Travel Insurance Claim Form | Cruise Mapfre Insurance Services
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Investigations Unveil Extent of Fraud
ESSENTIAL READING FOR TRAVEL INSURANCE INDUSTRY PROFESSIONALS WWW.ITIJ.CO.UK NOVEMBER 2011 • ISSUE 130 Investigations unveil extent of fraud Kenyan conundrum The summer holiday season has come to an end in the northern hemisphere, and with it has come more dire warnings from travel insurance Travel insurers basing their coverage decisions on companies that fraud is on the up – both from travel advice from government agencies have hit clinics treating travellers, and from travellers the headlines in the UK recently. Mandy Aitchison themselves. Sarah Watson reports on the problem looks into the issue In a recent editorial piece in Insurance Insight, The UK’s Foreign and Commonwealth Offi ce (FCO) Mike Keating of AXA Insurance explained that has advised against ‘all but essential travel to coastal the company noticed ‘a worrying trend over the areas within 150 km of the Kenya-Somalia border’. It summer’, stating that AXA’s claims department further explained: “We advise against all but essential received some excessively high medical bills as part travel to coastal areas within 150 km of the Somali of claims for treatment in Spain, Turkey, Bulgaria, border, following two attacks by armed gangs in small Egypt and sub-Saharan Africa. He added: “There boats against beach resorts in the Lamu area on 11 is evidence of overcharging, overdiagnosis and September and 1 October 2011. This advice will be over-treatment of minor problems and collusion kept under review. Both attacks were on beach-front between clinics and holidaymakers. Travellers need properties, with two Westerners kidnapped and one to be warned of the risks involved in using overseas murdered. -

Admiralty, Maritime & Naval
30 ANTIQUARIAN TITLES ON ADMIRALTY, MARITIME & NAVAL LAW May 10, 2016 The Lawbook Exchange, Ltd. (800) 422-6686 or (732) 382-1800 | Fax: (732) 382-1887 [email protected] | www.lawbookexchange.com 30 Antiquarian Titles on Admiralty, Maritime and Naval Law Scarce Eighteenth-Century Treatise on Prize Law and Privateering 1. Abreu y Bertodano, Felix Joseph de [c.1700-1775]. Traite Juridico-Politique sur les Prises Maritimes, et Sur les Moyens qui Doivent Concourir pour Rendre ces Prises Legitimes. Paris: Chez la Veuve Delaguette, 1758. Two volumes in one, each with title page and individual pagination. Octavo (6-1/2" x 4"). Contemporary speckled sheep, raised bands, lettering piece and gilt ornaments to spine, speckled edges, patterned endpapers. Some wear to corners, joints starting, some worming to lettering piece, joints and hinges. Attractive woodcut head-pieces. Toning to sections of text, light foxing to a few leaves, internally clean. An appealing copy of a scarce title. $1,500. * Second French edition. First published in Madrid in 1746, this treatise on prize law and privateering went through three other editions, all in France in a translation by the author, in 1753, 1758 and 1802. Little is known about Abreu, a minor Spanish noble and diplomat. According to the title page, he was a "membre de l'Academie Espagnole, & actuellement Envoye Extraordinaire de S.M. Catholique aupres du Roi de la Grande-Bretagne." All editions are scarce. OCLC locates 5 copies of all editions in the Americas, 1 of this edition (at Columbia University Law Library). Not in the British Museum Catalogue. -

Closing the Protection Gap, Disaster Risk Financing: Smart Solutions For
Closing the protection gap Disaster risk financing: Smart solutions for the public sector Every year natural and man-made catastrophes cause a distressing loss of lives and considerable economic costs around the world. Both industrialised and developing countries are affected. Surprisingly, both are also materially underinsured. This financing gap is borne largely by the public sector, and may create long-term fiscal instability at a time when government budgets are stretched. Furthermore rating agencies are starting to take a closer look at such contingent liabilities faced by public administrations. But there are ways to alleviate both the impacts and the costs of disaster by planning ahead. Insurance plays a critical role in effective disaster risk management helping communities get back on their feet faster. This report outlines tools and approaches proven to help governments, regions and cities, as well as the constituents they represent, to become more resilient. We’re smarter together Cover images Above: Cars getting stuck on flooded streets in Fukuyama, 23 June 2016, after areas of western Japan were hit by heavy rain, causing landslides and caving in roads. Below: Emergency workers supporting the recovery after an earthquake on 25 August 2016 in Amatrice, Italy Table of contents Disaster risks are growing 2 A major strain on government budgets 4 Resilience through insurance 6 More than one way to close 12 the protection gap Benefits of sovereign and 18 sub-sovereign risk transfer Case studies 21 A single house left standing after Hurricane Ike struck Gilchrist, Texas in 2008. Disaster risks are growing The economic cost of natural catastrophes has increased markedly. -

