Final Report May 21, 2018
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Democratic Republic of the Congo (DRC) Reports Children in Need of Humanitarian Assistance Its First COVID-19 Confirmed Case
ef Democratic Republic of the Congo Humanitarian Situation Report No. 03 © UNICEF/UN0231603/Herrmann Reporting Period: March 2020 Highlights Situation in Numbers 9,100,000 • 10 March, the Democratic Republic of the Congo (DRC) reports children in need of humanitarian assistance its first COVID-19 confirmed case. As of 31 March 2020, 109 confirmed cases have been recorded, of which 9 deaths and 3 (OCHA, HNO 2020) recovered patients have been reported. During the reporting period, the virus has affected the province of Kinshasa and North Kivu 15,600,000 people in need • In addition to UNICEF’s Humanitarian Action for Children (HAC) (OCHA, HNO 2020) 2020 appeal of $262 million, UNICEF’s COVID-19 response plan has a funding appeal of $58 million to support UNICEF’s response 5,010,000 in WASH/Infection Prevention and Control, risk communication, and community engagement. UNICEF’s response to COVID-19 Internally displaced people can be found on the following link (HNO 2020) 6,297 • During the reporting period, 26,789 in cholera-prone zones and cases of cholera reported other epidemic-affected areas benefiting from prevention and since January response WASH packages (Ministry of Health) UNICEF’s Response and Funding Status UNICEF Appeal 2020 9% US$ 262 million 11% 21% Funding Status (in US$) 15% Funds Carry- received forward, 10% $5.5 M $28.8M 10% 49% 21% 15% Funding gap, 3% $229.3M 0% 20% 40% 60% 80% 100% 1 Funding Overview and Partnerships UNICEF appeals for US$ 262M to sustain the provision of humanitarian services for women and children in the Democratic Republic of the Congo (DRC). -

IMCK Newsletter 17.3.Pages
INSTITUT MEDICAL CHRETIEN DU KASAI !1 OFINSTITUT MEDICAL!5 CHRETIEN DU KASAI B.P. 205 KANANGA B.P. 205 KANANGA INSTITUT MEDICAL CHRETIENREPUBLIQUE DEMOCRATIQUE DU DUKASAI CONGO REPUBLIQUE DEMOCRATIQUE DU CONGO Christian Medical Institute Hôpitalof – theEcole d’infirmiers Kasai – Ecole de laborantins - Serving – Service de santé communautairein Central - Service d’ophtalmologie Congo Service dentaire – Centre d’études et de recyclage Hôpital – Ecole d’infirmiers – Ecole de laborantins – Service de santé communautaire - Service d’ophtalmologie E-mail : [email protected] Service dentaire – Centre d’études et de recyclage B. P. 205 Kananga, Republic Democratic du Congo ; Email: [email protected] E-mail : [email protected] 2. Find a way to channel a greater percentage of donations back into that unpopular category 2. Find a way to channel a greater percentage of donations back into that unpopular category of “undesignated” gifts so that we can have the flexibility to apply them where A Periodic Newsletter operational needs are Issuethe most desperate. No. 41 But ifJanuary you cannot (and - thatMarch is understandable, 2017 of “undesignated” gifts so that we can have the flexibility to apply them whereA considering all the news stories one sees about mismanaged funds), then consider operational needs are the most desperate. But if you cannot (and that is understandable, designating gifts carefully to those things that are at the core of IMCK’s operational considering all the news stories one sees about mismanaged funds), then consider The current conflict in the Kasai has needs.I askedFor example the new: Specify IMCK money Administrator, for medicines and Kastin medical Katawa, supplies; Specifyto describe money designating gifts carefully to those things that are at the core of IMCK’s operational added new suffering and danger. -

