PS Form 1769 Worksheet Fascimile, September 1991 (P
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Post Office Llv Shop Manual 2019
Post Office Llv Shop Manual 2019 If you are looking for the ebook Post office llv shop manual 2019 in pdf form, then you have come on to the loyal website. We present full option of this ebook in DjVu, PDF, ePub, doc, txt formats. You can read online Post office llv shop manual 2019 either download. Additionally, on our website you can reading the guides and another art eBooks online, or load theirs. We want to invite regard what our website does not store the book itself, but we give reference to the site wherever you may downloading either read online. If have must to downloading pdf Post office llv shop manual 2019, then you've come to the correct website. We own Post office llv shop manual 2019 doc, DjVu, PDF, ePub, txt forms. We will be glad if you return us again and again. online chevrolet llv service & repair manual - - Online Repair Manual Home > Chevrolet > LLV Online Chevrolet LLV Repair Manual Software This online repair manual software is easy to use and you are covered by grumman llv - wikipedia, the free encyclopedia - The Grumman Long Life Vehicle, also known as the LLV, is an American light transport truck. The Grumman LLV was designed for the United States Postal Service, which usps s latest solution for aging long - postal - LONG LIFE VEHICLE (LLV) There shall be a fully detailed service manual provided in some family member of the post office management that made this post office - At the Post Office our aim is to provide you with the things that are important to you Whether you pop into a branch or shop online, 1989 -
1999 GES Coding and Editing Manual 1999
U.S. Department of Transportation National Highway Traffic Safety Administration General Estimates System Coding And Editing Manual 1999 Table of Contents Variables/Questions are displayed in data entry order. Variable/Question Name Index .......................................... vi PAR A22 Police Jurisdiction ................................................1 A01 Date ...........................................................2 A02 Time ...........................................................3 A23 Stratum .........................................................5 PAR Configuration Questions A03 Number of Motor Vehicles ..........................................8 A04 Number of Non-Motorists ..........................................11 Events E01 Event Number -- NEW VARIABLE ...................................13 V01 Vehicle Number (This Vehicle) ......................................19 V24 Initial Point of Impact (This Vehicle) ..................................20 E02 Action -- NEW VARIABLE .........................................24 A06 First Harmful Event ..............................................27 V01 Vehicle Number (Other Vehicle) ....................................39 V24 Initial Point of Impact (Other Vehicle) .................................40 A07 Manner of Collision ..............................................44 Crash Data Questions A05 Land Use ......................................................47 A25 Work Zone .....................................................48 A21 School Bus Related ..............................................49 -

I!1'C[F&!) POSTAL RATE Commlsston WASHINGTON, DC
BEFORE THE i!1‘C[f&!) POSTAL RATE COMMlSStON ‘(3 Ii WASHINGTON, DC. 20266~661 5 2J, p/j 90, pw:,I fi,\iE c”, OFFICEOF r//C s;hkk,>,,,, POSTAL RATE AND FEE CHANGES,2001 i Docket No. R2001-1 RESPONSE OF UNITED STATES POSTAL SERVICE WITNESS TAYMAN TO INTERROGATORIES OF THE OFFICE OF THE CONSUMER ADVOCATE (OCA/USPS-T&l-21) The United States Postal Service hereby provides the responses of witness Tayman to the following interrogatories of the Office of the Consumer Advocate: OCA/USPS-T6-l-21, filed on October 3,200l. Each interrogatory is stated verbatim and is followed by the response. Respectfully submitted, UNITED STATES POSTAL SERVICE By its attorneys: Daniel J. Foucheaux, Jr. Chief Counsel, Ratemaking 475 L’Enfant Plaza West, S.W. Washington, D.C. 20260-l 137 (202) 266-2999; Fax -5402 October 17,200l RESPONSE OF UNITED STATES POSTAL SERVICE WITNESS TAYMAN TO INTERROGATORIES OF THE OFFICE OF THE CONSUMER ADVOCATE OCA/USPS-16-l. The following refer to the USPS FY 2001 and FY 2002 Operating Plans. (a) Please provide the FY 2001 Operating Plan and the most current USPS FY 2002 Operating Plan by accounting periods for Postal Service operating revenues, appropriations, investment income, expenses and volumes. 04 For each of the thirteen accounting periods presented in part “a” of this interrogatory, please provide the most current USPS Operating Plan with operating revenues broken out by mail class and subclass cost categories. RESPONSE: (a) The FY 2001 Operating Plan by accounting period is attached. The FY 2002 accounting period Operating Plan has not been finalized. -
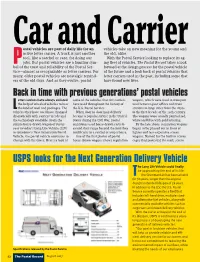
USPS Looks for the Next Generation Delivery Vehicle He Long Life Vehicle Could Finally Be Approaching the End of Its Life