COMMERCIAL INSURANCE PACKAGE (Applicable to Entertainment Related Risks Only)
COMMERCIAL INSURANCE PACKAGE (Applicable to entertainment related risks only) 1. Full Legal Name of company(ies) to be Insured: 2. Business Address: 3. Contact Name: Fax: Web-site: Phone: Cell: Email: Please provide CV on background experience of the principals of the company along with a company bio if you have not previously obtained coverage through our office. 4. Describe your operations: 5. Date company established: 6. Number of full time employees: 7. Do you have employee health/ benefits plan? Yes No 8. Previous Insurer: Expiry Date: Have there been any losses in the last 5 years? Yes No If yes, how many and please provide details: 9. Has any form of insurance been declined or cancelled? Yes No 10. General Information: explain all “yes” responses below (a) Is equipment loaned or rented to others with/without operators Yes No (b) If you responded yes above, do they provide certificates of insurance Yes No (c) Is post production work done for others Yes No (d) Does applicant travel out of country with equipment Yes No (e) Are any repairs and/or installations done away from the premises Yes No (f) Are sub-contractors used Yes No (g) If yes, is proof of insurance obtained Yes No Explain in detail all “yes” answers in section 10: August ‘-09 Front Row Insurance Brokers Inc. T 604-684-FILM (3456) Toll Free: 1-866-690-3456 COMMERCIAL PACKAGE 604 – 1200 Burrard Street F 604-684-3437 Vancouver BC V6Z 2C7 Initial 1 PROPERTY INFORMATION . 11. Location Address: owned: rented: square Feet: no. of stories: CONSTRUCTION Fire Resistive masonry -
WEATHER INDEX INSURANCE for AGRICULTURE: Guidance for Development Practitioners
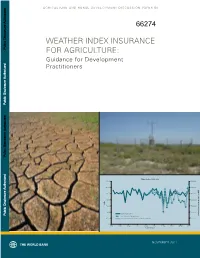
AGRICULTURE AND RURAL DEVELOPMENT DISCUSSION PAPER 50 WEATHER INDEX INSURANCE Public Disclosure Authorized FOR AGRICULTURE: Guidance for Development Practitioners Public Disclosure Authorized Public Disclosure Authorized Maize Index, 1962−2007 140.00 3500000 120.00 3000000 100.00 2500000 80.00 2000000 oduction (MT) e pr alue v 60.00 1500000 otal maiz 40.00 1000000 Maize Index, MMI national t Public Disclosure Authorized Met Office 75-Station Model 20.00 National Total Maize Production (Normalized AP) 500000 0.00 0 1962 1967 1972 1977 1982 1987 1992 1997 2002 2007 harvest year NOVEMBER 2011 A&R_Risk_Cover.indd 2 29/10/11 1:02 PM AGRICULTURE AND RURAL DEVELOPMENT DISCUSSION PAPER 50 WEATHER INDEX INSURANCE FOR AGRICULTURE: Guidance for Development Practitioners A&R_Risk_FM.indd 1 28/10/11 11:59 AM © 2011 The International Bank for Reconstruction and Development / The World Bank 1818 H Street, NW Washington, DC 20433 Telephone: 202-473-1000 Internet: http://www.worldbank.org/rural All rights reserved. The findings, interpretations, and conclusions expressed herein are those of the author(s) and do not necessarily reflect the views of the Board of Executive Directors of the World Bank or the governments they represent. The World Bank does not guarantee the accuracy of the data included in this work. The boundaries, colors, denominations, and other information shown on any map in this work do not imply any judgment on the part of the World Bank concerning the legal status of any territory or the endorsement or acceptance of such boundaries. Rights and Permissions The material in this work is copyrighted. -