Introduction Generale
P a g e | 1 INTRODUCTION GENERALE 0.1. Problématique Le présent mémoire porte sur les logotypes et la signification : Analyse de la dénotation et de la connotation des logotypes des banques Trust Merchant Bank (TMB) et Rawbank. En effet, Sperber1 dit qu’il n’y a rien de plus banal que la communication, car les êtres humains sont par nature des êtres communiquant par la parole, le geste, l’écrit, l’habillement et voire le silence, etc. La célèbre école de Palo Alto le dit tout haut aussi: on ne peut pas ne pas communiquer, tout est communication2. La communication, nous la pratiquons tous les jours sans y penser (mais également en y pensant) et généralement avec un succès assez impressionnant, même si parfois nous sommes confrontés à ses limites et à ses échecs. La communication demeure l’élément fondamental et complexe de la vie sociale qui rend possible l’interaction des personnes et dont la caractéristique essentielle est, selon Daniel Lagache3, la réciprocité. Elle est ce par quoi une personne influence une autre et en est influencée, car elle n’est pas indépendante des effets de son action. Morin affirme même que la communication a plusieurs fonctions : l’information, la connaissance, l’explication et la compréhension. Toutefois, pour lui, le problème central dans la communication humaine est celui de la compréhension, car on communique pour comprendre et se comprendre4. Raison pour laquelle, les chercheurs en matière de communication, surtout de notre ère, époque marquée par l’accroissement des entreprises dans la plupart des secteurs de la vie sociale, se trouvent confronté à de nouvelles problématiques qui sont autant d’enjeux pour améliorer la communication. -

Kalemie L'oubliee Kalemie the Forgotten Mwiba Lodge, Le Safari Version Luxe Mexico Insolite Not a Stranger in a Familiar La
JUILLET-AOUT-SEPTEMBRE 2018 N° 20 TRIMESTRIEL N° 20 5 YEARS ANNIVERSARY 5 ANS DÉJÀ LE VOYAGE EN AFRIQUE TRAVEL in AFRICA LE VOYAGE EN AFRIQUE HAMAJI MAGAZINE N°20 • JUILLET-AOUT-SEPTEMBRE 2018 N°20 • JUILLET-AOUT-SEPTEMBRE HAMAJI MAGAZINE MEXICO INSOLITE Secret Mexico GRAND ANGLE MWIBA LODGE, LE SAFARI VERSION LUXE Mwiba Lodge, luxury safari at its most sumptuous VOYAGE NOT A STRANGER KALEMIE L’OUBLIEE IN A FAMILIAR LAND KALEMIE THE FORGOTTEN Par Sarah Waiswa Sur une plage du Tanganyika, l’ancienne Albertville — On the beach of Tanganyika, the old Albertville 1 | HAMAJI JUILLET N°20AOÛT SEPTEMBRE 2018 EDITOR’S NEWS 6 EDITO 7 CONTRIBUTEURS 8 CONTRIBUTORS OUR WORLD 12 ICONIC SPOT BY THE TRUST MERCHANT BANK OUT OF AFRICA 14 MWIBA LODGE : LE SAFARI DE LUXE À SON SUMMUM LUXURY SAFARI AT ITS MOST SUMPTUOUS ZOOM ECO ÉCONOMIE / ECONOMY TAUX D’INTÉRÊTS / INTEREST RATES AFRICA RDC 24 Taux d’intérêt moyen des prêts — Average loan interest rates, % KALEMIE L'OUBLIÉE — THE FORGOTTEN Taux d’intérêt moyen des dépôts d’épargne — Average interest TANZANIE - 428,8 30 % rates on saving deposits, % TANZANIA AT A GLANCE BALANCE DU COMPTE COURANT EN MILLION US$ 20 % CURRENT ACCOUNT AFRICA 34 A CHAQUE NUMERO HAMAJI MAGAZINE VOUS PROPOSE UN COUP D’OEIL BALANCE, MILLION US$ SUR L’ECONOMIE D’UN PAYS EN AFRIQUE — IN EVERY ISSUE HAMAJI MAGAZINE OFFERS 250 YOU A GLANCE AT AN AFRICAN COUNTRY’S ECONOMY 10 % TRENDY ACCRA, LA CAPITALE DU GHANA 0 SOURCE SOCIAL ECONOMICS OF TANZANIE 2016 -250 -500 0 DENSITÉ DE POPULATION PAR RÉGION / POPULATION DENSITY PER REGION 1996 -
