Utilization of Institutional Delivery Service and Associated Factors
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Report on Field Trip to Provide Technical Support in Emergency Preparedness and Response
World Health Organisation (WHO) Emergency Humanitarian Action (EHA) Ethiopia Programme Report on field trip to provide technical support in emergency preparedness and response to Oromiya Regional State Ethiopia 13th March 2007 – 23rd March 2007 Report prepared by: Amey Kouwonou, MD, MSc (Epidemiology), Field Officer EHA/WHO Ethiopia March 2007 Report on field trip to Oromiya Regional State, Ethiopia, March 2007 / AMEY 1 Table of content Executive summary ------------------------------------------------------------------------- 3 List of acronyms ---------------------------------------------------------------------------- 4 I/ Background ------------------------------------------------------------------------------- 5 II/ Objective of the mission ----------------------------------------------------------------- 6 III/ Methodology ---------------------------------------------------------------------------- 6 IV/ Findings --------------------------------------------------------------------------------- 6 A/ Situation ---------------------------------------------------------------------------------- 6 At regional level ------------------------------------------------------------------------- 6 Bale Zone ------------------------------------------------------------------------------- 7 Borena zone ----------------------------------------------------------------------------- 9 Guji Zone -------------------------------------------------------------------------------- 9 B / Interventions ---------------------------------------------------------------------------- -

Addis Ababa Science and Technology University College of Architecture and Civil Engineering Department of Civil Engineering
ADDIS ABABA SCIENCE AND TECHNOLOGY UNIVERSITY COLLEGE OF ARCHITECTURE AND CIVIL ENGINEERING DEPARTMENT OF CIVIL ENGINEERING Master thesis on: Hydraulic Analysis of Road Drainage Structures and Proposed Mitigation Measures (Case study of Bule hora to Yirgacheffe Asphalt Road). By Mitiku Chachu Advisor Fitsum Tesfaye (PhD) Thesis submitted to school of graduate studies, Addis Ababa Science and Technology University, for the in partial fulfillment of the requirement for the Degree of Masters of Science in Civil engineering (Hydraulic Engineering Major) June, 2018 APPROVAL PAGE This MSc thesis entitled with “Hydraulic Analysis of Road Drainage Structures and Proposed Mitigation Measures (case study BuleHorato Yirgacheffe Asphalt Road).” has been approved by the following examiners in partial fulfillment of the requirement for the degree of Master of Science in Hydraulic Engineering. Date of Defense: June 9, 2018 Principal Advisor 1. Dr. Fitsum Tesfaye _______ ______ Signature Date Members of the Examining board: 1. Dr. Mohamed _______ ________ External Examiner Signature Date 2. Dr. Adanech Yared ________ _______ Internal Examiner Signature Date 3. Dr. Melaku Sisay ___________ ___________ ERA PG ,Programme Coordinator Signature Date 4. Mr. Simon G/egiziabher _______ ________ Head , Civil Eng’g Department Signature Date 5. Dr. Brook Abate _______ ________ Dean, College of Architecture Signature Date and Civil Engineering i CERTIFICATION I, the undersigned, certify that I read and hear by recommend for acceptance by Addis Ababa Science and Technology University a dissertation entitled “Hydraulic Analysis of Road Drainage Structures and Proposed Mitigation Measures ( Case Study of BuleHorato Yirgacheffe Asphalt Road).” in partial fulfillment of the requirement for the degree of Master of Civil Engineering in Hydraulic Engineering major. -

