EDO IDELTA CDTI PROJEGT {F, ORIGINAL : English
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nigeria's Constitution of 1999
PDF generated: 26 Aug 2021, 16:42 constituteproject.org Nigeria's Constitution of 1999 This complete constitution has been generated from excerpts of texts from the repository of the Comparative Constitutions Project, and distributed on constituteproject.org. constituteproject.org PDF generated: 26 Aug 2021, 16:42 Table of contents Preamble . 5 Chapter I: General Provisions . 5 Part I: Federal Republic of Nigeria . 5 Part II: Powers of the Federal Republic of Nigeria . 6 Chapter II: Fundamental Objectives and Directive Principles of State Policy . 13 Chapter III: Citizenship . 17 Chapter IV: Fundamental Rights . 20 Chapter V: The Legislature . 28 Part I: National Assembly . 28 A. Composition and Staff of National Assembly . 28 B. Procedure for Summoning and Dissolution of National Assembly . 29 C. Qualifications for Membership of National Assembly and Right of Attendance . 32 D. Elections to National Assembly . 35 E. Powers and Control over Public Funds . 36 Part II: House of Assembly of a State . 40 A. Composition and Staff of House of Assembly . 40 B. Procedure for Summoning and Dissolution of House of Assembly . 41 C. Qualification for Membership of House of Assembly and Right of Attendance . 43 D. Elections to a House of Assembly . 45 E. Powers and Control over Public Funds . 47 Chapter VI: The Executive . 50 Part I: Federal Executive . 50 A. The President of the Federation . 50 B. Establishment of Certain Federal Executive Bodies . 58 C. Public Revenue . 61 D. The Public Service of the Federation . 63 Part II: State Executive . 65 A. Governor of a State . 65 B. Establishment of Certain State Executive Bodies . -

ZONAL INTERVENTION PROJECTS Federal Goverment of Nigeria APPROPRIATION ACT
2014 APPROPRIATION ACT ZONAL INTERVENTION PROJECTS Federal Goverment of Nigeria APPROPRIATION ACT Federal Government of Nigeria 2014 APPROPRIATION ACT S/NO PROJECT TITLE AMOUNT AGENCY =N= 1 CONSTRUCTION OF ZING-YAKOKO-MONKIN ROAD, TARABA STATE 300,000,000 WORKS 2 CONSTRUCTION OF AJELE ROAD, ESAN SOUTH EAST LGA, EDO CENTRAL SENATORIAL 80,000,000 WORKS DISTRICT, EDO STATE 3 YOUTH DEVELOPMENT CENTRE, OTADA, OTUKPO, BENUE STATE (ONGOING) 150,000,000 YOUTH 4 YOUTH DEVELOPMENT CENTRE, OBI, BENUE STATE (ONGOING) 110,000,000 YOUTH 5 YOUTH DEVELOPMENT CENTRE, AGATU, BENUE STATE (ONGOING) 110,000,000 YOUTH 6 YOUTH DEVELOPMENT CENTRE-MPU,ANINRI LGA ENUGU STATE 70,000,000 YOUTH 7 YOUTH DEVELOPMENT CENTRE-AWGU, ENUGU STATE 150,000,000 YOUTH 8 YOUTH DEVELOPMENT CENTRE-ACHI,OJI RIVER ENUGU STATE 70,000,000 YOUTH 9 YOUTH DEVELOPMENT CENTRE-NGWO UDI LGA ENUGU STATE 100,000,000 YOUTH 10 YOUTH DEVELOPMENT CENTRE- IWOLLO, EZEAGU LGA, ENUGU STATE 100,000,000 YOUTH 11 YOUTH EMPOWERMENT PROGRAMME IN LAGOS WEST SENATORIAL DISTRICT, LAGOS STATE 250,000,000 YOUTH 12 COMPLETION OF YOUTH DEVELOPMENT CENTRE AT BADAGRY LGA, LAGOS 200,000,000 YOUTH 13 YOUTH DEVELOPMENT CENTRE IN IKOM, CROSS RIVER CENTRAL SENATORIAL DISTRICT, CROSS 34,000,000 YOUTH RIVER STATE (ON-GOING) 14 ELECTRIFICATION OF ALIFETI-OBA-IGA OLOGBECHE IN APA LGA, BENUE 25,000,000 REA 15 ELECTRIFICATION OF OJAGBAMA ADOKA, OTUKPO LGA, BENUE (NEW) 25,000,000 REA 16 POWER IMPROVEMENT AND PROCUREMENT AND INSTALLATION OF TRANSFORMERS IN 280,000,000 POWER OTUKPO LGA (NEW) 17 ELECTRIFICATION OF ZING—YAKOKO—MONKIN (ON-GOING) 100,000,000 POWER ADD100M 18 SUPPLY OF 10 NOS. -

States and Lcdas Codes.Cdr
PFA CODES 28 UKANEFUN KPK AK 6 CHIBOK CBK BO 8 ETSAKO-EAST AGD ED 20 ONUIMO KWE IM 32 RIMIN-GADO RMG KN KWARA 9 IJEBU-NORTH JGB OG 30 OYO-EAST YYY OY YOBE 1 Stanbic IBTC Pension Managers Limited 0021 29 URU OFFONG ORUKO UFG AK 7 DAMBOA DAM BO 9 ETSAKO-WEST AUC ED 21 ORLU RLU IM 33 ROGO RGG KN S/N LGA NAME LGA STATE 10 IJEBU-NORTH-EAST JNE OG 31 SAKI-EAST GMD OY S/N LGA NAME LGA STATE 2 Premium Pension Limited 0022 30 URUAN DUU AK 8 DIKWA DKW BO 10 IGUEBEN GUE ED 22 ORSU AWT IM 34 SHANONO SNN KN CODE CODE 11 IJEBU-ODE JBD OG 32 SAKI-WEST SHK OY CODE CODE 3 Leadway Pensure PFA Limited 0023 31 UYO UYY AK 9 GUBIO GUB BO 11 IKPOBA-OKHA DGE ED 23 ORU-EAST MMA IM 35 SUMAILA SML KN 1 ASA AFN KW 12 IKENNE KNN OG 33 SURULERE RSD OY 1 