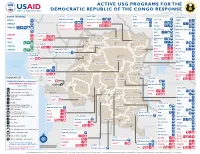
ACTIVE USG PROGRAMS for the DEMOCRATIC REPUBLIC of the CONGO RESPONSE Last Updated 07/27/20
ACTIVE USG PROGRAMS FOR THE DEMOCRATIC REPUBLIC OF THE CONGO RESPONSE Last Updated 07/27/20 BAS-UELE HAUT-UELE ITURI S O U T H S U D A N COUNTRYWIDE NORTH KIVU OCHA IMA World Health Samaritan’s Purse AIRD Internews CARE C.A.R. Samaritan’s Purse Samaritan’s Purse IMA World Health IOM UNHAS CAMEROON DCA ACTED WFP INSO Medair FHI 360 UNICEF Samaritan’s Purse Mercy Corps IMA World Health NRC NORD-UBANGI IMC UNICEF Gbadolite Oxfam ACTED INSO NORD-UBANGI Samaritan’s WFP WFP Gemena BAS-UELE Internews HAUT-UELE Purse ICRC Buta SCF IOM SUD-UBANGI SUD-UBANGI UNHAS MONGALA Isiro Tearfund IRC WFP Lisala ACF Medair UNHCR MONGALA ITURI U Bunia Mercy Corps Mercy Corps IMA World Health G A EQUATEUR Samaritan’s NRC EQUATEUR Kisangani N Purse WFP D WFPaa Oxfam Boende A REPUBLIC OF Mbandaka TSHOPO Samaritan’s ATLANTIC NORTH GABON THE CONGO TSHUAPA Purse TSHOPO KIVU Lake OCEAN Tearfund IMA World Health Goma Victoria Inongo WHH Samaritan’s Purse RWANDA Mercy Corps BURUNDI Samaritan’s Purse MAI-NDOMBE Kindu Bukavu Samaritan’s Purse PROGRAM KEY KINSHASA SOUTH MANIEMA SANKURU MANIEMA KIVU WFP USAID/BHA Non-Food Assistance* WFP ACTED USAID/BHA Food Assistance** SA ! A IMA World Health TA N Z A N I A Kinshasa SH State/PRM KIN KASAÏ Lusambo KWILU Oxfam Kenge TANGANYIKA Agriculture and Food Security KONGO CENTRAL Kananga ACTED CRS Cash Transfers For Food Matadi LOMAMI Kalemie KASAÏ- Kabinda WFP Concern Economic Recovery and Market Tshikapa ORIENTAL Systems KWANGO Mbuji T IMA World Health KWANGO Mayi TANGANYIKA a KASAÏ- n Food Vouchers g WFP a n IMC CENTRAL y i k -

Democratic Republic of Congo Democratic Republic of Congo Gis Unit, Monuc Africa
Map No.SP. 103 ADMINISTRATIVE MAP OF THE DEMOCRATIC REPUBLIC OF CONGO DEMOCRATIC REPUBLIC OF CONGO GIS UNIT, MONUC AFRICA 12°30'0"E 15°0'0"E 17°30'0"E 20°0'0"E 22°30'0"E 25°0'0"E 27°30'0"E 30°0'0"E Central African Republic N N " " 0 0 ' Sudan ' 0 0 ° ° 5 5 Z o n g oBangui Mobayi Bosobolo Gbadolite Yakoma Ango Yaounde Bondo Nord Ubangi Niangara Faradje Cameroon Libenge Bas Uele Dungu Bambesa Businga G e m e n a Haut Uele Poko Rungu Watsa Sud Ubangi Aru Aketi B u tt a II s ii rr o r e Kungu Budjala v N i N " R " 0 0 ' i ' g 0 n 0 3 a 3 ° b Mahagi ° 2 U L ii s a ll a Bumba Wamba 2 Orientale Mongala Co Djugu ng o R i Makanza v Banalia B u n ii a Lake Albert Bongandanga er Irumu Bomongo MambasaIturi B a s a n k u s u Basoko Yahuma Bafwasende Equateur Isangi Djolu Yangambi K i s a n g a n i Bolomba Befale Tshopa K i s a n g a n i Beni Uganda M b a n d a k a N N " Equateur " 0 0 ' ' 0 0 ° Lubero ° 0 Ingende B o e n d e 0 Gabon Ubundu Lake Edward Opala Bikoro Bokungu Lubutu North Kivu Congo Tshuapa Lukolela Ikela Rutshuru Kiri Punia Walikale Masisi Monkoto G o m a Yumbi II n o n g o Kigali Bolobo Lake Kivu Rwanda Lomela Kalehe S S " KabareB u k a v u " 0 0 ' ' 0 Kailo Walungu 0 3 3 ° Shabunda ° 2 2 Mai Ndombe K ii n d u Mushie Mwenga Kwamouth Maniema Pangi B a n d u n d u Bujumbura Oshwe Katako-Kombe South Kivu Uvira Dekese Kole Sankuru Burundi Kas ai R Bagata iver Kibombo Brazzaville Ilebo Fizi Kinshasa Kasongo KasanguluKinshasa Bandundu Bulungu Kasai Oriental Kabambare K e n g e Mweka Lubefu S Luozi L u s a m b o S " Tshela Madimba Kwilu Kasai -