Carostal vehicles are partand of daily life for an vehiclesCarrier take on new meaning for the young and active letter carrier. A truck is just another the old, alike. tool, like a satchel or case, for doing our With the Postal Service looking to replace its ag- Pjobs. But postal vehicles are a familiar sym- ing fleet of vehicles, The Postal Record takes a look bol of the trust and reliability of the Postal Ser- forward at the design process for the postal vehicle vice—almost as recognizable as letter carriers. For of the future and a look back at postal vehicles that many, older postal vehicles are nostalgic remind- letter carriers used in the past, including some that ers of the old days. And as they evolve, postal have found new lives. Back in time with previous generations’ postal vehicles etter carriers have always enlisted some of the vehicles that city carriers wagons, which were used to transport the help of wheeled vehicles to bear have used throughout the history of mail between post offices and train Lthe load of mail and packages. The the U.S. Postal Service. stations in large cities from the 1870s vehicles they have used have changed When door-to-door mail delivery to the first decade of the 20th century. dramatically with carriers’ needs and became a popular service in the United The wagons were usually painted red, the technology available. From the States during the Civil War, postal white and blue with gold lettering. simple horse-drawn wagon of yester- employees used horse-drawn carts to By the late 1890s, regulation wagons year to today’s Long Life Vehicle (LLV) extend their range beyond the mail they began to be phased out in favor of to tomorrow’s Next Generation Postal could carry in a satchel or atop a horse. -

BUSINESS MAILERS REVIEW Monitoring the Postal Service, Private Carriers and Suppliers Published by PNMSI Publishing Co
BUSINESS MAILERS REVIEW Monitoring the Postal Service, Private Carriers and Suppliers Published by PNMSI Publishing Co. Volume 38, Number 21 October 23, 2017 USPS Seeks 2018 Price Increase USPS filed a case earlier this month with the As in the past, the Postal Service will not include Postal Regulatory Commission (PRC) for a proposed any surcharges for fuel, residential delivery, or regular price adjustment for all classes of mail. This price Saturday delivery. adjustment, if approved by the PRC, will be effective on Jan. 21, 2018. Non-Competitive Products Price adjustments for Non-Competitive Products as an overall percentage basis by mail class average about 1.9%. Individual price categories within each class of mail listed below will have varying percentage increases, some greater than the overall percentage increase. In fact, some price categories will actually see a decrease in pricing. The new prices, if approved, include a one cent increase in the price of a First-Class Mail Forever stamp from 49 cents to 50 cents. Postcard stamps and metered letters would also have a one cent increase. The USPS filing does not include any price change for single-piece letters being mailed to international destinations or for additional ounces for letters. Competitive Products In contrast, prices for Competitive Products and services will increase by about 4%. The USPS requested an overall 3.9% increase for Priority Mail Express. Retail prices will increase an average of 3.9%, while Commer- cial Base prices increase an average of 3.7% and Com- While Mailing Services price increases are mercial Plus by 3.7%. -
2014 FARS/NASS GES Coding and Validation Manual
DOT HS 812 216 Revised July 2016 2014 FARS/NASS GES Coding and Validation Manual 2014 FARS / NASS GES MANUAL CHANGES SUMMARY Below is a list of elements that have substantial changes for 2014. These changes, as well as others, are highlighted throughout the manual by bold/italic type. IT IS RECOMMENDED THAT YOU REVIEW THE ENTIRE MANUAL FOR ALL CHANGES NEW/ NEW/ ELEMENT # ELEMENT REVISED REVISED COMMENTS NAME VALUES REMARKS Submission X . Update Remarks for (103) Data Sources Instructions for hierarchy. C17 Crash Events X X . Added Remarks from Sequence of - Sequence of Events. Events . Updated Remarks and Attribute for: "70 - Non-harmful, Swaying Trailer/Jackknife [non-harmful]". Updated Remarks for Attributes: "33 - Curb", "43 - Other Fixed Object" and "68 - Cross Centerline". Added new Attribute and Remarks: "79 - Ran Off Roadway - Direction Unknown". Added new Remarks for: "Guidelines for PAR Combination Attributes". Updated Remarks for: "Collision with Fixed Object". C17 Crash Events . Added Remarks from Areas of Impact. - Areas of . Updated Remarks regarding "Load". Impact C18 First Harmful X . Updated Remarks for Attributes for: "33 - Event Curb" and "43 - Other Fixed Object". Added new Remarks for: "Guidelines for PAR Combination Attributes". Updated Remarks for: "Collision with Fixed Object". C20 Relation to X `X . Updated Remarks and Attribute for: "16 - Junction (a/b) Shared-Use Path or Trail Crossing". C22 Relation to X Updated Remarks for Attribute: "04 - On Trafficway Roadside" NEW/ NEW/ ELEMENT # ELEMENT REVISED REVISED COMMENTS NAME VALUES REMARKS C31 Related X . Added new examples for Attribute: "14 - Factors - Motor Vehicle Struck by Falling Cargo, or Crash Level Something That Came Loose From, Or Something That was Set-in-Motion by a Vehicle". -