BADE GSH YB 4 Sigma Pensions Limited 0024 10 GUZAMALA GZM BO 12 OREDO BEN ED 24 ORU-WEST NGB IM 36 TAKAI TAK KN 2 BARUTEN KSB KW 13 IMEKO-AFON MEK OG 2 BOSARI DPH YB 5 Pensions Alliance Limited 0025 ANAMBRA 11 GWOZA GZA BO 13 ORHIONMWON ABD ED 25 OWERRI-MUNICIPAL WER IM 37 TARAUNI TRN KN 3 EDU LAF KW 14 IPOKIA PKA OG PLATEAU 3 DAMATURU DTR YB 6 ARM Pension Managers Limited 0026 S/N LGA NAME LGA STATE 12 HAWUL HWL BO 14 OVIA-NORTH-EAST AKA ED 26 26 OWERRI-NORTH RRT IM 38 TOFA TEA KN 4 EKITI ARP KW 15 OBAFEMI OWODE WDE OG S/N LGA NAME LGA STATE 4 FIKA FKA YB 7 Trustfund Pensions Plc 0028 CODE CODE 13 JERE JRE BO 15 OVIA-SOUTH-WEST GBZ ED 27 27 OWERRI-WEST UMG IM 39 TSANYAWA TYW KN 5 IFELODUN SHA KW 16 ODEDAH DED OG CODE CODE 5 FUNE FUN YB 8 First Guarantee Pension Limited 0029 1 AGUATA AGU AN 14 KAGA KGG BO 16 OWAN-EAST -
Assessment of the Use of Surface Water and Its Environmental Health Effects in Ekpoma, Nigeria
International Journal of Development and Sustainability ISSN: 2186-8662 – www.isdsnet.com/ijds Volume 6 Number 12 (2017): Pages 2147-2161 ISDS Article ID: IJDS17111002 Assessment of the use of surface water and its environmental health effects in Ekpoma, Nigeria Okhakhu Poly Alens * Department of Geography and Environmental Management, Ambrose Alli University, Ekpoma, Nigeria Abstract This study which benefits from field data and hydro-climatic literature examines the use of surface water and its environmental health effects in Ekpoma, Nigeria. It identifies rainfall, borehole, public tap and rivers as the main surface water resources which are used by the residents for domestic, agricultural, institutional, industrial, and research activities in Ekpoma. It observes that owing to poor road surfaces, failed power sources, obsolete water purification facilities, little maintenance funds, absence of specialists, increased fuel price, poor surveillance of facilities, inadequate security and existence of pervious catchment basins, the residents do not have adequate access to clean and purified surface water resources for daily uses. These limitations led to occurrence of water-induced diseases as cholera, diarrhea, dysentery, gastroenteritis, malaria, ringworm, trachoma and typhoid fever in Ekpoma. Based on these findings, the study suggests among others that adequately clean and purified surface water resources managed by specialists, reinforced with modern facilities and sufficiently funded by the state government should be supplied to the residents to eliminate these rampant diseases in the settlement. Keywords: Surface Water; Use; Environment; Health Effects; Ekpoma-Nigeria Published by ISDS LLC, Japan | Copyright © 2017 by the Author(s) | This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. -

Organized Crime Facts Edo State
ORGANIZED CRIME FACTS • EDO STATE GEOPOLITICAL INTELLIGENCE CRIME INTELLIGENCE MARITIME INTELLIGENCE SPECIAL INVESTIGATION BREAKING NEWS INCIDENT ALERT SYSTEM Location: Lagos, Nigeria [email protected] +2349083588787 Being inundated with fears over the rising spate Gifting the delegation as we sat to deliberate on of insecurity in the nation, I always find solace the reason for our visit from their variety of in working from the comfort of my office's natural resources, we could not help but blot bounded walls. Therefore my dismay came to a out:what went wrong that the nation's crescendo when my organization nominated heartbeat has transformed into the nightmare me as part of a high profiled delegation to of travellers and residents alike? investigate the accelerated spate of the insecurity situation in Edo State. Recall that #ENDSARS protest hijacked by hoodlums resulted in a prison break within the Benin City is the state capital and largest urban state. Anticipation became rife that hoodlums centre, tilting more than 1,800feet in the north wreak of terror in Edo state would abate with while lying at elevations between 500 feet in time. However, the magnitude and intensity the south. Edo state bounded by Kogi to the took a turn for the worse. The gravity has northeast and east, Anambra to the degenerated to an equilibrium where Edo state east, Delta to the southeast and south, sends jitters. and Ondo to the west and northwest; is famous for its unique bronze, brass and ivory works of Kidnapping, armed robbery and cultism have arts which are found all over the world in recently reached its peak within and around the museums. -