Dr Congo Humanitarian Crisis International Organization for Migration
DR CONGO HUMANITARIAN CRISIS INTERNATIONAL ORGANIZATION FOR MIGRATION SITUATION REPORT 20 April - 16 May 2018 IOM staff monitoring the construction of transitional shelters in Katanika displacement site. Highlights © IOM 2018 (Photo: Carin Atterby) IOM constructed 200 emergency IOM trained 30 staff on the To date, IOM has transferred 3,154 IDPs shelters in Katanika displacement site and Displacement Tracking Matrix in from collective centres in Kalemie to provided in collaboration with the UNHCR preparation for the second baseline study displacement sites, and provided and the RRMP 1,748 IDP households in in seven provinces. voluntary return assistance to 390 IDPs to Kikumbe displacement site with shelter return to their areas of origin. kits. Situation Overview During the reporting period, Ebola Virus Disease was declared on 8 May 2018 in the North-Western province of Equateur in the Democratic Republic of the Congo (DRC). The disease was detected in the village of Bikoro and has since reached urban areas in the city of Mbandaka where the first cases were detected on 11 May 2018. This is the ninth outbreak in this area since the virus was discovered in 1976. The humanitarian community is working alongside the Congolese authorities to mitigate the spreading of the disease. IOM aims to respond by focusing on the surveillance of Point of Entries (POE) to cities and by doing risk communication and promoting sanitary control. IOM in partnership with the World Health Organization (WHO), has already started mapping population mobility (both by using qualitative and quantitative methodologies) through participatory mapping exercises, as well as point surveillance at the selected key POEs including those in Kinshasa. -
From Resource War to ‘Violent Peace’ Transition in the Democratic Republic of the Congo (DRC) from Resource War to ‘Violent Peace’
paper 50 From Resource War to ‘Violent Peace’ Transition in the Democratic Republic of the Congo (DRC) From Resource War to ‘Violent Peace’ Transition in the Democratic Republic of Congo (DRC) by Björn Aust and Willem Jaspers Published by ©BICC, Bonn 2006 Bonn International Center for Conversion Director: Peter J. Croll An der Elisabethkirche 25 D-53113 Bonn Germany Phone: +49-228-911960 Fax: +49-228-241215 E-mail: [email protected] Internet: www.bicc.de Cover Photo: Willem Jaspers From Resource War to ‘Violent Peace’ Table of contents Summary 4 List of Acronyms 6 Introduction 8 War and war economy in the DRC (1998–2002) 10 Post-war economy and transition in the DRC 12 Aim and structure of the paper 14 1. The Congolese peace process 16 1.1 Power shifts and developments leading to the peace agreement 17 Prologue: Africa’s ‘First World War’ and its war economy 18 Power shifts and the spoils of (formal) peace 24 1.2 Political transition: Structural challenges and spoiler problems 29 Humanitarian Situation and International Assistance 30 ‘Spoiler problems’ and political stalemate in the TNG 34 Systemic Corruption and its Impact on Transition 40 1.3 ‘Violent peace’ and security-related liabilities to transition 56 MONUC and its contribution to peace in the DRC 57 Security-related developments in different parts of the DRC since 2002 60 1.4 Fragility of security sector reform 70 Power struggles between institutions and parallel command structures 76 2. A Tale of two cities: Goma and Bukavu as case studies of the transition in North and South Kivu -