A Comparative History of Insurance Law in Europe. a Research Agenda
Comparative Studies in the History of Insurance Law Studien zur vergleichenden Geschichte des Versicherungsrechts Volume / Band 1 A Comparative History of Insurance Law in Europe A Research Agenda Edited by Phillip Hellwege Duncker & Humblot · Berlin PHILLIP HELLWEGE (ED.) A Comparative History of Insurance Law in Europe Comparative Studies in the History of Insurance Law Studien zur vergleichenden Geschichte des Versicherungsrechts Edited by / Herausgegeben von Prof. Dr. Phillip Hellwege Volume / Band 1 A Comparative History of Insurance Law in Europe A Research Agenda Edited by Phillip Hellwege Duncker & Humblot · Berlin The project ‘A Comparative History of Insurance Law in Europe’ has received funding from the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation programme (grant agreement No. 647019). Bibliographic information of the German national library The German national library registers this publication in the German national bibliography; specified bibliographic data are retrievable on the Internet about http://dnb.d-nb.de. All rights reserved. No part of this book may be reproduced, translated, or utilized in any form or by any means, electronic or mechanical, without the expressed written consent of the publisher. © 2018 Duncker & Humblot GmbH, Berlin Printing: CPI buchbücher.de GmbH, Birkach Printed in Germany ISSN 2625-638X (Print) / ISSN 2625-6398 (Online) ISBN 978-3-428-15499-9 (Print) ISBN 978-3-428-55499-7 (E-Book) ISBN 978-3-428-85499-8 (Print & E-Book) Printed on no aging resistant (non-acid) paper according to ISO 9706 Internet: http://www.duncker-humblot.de Preface The history of insurance law has fallen into neglect, and the state of research is for a number of reasons unsatisfactory. -

Weather Insurance for Farmers: Experience from Ethiopia Nahu Senaye Araya
Weather Insurance for Farmers: Experience from Ethiopia Nahu Senaye Araya Session 5 Breakout Session 11 Weather Insurance for Farmers: Experience from Ethiopia1 Nahu Senaye Araya2 Paper presented at the IFAD Conference on New Directions for Smallholder Agriculture 24-25 January, 2011 International Fund for Agricultural Development Via Paolo Di Dono, 44, Rome 00142, Italy 1 Copyright of the paper is reserved by IFAD. The paper may not be reproduced in part or in full and in any form without written permission of the Conference Organisers at IFAD (e-mail: [email protected]) 2 The author is Chief Executive Officer of Nyala Insurance, Addis Ababa, Ethiopia Summary Agriculture is the dominant sector in the Ethiopian economy where 83% of the population fully depends on and more than 43% of the GDP is generated. This sector in turn is dominated by a subsistence farming where more than 95% is a rain fed farming of which more than 90% owned by a smallholder (mostly less than half hectar) poor farmers. These smallholder farmers are highly exposed to the negative impact of climate change mainly reflected in shortage of rainfall (draught) in this part of the continent. The climate risk mitigation mechanisms existing in the country are more of informal traditional ways of risk sharing and risk smoothing mechanism. Whereas the covariant nature of the climate risk like draught cannot be copped with this traditional mechanisms. Therefore as an innovative means of market mechanism Nyala Insurance S.C. (NISCO) has introduced insurance products which can help in mitigating the impact of climate risk. -

Principles of Insurance Law Peter N
University of Richmond UR Scholarship Repository Law Faculty Publications School of Law 2011 Principles of Insurance Law Peter N. Swisher University of Richmond, [email protected] Follow this and additional works at: http://scholarship.richmond.edu/law-faculty-publications Part of the Insurance Law Commons Recommended Citation Jeffrey W. Stempel et al., Principles of Insurance Law (4th ed., 2011). This Book is brought to you for free and open access by the School of Law at UR Scholarship Repository. It has been accepted for inclusion in Law Faculty Publications by an authorized administrator of UR Scholarship Repository. For more information, please contact [email protected]. PRINCIPLES OF INSURANCE LAW FOURTH EDITION JEFFREY W. STEMPEL Doris S. & Theodore B. Lee Professor of Law William S. Boyd School of Law University of Nevada, Las Vegas PETER N. SWISHER Professor of Law T.C. Williams School of Law University of Richmond ERIK S. KNUTSEN Associate Professor Queen's University Faculty of Law Kingston, Ontario, Canada • . LexisNexis· Preface There have been a number of important developments in liability insurance, property insurance, and life and health insurance that have significantly impacted insurance law. Accordingly, our Fourth Edition of Principles of Insurance Law has been substantially revised and updated in order to offer the insurance law student and practitioner a broad perspective of both traditional insurance law concepts and cutting-edge legal issues affecting contemporary insurance law theory and practice. We have retained .the organization substantially begun in the Third Edition, with fifteen chapters, a division that enables an expanded scope of topical coverage and also segments the law of insurance in a manner more amenable to study, as well as facilitating recombination and reordering of the chapters as desired by individual instructors. -