Conflict Incident Monthly Tracker
Conflict Incident Monthly Tracker Edo State: February - M arch 2 01 8 B a ck gro und The incident led to heightened tensions in Arson: In February, a man reportedly set the area. ablaze the house he inherited from his father This monthly tracker is designed to update over payment of rent in Oredo LGA. Over 20 Peace Agents on patterns and trends in Violence Affecting Women and Girls shops were destroyed. The man resisted conflict risk and violence, as identified by the (VAWG): In January, two brothers attempts by neighbors to stop the fire, Integrated Peace and Development Unit reportedly killed their grandmother for claiming it is better for him to burn down the (IPDU) early warning system, and to seek ritualistic purposes in Ikpoba-Okha LGA. house than to allow tenants stay for free. feedback and input for response to mitigate Separately, a retired female military officer areas of conflict. was reportedly killed and set ablaze in her Recent Incidents or house by her security guard in Benin City, Patterns and Trends the state capital. Also, in January, a Issues, March 2018 herdsman reportedly inflicted a fatal injury D ec 2 01 7 -Fe b 20 1 8 Incidents reported during the month mainly on a woman at her farm in Akoko-Edo LGA. According to Peace Map data (see Figure 1), related to communal tensions, and reported incidents during this period Violent Protest: In February, four people criminality. including a policeman were reported dead included criminality, communal tensions, Communal Tensions: Residents of Odighi during a protest over the dead of a 26-year protests, and violence affecting women and and Odiguetue communities in Oredo LGA old commercial driver in Benin City, Oredo girls. -

Original Research
DOI: http://dx.doi.org/10.4314/star.v3i3.4 ISSN: 2226-7522(Print) and 2305-3372 (Online) Science, Technology and Arts Research Journal Sci. Technol. Arts Res. J., July-Sep 2014, 3(3): 23-28 Journal Homepage: http://www.starjournal.org/ Original Research Ethnobotany and Germplasm Collection of Two Genera of Cocoyam (Colocasia [Schott] and Xanthosoma [Schott], Araceae) in Edo State Nigeria Osawaru M.E1, 2 and Ogwu, M.C1* 1Department of Plant Biology and Biotechnology, Faculty of Life Sciences, University of Benin, Benin City, Nigeria 2Department of Biological Sciences, University of Abuja, Gwagwalada, Abuja FCT, Nigeria Abstract Article Information Ethnobotany describes the realm between human interactions with plant in their Article History: environment. Colocasia [Schott] and Xanthosoma [Schott] (Araceae) are important staples Received : 29-05-2014 in Nigeria. This study aims to document the traditional knowledge base of these crops Revised : 10-09-2014 amongst tribes in Edo state. Using random stratified sampling technique, fifty respondents Accepted : 17-09-2014 were selected and primary data obtained through semi structured questionnaire. Fifty-four Keywords: cocoyam (61.11 % Xanthosomaand and 38.89 % Colocasia) germplasm were collected Ethnobotany and documented. Respondents were mostly between 41-50 years (29.63 %) while farming Colocasia and Xanthosoma (33.33 %) is the dominant occupation. The dominant ethnic groups encountered were Bini Plant Germplasm Traditional Knowledge (22.22 %) and Esan (25.93 %). Status of cocoyam collected was 94.44 % and 5.55 % for Plant Genetic Resources cultivated and wild respectively. Local names were significant with over twenty recorded. Edo state Food use (94.26 %) is higher than non-food use (5.74 %). -
Etsako: an Anthropological Reflection of an Endangered Minority Language in Nigeria