Musebe Artisanal Mine, Katanga Democratic Republic of Congo
Gold baseline study one: Musebe artisanal mine, Katanga Democratic Republic of Congo Gregory Mthembu-Salter, Phuzumoya Consulting About the OECD The OECD is a forum in which governments compare and exchange policy experiences, identify good practices in light of emerging challenges, and promote decisions and recommendations to produce better policies for better lives. The OECD’s mission is to promote policies that improve economic and social well-being of people around the world. About the OECD Due Diligence Guidance The OECD Due Diligence Guidance for Responsible Supply Chains of Minerals from Conflict-Affected and High-Risk Areas (OECD Due Diligence Guidance) provides detailed recommendations to help companies respect human rights and avoid contributing to conflict through their mineral purchasing decisions and practices. The OECD Due Diligence Guidance is for use by any company potentially sourcing minerals or metals from conflict-affected and high-risk areas. It is one of the only international frameworks available to help companies meet their due diligence reporting requirements. About this study This gold baseline study is the first of five studies intended to identify and assess potential traceable “conflict-free” supply chains of artisanally-mined Congolese gold and to identify the challenges to implementation of supply chain due diligence. The study was carried out in Musebe, Haut Katanga, Democratic Republic of Congo. This study served as background material for the 7th ICGLR-OECD-UN GoE Forum on Responsible Mineral Supply Chains in Paris on 26-28 May 2014. It was prepared by Gregory Mthembu-Salter of Phuzumoya Consulting, working as a consultant for the OECD Secretariat. -

Democratic Republic of the Congo
DEMOCRATIC REPUBLIC OF THE CONGO MONTHLY REFUGEE STATISTICS Situation as of November 30, 2020 Type Age 0-4 5-11 12-17 18-59 60+ Total % Total Rural (out of camp) 75,821 105,155 62,321 131,723 9,121 384,141 73.3% Total Camps/Sites 23,501 39,046 20,860 47,419 2,981 133,807 25.5% Total 524,302 Total Urban 620 1,487 1,132 2,939 176 6,354 1.2% Grand Total 99,942 145,688 84,313 182,081 12,278 524,302 Refugee Population in DRC Refugee Population by Province in DRC Country Female Male Total % Province Main Location Type Female Male Total Angola** 179 235 414 0.08% Bas Uele Ango & Bondo Rural 22,519 17,697 40,216 Burundi* 25,022 23,530 48,552 9.26% Equateur Disperced Rural 143 213 356 CAR* 91,469 79,582 171,051 32.62% Haut Katanga Lubumbashi & Urb. & Rur. 1,742 Arounds 808 934 Rep.Congo 251 386 637 0.12% Haut Uele Dungu, Doruma Rural 22,311 19,394 41,705 Rwanda*** 107,534 106,440 213,974 40.81% Ituri Aru & Ariwara Rural 25,506 22,351 47,857 S. Sudan* 47,837 41,737 89,574 17.08% Kasai Oriental Tshiala Rural 2 6 8 Kinshasa & Sudan 8 24 32 0.01% Kinshasa Urb. & Rur. 790 outskirts 375 415 Bas Fleuve, Uganda 13 10 23 0.004% Kongo Central Rural 817 MbanzaNg. & Kimaza 328 489 Somalia 7 7 14 0.003% Lomami Luila &MweneDitu Rural 430 456 886 Ivory Coast 4 3 7 0.001% Lualaba Dilolo,Sandoa &Kolwezi Rural 590 596 1,186 Other 10 14 24 0.005% Maniema Pangi, Kailo&Lukolo Rural 203 269 472 Lubero, Masisi, Total 272,334 251,968 524,302 100% Nord Kivu Urb. -

Tender for the Inland Transportation of USAID|Food for Peace Direct Distribution Commodities