Taxation of Insurance Companies
Taxation of Insurance Companies Informational Paper 10 Wisconsin Legislative Fiscal Bureau January, 2017 Taxation of Insurance Companies Prepared by Sean Moran Wisconsin Legislative Fiscal Bureau One East Main, Suite 301 Madison, WI 53703 http://legis.wisconsin.gov/lfb Taxation of Insurance Companies This paper provides background information example, under a pure "term" life insurance on the taxation of insurance companies in policy, the insured pays a premium which Wisconsin. While the main topic is the separate obligates the insurance company to pay a specific state premiums tax imposed on certain insurance sum in the event of the insured's death during the companies, the imposition of the state corporate term of the policy. Term insurance is the most income/franchise tax is also discussed. straightforward type of life insurance policy in that the premium provides coverage only in the In order to put the taxation of insurance com- event of death during the policy's specified term. panies in focus, information is provided on the characteristics of the insurance industry and the Certain life insurance policies perform a bank- Wisconsin operations of some of the major com- like function in that policyholder premiums are panies in different lines of insurance. The regula- invested by the insurer on behalf of the insured. tory role of the Office of the Commissioner of Income from such investments is credited to the Insurance (OCI) is also discussed briefly. Finally, policyholder's account in determining the policy's a discussion of the rationale and issues of insur- "cash surrender value," which is the amount which ance taxation is presented and the insurance tax the insured would receive if he or she cancels the provisions of other states are outlined. -

Division of Insurance 2008 Annual Report 1
Commonwealth of Massachusetts Division of Insurance 2008 Annual Report Nonnie S. Burnes Commissioner of Insurance www.mass.gov\doi Table of Contents 1. Division of Insurance .......................................................................................................1 Mission ................................................................................................................................................ 1 Primary Activities ................................................................................................................................. 1 Organizational Chart ........................................................................................................................... 3 Human Resources ............................................................................................................................... 3 Budget, Revenue & Assessments ....................................................................................................... 4 The Massachusetts Insurance Marketplace ........................................................................................ 7 2. Significant Events of 2008 ............................................................................................. 10 Automobile Insurance Reform ........................................................................................................... 10 Global Financial Crisis ....................................................................................................................... 13 3. -

Travel Insurance Important Policy Information
Insurance Travel Insurance Important policy information 24-hour medical assistance & to access cashless medical expenses +44 (0)203 362 2451 Non-medical emergency claims www.travel.co-opinsurance.co.uk/login or call +44 (0)203 362 2450 Other policy queries +44 (0)203 362 2452 coop.co.uk/travelinsurance Co-op covers BKP 0320.indd 1 28/04/2020 10:12:27 COOP/MF/PW/BKP/0321 This policy document will outline everything you need to know about your cover. Have a read and make sure you’re completely happy. If you have any questions or concerns, please don’t hesitate to call us on 0330 400 1626. Useful contact details Optional upgrades For medical screening To further enable you to tailor your policy to Either complete the online medical your specific travel requirements, we have screening step as part of the online designed the following great range of purchase of your policy; or optional upgrades. Call 0330 400 1626 • Winter sports cover See pages 3 and 4 for more information • Gadget and valuables upgrade • Natural disaster cover For emergency medical assistance • Car hire excess waiver Call +44 (0)207 748 0060 • Hazardous activities cover See pages 4 and 11 – 12 for more For full details of these cover options, information please see pages 29 – 34. To make a claim To submit your claim online, go to: www.travel.co-opinsurance.co.uk/login To start, just log in through ‘Manage your quote or policy’ or ‘Make a claim’. If your query relates to an existing claim, please call us on +44 (0)203 362 2450. -

Insuring Farmers Against Weather Shocks: Evidence from India, As Partial Fulfilment of the Requirements of Grant OW3.1171 Awarded Under Open Window 3
Jeremy Tobacman Insuring farmers against Daniel Stein weather shocks Vivek Shah Laura Litvine Evidence from India Shawn Cole Raghabendra Chattopadhyay July 2017 Impact Agriculture Evaluation Report 29 About 3ie The International Initiative for Impact Evaluation (3ie) is an international grant-making NGO promoting evidence-informed development policies and programmes. We are the global leader in funding, producing and synthesising high-quality evidence of what works, for whom, how, why and at what cost. We believe that better and policy-relevant evidence will help make development more effective and improve people’s lives. 3ie impact evaluations 3ie-supported impact evaluations assess the difference a development intervention has made to social and economic outcomes. 3ie is committed to funding rigorous evaluations that include a theory-based design, use the most appropriate mix of methods to capture outcomes and are useful in complex development contexts. About this report 3ie accepted the final version of this report, Insuring farmers against weather shocks: evidence from India, as partial fulfilment of the requirements of grant OW3.1171 awarded under Open Window 3. The report has been formatted to 3ie standards. However, despite best efforts in working with the authors, some references are still missing and figures and tables could not be improved. We have copy-edited the content to the extent possible. These efforts caused a delay in publishing this report, which is why the series number and date are out of sequence. All of the content is the sole responsibility of the authors and does not represent the opinions of 3ie, its donors or its board of commissioners.