Congressional Record United States Th of America PROCEEDINGS and DEBATES of the 117 CONGRESS, FIRST SESSION
E PL UR UM IB N U U S Congressional Record United States th of America PROCEEDINGS AND DEBATES OF THE 117 CONGRESS, FIRST SESSION Vol. 167 WASHINGTON, WEDNESDAY, MARCH 3, 2021 No. 40 House of Representatives The House met at 9 a.m. and was In the strength of Your divine name local officials and volunteers across called to order by the Speaker pro tem- we pray. the country—its limitations were laid pore (Mr. CUELLAR). Amen. bare, for us to fix. f f H.R. 1 would shore up our democracy and the people’s faith in its power. DESIGNATION OF THE SPEAKER THE JOURNAL I am pleased this bill incorporates PRO TEMPORE The SPEAKER pro tempore. Pursu- two of my bills. The first requires all The SPEAKER pro tempore laid be- ant to section 5(a)(1)(A) of House Reso- States to offer same-day registration. fore the House the following commu- lution 8, the Journal of the last day’s The second ends partisan gerry- nication from the Speaker: proceedings is approved. mandering by requiring States to adopt WASHINGTON, DC, f citizen redistricting commissions. March 3, 2021. I urge my colleagues to join me in I hereby appoint the Honorable HENRY PLEDGE OF ALLEGIANCE voting ‘‘yes’’ for this transformational CUELLAR to act as Speaker pro tempore on this day. The SPEAKER pro tempore. Will the bill that fights special interests, takes NANCY PELOSI, gentleman from Florida (Mr. GIMENEZ) money out of politics, and puts power Speaker of the House of Representatives. come forward and lead the House in the back in the hands of the American peo- f Pledge of Allegiance. -

Recyclers News Pres November December 2015
Iowa Auto Recyclers November / December 2015 Inside this issue: Mike Swift Becomes President Mike Swift 10 ARA President of the Automotive Recyclers Association from front cover Professional Automotive Recycler Mike Association’s initiatives and directives. Swift of Swift's Trails End Auto Recy- Sue Speaking 8 "I am honored to take the reigns as Pres- cling, in Des Moines, Iowa, gave his in- augural speech as the President of the ident of ARA and to continue to play a Automotive Recyclers Association (ARA) role in preserving and promoting the Haz Comm 11 at the 72nd Annual ARA Convention & work of professional automotive recy- New Labels Exposition held October 7-10 in Char- clers,” said Swift in his acceptance lotte, North Carolina. speech. Swift, a longstanding ARA and Scholarship 15 Certified Automotive Recycler (CAR) Program His tenure on the Executive Committee member, is extremely active in the indus- of the Association, where he has served try as a cutting-edge automotive recycler as Secretary, Second Vice President, and leader in his community. Next Gen 16 and First Vice President, continues in a Delivery leading role to help shape and guide the Continued on page 10... Postal Trucks Industry News 20 ARA Update 22 Photo courtesy of ARA Recyclers News Press Page 3 Page 3 Recyclers IAR’s 2014-2016 Board of Directors News Press Andy Wilken, President nd Wilken Auto Salvage Tom Quandt (2014 – 2 Term) Phone: 641-435-4077 Quandt Auto Salvage, Inc. [email protected] Phone: 712-792-9204 The RECYCLERS NEWS PRESS is [email protected] published six times per year for the Brad Osborn, rd Iowa Automotive Recyclers. -

NEWS ARCHIVES JULY 2017 National News
NEWS ARCHIVES JULY 2017 National News July 31 WashingtonTimes: When the U.S. Postal Service’s top marketing officer agreed to hire Goldman Sachs nearly two years ago without a written contract, top executives inside postal headquarters scrambled to make the unauthorized deal square with postal procurement rules. But the no-bid contract they eventually awarded to Goldman Sachs was backdated and was for the wrong kinds of services: The company was hired under a banking services agreement, but Goldman Sachs‘ postal work didn’t have anything to do with banking, records show. In trying to fix a $1.5 million deal that already generated misgivings, officials may have only added to the list of problems that remain under review by the Postal Service’s office of inspector general even after the contract’s expiration. Key details about the arrangement have surfaced through the inspector general’s recently released report on the tenure of the Postal Service’s former president of shipping and mailing services, Robert Bernstock. TeamBHP: Mahindra has bagged a $11 million prototype contract from the US Govt. for next-gen postal delivery vehicles. Mahindra Automotive North America will deliver 14 prototypes for approval by November, 2017. According to media reports, the prototypes will be built in Detroit and will be delivered for road-testing in two phases. The first batch of eight prototypes will be delivered in September and the remaining six by November. If approved, Mahindra will have to build 1.8 lakh vehicles over a six year period. The price of each vehicle is expected to be around $35,000 and also a maintenance and repair contract will be awarded. -