Tender for the Inland Transportation of USAID|Food for Peace Direct Distribution Commodities. Location: The Democratic Republic of Congo. Tender №: FH DRC/FY19 Program : Food for the Hungry | Tuendelee Pamoja II. Date: 12th September,2018 Section A: GENERAL CONDITIONS OF TENDER Food for the Hungry (FH) Democratic republic of Congo (DRC) is soliciting for Inland Transporter to transport a minimum of 1,000 (one thousand) and a maximum of 4,460 (Four thousand four hundred and sixty) metric tons of food commodities donated by the United States Government through USAID/Food for Peace from Dar es Salaam, Tanzania to FH warehouses situated in Bukavu, Kalemie and Moba in the Democratic Republic of Congo through Kigoma port on Lake Tanganyika, however shipments destined to Bukavu warehouse will be shipped via Rwanda through Cyangungu/Rusizi customs border post. The commodities to be transported are bagged Cornmeal (packed in 25kg bags), Split Peas (packed in 50kg bags) and bottled (plastic) vegetable oil packaged in cartons. The Inland Transporter company will also be responsible for commodities clearance out of Dar Es Salaam port. All sealed bids, clearly marked “Tender for the Provision of Food Commodities Inland Transport Dar es Salaam – Bukavu, Kalemie and Moba Reference FH DRC/FY19” should be addressed to the Chief of Party, Food for the Hungry, DRC No. 069 Avenue Tanganyika, Quartier de Nyalukemba B.P. 2055, Bukavu, RD Congo. Scanned tender documents can be submitted to [email protected] with subject clearly marked “Tender for the Provision of Food Commodities Inland Transport Dar es Salaam – Bukavu, Kalemie and Moba” not later than Friday 28th September, 2018 before 05:00 pm East African standard time. -

Centre De Recherche Sur L'anti-Corruption
Centre de Recherche sur l’Anti-Corruption Project Title: Citizen Action for open and accountable and inclusive institutions. Project Title: Fix My Street Project Period: 1 year I. Project Description and Justification Short Description of the Project In support of improved public policies and inclusive decision-making, an online tool is created for civic monitoring of Uvira, Bukavu, Goma, Lubumbashi and Kinshasa municipalities activities on solving city problems based on direct reporting from affected citizens. Summary FixmyStreet.cd will help and encourage Congolese to report local problems to the administration of Bukavu, Goma, Lubumbashi and Kinshasa. The problems are located on a map and can be viewed and discussed by citizens, stakeholders and representatives of the competent government authority. The platform, launched through a year-long project, will enable the public to monitor the competent authorities reaction to a reported issue of concern. Goals and objectives The goal of FixmyStreet.cd is to create an online platform that facilitates direct communication on local problems between citizens and the city of Uvira, Bukavu, Goma, Lubumbashi and Kinshasa 's administration. The goal of the platform is to encourage citizens to report issues in their neighborhood they are concerned about by lowering the barriers to get active, share, discuss problems with others, and monitor the authorities’ reactions. Consequently, the project aims to create more public awareness and debate about dangerous problems on the streets of Uvira, Bukavu, Goma, Lubumbashi and Kinshasa. By bringing people's concern about local problems into the public sphere, pressure on the competent authorities to address and solve those issues increases.