recommendations to carry out reproducible meta-analyses. We conducted a meta-review of meta-analyses of psychological interventions published between 2000 and 2020. We searched PubMed, PsycInfo and Web of Science databases. A structured coding form to assess transparency indicators was created based on previous studies and existing meta-analysis guidelines. -

Adaptive Designs in Clinical Trials: Why Use Them, and How to Run and Report Them Philip Pallmann1* , Alun W
Pallmann et al. BMC Medicine (2018) 16:29 https://doi.org/10.1186/s12916-018-1017-7 CORRESPONDENCE Open Access Adaptive designs in clinical trials: why use them, and how to run and report them Philip Pallmann1* , Alun W. Bedding2, Babak Choodari-Oskooei3, Munyaradzi Dimairo4,LauraFlight5, Lisa V. Hampson1,6, Jane Holmes7, Adrian P. Mander8, Lang’o Odondi7, Matthew R. Sydes3,SofíaS.Villar8, James M. S. Wason8,9, Christopher J. Weir10, Graham M. Wheeler8,11, Christina Yap12 and Thomas Jaki1 Abstract Adaptive designs can make clinical trials more flexible by utilising results accumulating in the trial to modify the trial’s course in accordance with pre-specified rules. Trials with an adaptive design are often more efficient, informative and ethical than trials with a traditional fixed design since they often make better use of resources such as time and money, and might require fewer participants. Adaptive designs can be applied across all phases of clinical research, from early-phase dose escalation to confirmatory trials. The pace of the uptake of adaptive designs in clinical research, however, has remained well behind that of the statistical literature introducing new methods and highlighting their potential advantages. We speculate that one factor contributing to this is that the full range of adaptations available to trial designs, as well as their goals, advantages and limitations, remains unfamiliar to many parts of the clinical community. Additionally, the term adaptive design has been misleadingly used as an all-encompassing label to refer to certain methods that could be deemed controversial or that have been inadequately implemented. We believe that even if the planning and analysis of a trial is undertaken by an expert statistician, it is essential that the investigators understand the implications of using an adaptive design, for example, what the practical challenges are, what can (and cannot) be inferred from the results of such a trial, and how to report and communicate the results. -

Evidence Based Policymaking’ in a Decentred State Abstract
Paul Cairney, Professor of Politics and Public Policy, University of Stirling, UK [email protected] Paper accepted for publication in Public Policy and Administration 21.8.19 Special Issue (Mark Bevir) The Decentred State The myth of ‘evidence based policymaking’ in a decentred state Abstract. I describe a policy theory story in which a decentred state results from choice and necessity. Governments often choose not to centralise policymaking but they would not succeed if they tried. Many policy scholars take this story for granted, but it is often ignored in other academic disciplines and wider political debate. Instead, commentators call for more centralisation to deliver more accountable, ‘rational’, and ‘evidence based’ policymaking. Such contradictory arguments, about the feasibility and value of government centralisation, raise an ever-present dilemma for governments to accept or challenge decentring. They also accentuate a modern dilemma about how to seek ‘evidence-based policymaking’ in a decentred state. I identify three ideal-type ways in which governments can address both dilemmas consistently. I then identify their ad hoc use by UK and Scottish governments. Although each government has a reputation for more or less centralist approaches, both face similar dilemmas and address them in similar ways. Their choices reflect their need to appear to be in control while dealing with the fact that they are not. Introduction: policy theory and the decentred state I use policy theory to tell a story about the decentred state. Decentred policymaking may result from choice, when a political system contains a division of powers or a central government chooses to engage in cooperation with many other bodies rather than assert central control.