Bargaining Agreement Ollowing Balloting, Eligible NALC Back Pay Will Be Calculated from the in Step O on Nov
Volume 134/Number 5 May 2021 In this issue President’s Message 1 National Officers 35 Branch Election Notices 55 Branch Items 56 The monthly journal of the NATIONAL ASSOCIATION OF LETTER CARRIERS G THE NEW IN VE- I G IN IMPLEMENT IN COLLECT —PAGES 12-19 BARGA AGREEMENT InstallInstall thethe freefree NALCNALC MemberMember AppApp forfor youryour iPhoneiPhone oror AndroidAndroid smartphonesmartphone As technology increases our ability to communicate, NALC must stay ahead of the curve. We’ve now taken the next step with the NALC Member App for iPhone and Android smartphones. The app was de- veloped with the needs of letter carriers in mind. The app’s features include: • Workplace resources, including the National • Instantaneous NALC news with Agreement, JCAM, MRS and CCA resources personalized push notifications • Interactive Non-Scheduled Days calendar and social media access • Legislative tools, including bill tracker, • Much more individualized congressional representatives and PAC information GoGo to to the the App App Store Store oror GoogleGoogle Play Play and and search search forfor “NALC “NALC Member Member App”App” toto install install for for free free President’s Message American workers need the PRO Act lthough the NALC was sions of a Union Buster: “Union busting is a field populated by founded in 1889, it bullies and built on deceit. A campaign against a union is an was not legally recog- assault on individuals and a war against the truth. As such, it nized as the exclusive is a war without honor. The only way to bust a union is to lie, representative of city distort, manipulate, threaten, and always, always attack. -

The Next Generation Delivery Vehicle Congressional Reps Want
Next The Generation Delivery Vehicle Congressional reps want investigation n late February, the Postal Service President Biden described in January startup that specializes in electric awarded the contract for the Next his administration’s plan for purchas- vehicles, announced that it would chal- IGeneration Delivery Vehicle (NGDV) ing federal vehicles, as follows: “The lenge the award, and three members of to Oshkosh Defense of Wisconsin. The federal government also owns an Congress called for a freeze on the con- winning design provides the Postal enormous fleet of vehicles, which we’re tract. Ohio Reps. Marcy Kaptur and Tim Service with the option of ordering going to replace with clean electric Ryan, along with Rep. Jared Huffman of either electric or fossil fuel engines. vehicles….” California, put forward a resolution that USPS says that at least 10 percent of When the USPS contract was calls for Congress to investigate how the new vehicles will come with electric awarded, one of the losing vendors, the Oshkosh contract was awarded. It motors. Workhorse Group Inc., an Ohio-based calls for the award to be in line with the 22 The Postal Record May 2021 May 2021 fter five years of proto- the 34 companies that responded to types and testing, on Feb. the RFI, USPS narrowed the field to a 23, the Postal Service an- 15 prospective vendors. After meeting nounced that it had awarded a contract with these vendors, the Postal Service to build the Next Generation Delivery issued a request for proposal (RFP), Vehicle (NGDV) to Oshkosh Defense. inviting each company to submit Under the terms of the contract, Osh- ideas for building a prototype vehicle kosh Defense will finalize the produc- for testing. -

General Estimates System (GES)
U.S. DEPARTMENT OF TRANSPORTATION National Highway Traffic Safety Administration National Automotive Sampling System (NASS) General Estimates System (GES) Analytical User's Manual 1988-1999 NASS GES Analytical User’s Manual 1988 - 1999 U. S. Department of Transportation National Highway Traffic Safety Administration National Center for Statistics and Analysis Washington, D.C. 20590 TABLE OF CONTENTS Introduction ...................................................................1 GES Operations ................................................................2 GES Sample Design .............................................................3 GES SAS Files ................................................................5 Understanding the GES Imputation Process ...........................................7 National Estimates ..............................................................9 GES Variable List .............................................................10 GES Variables and Definitions: ....................................................15 Accident File ...........................................................16 Vehicle/Driver File .......................................................36 Person File .............................................................70 Appendices: A. Make/Model Designation ............................................83 B. V23 Accident Type Diagram ........................................116 C. Summary Statistics ...............................................117 D. Generalized Estimated Sampling Errors