Etsako: An Anthropological Reflection of an Endangered Minority Language in Nigeria by M. D. Enaikele [email protected] Federal College of Fisheries and Marine Technology Victoria Island, Lagos, Nigeria Abstract Language is an important means of interaction. As people interact with their indigenous language, their culture, unique experiences and identity are shared and transmitted from one generation to the next. On the other hand, a language could go into extinction when its speakers cease to pass it from one generation to the next. An ethnographic study was conducted to evaluate the epistemological process underlying the threat to Etsako minority language, suggest solutions to safeguarding the language extinction and above all, provide ethno-historical information of the people. The findings show that Etsako is seriously under threat of extinction or simply endangered because the mother tongue is no longer being acquired by children whose parents are from this language community. The study recommends that the challenges of redeeming and revitalising Etsako language should be collective responsibility of Etsako people, their traditional rulers, scholars from Etsako and the government. Especially also, as the home remains the major and important agent of socialization, it is the contention of this paper that parents and other members of the language community of Etsako have a key role to play in intergenerational language transmission. One of the ways they can achieve this is by speaking the mother tongue to the children. Key Words: endangered, minority, language, Etsako Introduction Language is perhaps the most distinctive behaviour that makes human being human. It is among the very first form of behaviour that we learn as children. -

Original Researc Original Research
DOI: http://dx.doi.org/10.4314/star.v4i1.5 ISSN: 2226-7522(Print) and 2305 -3372 (Online) Science, Technology and Arts Research Journal Sci. Technol. Arts Res. J., Jan-March 2015, 4(1): 34-44 Journal Homepage: http://www.starjournal.org/ Original Research Soil Characteristics, Microbial Compostion of Plot, Leaf Count and Sprout Studies of Cocoyam (Colocasia [Schott] and Xanthosoma [Schott], Araceae) Collected in Edo State, Southern Nigeria Ogwu, M.C*and Osawaru, M.E Department of Plant Biology and Biotechnology, Facult y of Life Sciences, University o f Benin, Benin City, Nigeria Abstract Article Information Cocoyam ( Colocasia [Schott] and Xanthosoma [Schott]) belongs to the family Araceae and Article History: Alismatales order. The aim of this study is to collect cocoyam from the eighteen Local Received : 25-11-2014 Government Areas (LGA) in Edo state and describe them based on leaf count and sprout percentage. Using random stratified sam pling methods, cocoyam were collected. Field trials Revised : 15-02-2015 were conducted in the Experimental Garden, Department of Plant Biology and Biotechnology. Accepted : 02-03-2015 The soil was subjected to analysis at the Soil Science Department, University of Benin to determine its characteri stics and suitability for the growth of these arable crops.. The soil Keywords : microbial count was 6.25 X 10 5 and 1.34 X 10 5 cfu/g for bacterial and fungi respectively. Leaves Phosphorus, potassium, manganese and copper were low, zinc and iron were moderate Sprout studies whereas solubl e salts were high in the soil. Results of percentage sprout indicate accessions from Esan south east had highest percentage sprout of 92.0 % while accessions from Owan Vegetable East had the lowest percentage sprout value of 33.3 %. -
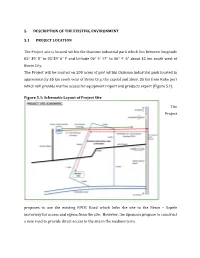
5 5 . DESCRIPTION of the EXISTING ENVIRONMENT .1 PROJECT LOCATION the Project Site Is Located Within the Ossiomo Indus
5. DESCRIPTION OF THE EXISTING ENVIRONMENT 5.1 PROJECT LOCATION The Project site is located within the Ossiomo industrial park which lies between longitude 05° 39' 8" to 05°39' 6" E and latitude 06° 4' 17" to 06° 4' 6" about 35 km south west of Benin City. The Project will be located on 200 acres of plot within Ossiomo industrial park located in approximately 35 km south west of Benin City, the capital and about 35 km from Koko port which will provide marine access for equipment import and products export (Figure 5.1). Figure 5.1: Schematic Layout of Project Site The Project proposes to use the existing NPDC Road which links the site to the Benin – Sapele motorway for access and egress from the site. However, the Sponsors propose to construct a new road to provide direct access to the site in the medium term. Plate 5.1 Benin – Sapele Motorway (March 2010) Plate 5.2 Marine Access to Project Site (Google) Plate 5.3 Ossiomo River Access to Project Site (March 2010) Plate 5.4 Ossiomo River Access to Project Site (March 2010) 5.2 BASELINE DATA The information source is based on a combination of literature review, field studies, and laboratory analyses. The literature review encompassed background information on the climatic condition of the area including recent environmental studies. Literature was sourced from the Project Sponsor, the Nigerian Meteorological Agency, the Federal and State Ministries of Environment, State Ministry of Lands and Agriculture. Additional data sources includes published articles in journals, gazettes, and technical reports, maps, internet, etc. -
Conflict Incident Monthly Tracker
Conflict Incident Monthly Tracker Edo State: March - A pr il 20 1 8 B a ck gro und watching over some herdsmen arrested for two sons in Benin City, Oredo LGA. alleged armed robbery in Ikpoba-Okha LGA. This monthly tracker is designed to update Drug Trafficking: In March, a 64-year old The incident led to heightened tensions in Peace Agents on patterns and trends in man was reportedly arrested by operatives the area. In March, residents of Odighi and conflict risk and violence, as identified by the of the National Drug Law Enforcement Odiguetue communities in Oredo LGA Integrated Peace and Development Unit Agency (NDLEA) over illicit drug trafficking in protested at the palace of the Oba of Benin (IPDU) early warning system, and to seek Egor LGA. About 280 bags of Indian hemp over frequent attacks by herdsmen in the feedback and input for response to mitigate were recovered from the suspect. area. areas of conflict. Violence Affecting Women and Girls Recent Incidents or Patterns and Trends (VAWG): In January, two brothers Issues, April 2018 J anuar y -M arch 2 0 1 8 reportedly killed their grandmother for ritualistic purposes in Ikpoba-Okha LGA. Incidents reported during the month mainly According to Peace Map data (see Figure 1), Separately, a retired female military officer related to criminality, sexual violence, and there was rise in lethal violence in Edo state was reportedly killed and set ablaze in her protests. in March 2018. Reported incidents during house by her security guard in Benin City, Criminality: Thugs reportedly attacked a this period included criminality, communal the state capital. -

Strategic Concepts for Skill Refinement and Development Amongst Educationally Less Privileged: a Focus on Etsako Community of Edo State, Nigeria
STRATEGIC CONCEPTS FOR SKILL REFINEMENT AND DEVELOPMENT AMONGST EDUCATIONALLY LESS PRIVILEGED: A FOCUS ON ETSAKO COMMUNITY OF EDO STATE, NIGERIA By *Omoregie, Kester O., *Oduntan, E.B, *Obuda V. & **Bada, O. *Computer Science Department,Auchi Polytechnic, Auchi **Statistics Department, Auchi Polytechnic, Auchi [email protected], [email protected], [email protected] &[email protected] Abstract Bringing education to the nomadic, road transport workers, street artisans, farmers in rural areas, and fishermen in coastal areas whose lifestyle have been so much conditioned by their social and cultural backgrounds has been one major challenge in Nigeria Education sector. For example, it is some cultural belief in Nigeria that men should marry many wives with the sole aim of having many male children that can be useful in farm works.This research paper reveals some ICT innovative concepts for reaching out to some categories of educationally less privileged in our society, keeping in mind the social and cultural background. The focus here is on bike riders, motor mechanics, and farmers in the rural areas of Etsako community of Edo state in Nigeria.The aim is to break through the socio-cultural barriers and bring education to the people in such a way as to enhance their productivity with a refinement on the existing skills, and development of new skills. Keywords: Skill refinement, Skill development, Socio-cultural barriers, ICT, Productivity. INTRODUCTION Bringing education to the educationally less privileged is a challenge that we must address in our society. A number of factors which include family background, tradition and culture of society have made formal education difficult to be realized among certain individuals.