ETHIOPIA Humanitarian Situation Report
1) ETHIOPIA Humanitarian Situation Report Child screening for malnutrition in Gewane health centre in Afar ©UNICEF Ethiopia/2015/Tesfaye SitRep #7 – Reporting Period, November-December 2015 SITUATION IN NUMBERS Highlights: 10.2 million people, including Ethiopia is facing its worst drought in decades, with over 10.2 million 6 million children, will require relief people requiring food aid in 2016. An estimated 435,000 children are food assistance in 2016. in need of treatment for severe acute malnutrition (SAM), and more than 1.7 million children, pregnant and lactating women with 435,000 children will require treatment moderate acute malnutrition (MAM) will require supplementary for acute severe malnutrition in 2016. feeding. As of October 2015, UNICEF has supported the treatment of 291,214 under-five children suffering severe acute malnutrition 730,358 total refugees in Ethiopia (SAM) with a cure rate of 88 per cent. (UNHCR, November 2015). Over 4.9 million children under-five were vaccinated against measles during a national vaccination campaign in October-November 2015. UNICEF procured 5,894,100 doses of measles vaccine to support the campaign. UNICEF will require US$106 million UNICEF, Health, WASH and C4D jointly responded to an acute for its humanitarian work in 2016. watery diarrhoea outbreak in Moyale woreda of Oromia and Somali regions. The number of reported cases has drastically decreased and the spread of the outbreak contained. Since first of January 2016, no new cases have been reported. UNICEF’s Key Response with Partners -

Value Chain Analysis of Milk and Milk Products in Borana Pastoralist Area
VALUE CHAIN ANALYSIS OF MILK AND MILK PRODUCTS IN BORANA PASTORALIST AREA COMMISSIONED BY: CARE-ETHIOPIA Regional Resilience Enhancement against Drought Project BY YONAD BUSINESS PROMOTION AND CONSULTANCY PLC Address: P.O.BOX 18054, Telephone 011-3714731, Mobile 091-1507881, Fax 011-1550323 E-mail: [email protected] Addis Ababa, Ethiopia Contents Page No Excutive Summary..................................................................................................................................6 Acknowledgements...............................................................................................................................10 Acronyms..............................................................................................................................................11 1. Introduction.....................................................................................................................................12 1.1 Overview ....................................................................................................................................12 1.2. Background of the study............................................................................................................12 1.3. Description of Borana Pastoral Area .........................................................................................12 1.4. Objectives of the study ..............................................................................................................14 1.5. Methodology of the study..........................................................................................................14 -

RESPONSE OVERVIEW Ethiopia | 04 June 2020
COVID-19 RESPONSE OVERVIEW Ethiopia | 04 June 2020 1. Partnerships and Coordination • As the designated lead agency for supporting the Government of Ethiopia (GoE) in the management of migrant returnees, IOM continued to support GoE in coordinating support for quarantine facilities in Addis Ababa and the regions (54 in total). Supporting the • Following simulation exercises in two quarantine facilities, IOM is planning similar exercises Government of in other quarantine facilities to prepare for upcoming returnees. Ethiopia 2. Disease Surveillance • Between 1 April and 4 June, Ethiopia received over 14,800 returnees: 4,440 from Sudan, 3,700 from Djibouti, approx. 3,000 from the Kingdom of Saudi Arabia (KSA), 2,350 from Somalia, 640 from Lebanon and 560 from Kenya. • IOM, UNICEF, and the Red Cross supported the GoE in receiving 647 returnees from Lebanon and 270 from KSA at the Addis Ababa airport over the past week. • IOM registered 2,408 migrant returnees in quarantine facilities: 647 Lebanese returnees 2,408 Returnees (646 Female and 1 Male) in Addis Ababa, 144 returnees in Semera, 682 (449 male, 233 registered in female) in Jijiga, 82 in Moyale (59 male, 23 female), 583 in Metema (553 male, 30 female) quarantine over the past week. facilities • Provided direct assistance to over 6,600 migrant returnees in quarantine including: transportation from Points of Entry (POEs) to quarantine facilities, registration, Non- food items (NFIs), Food, personal protective equipment (PPEs), subsistence allowance for onward transportation, family tracing and reunification, and Mental Health and Psychosocial Support (MHPSS) since April 1. 6,600 Returnees • Deployed two laboratory staff and supported the set-up of the COVID-19 laboratory in received Addis Ababa Science and Technology University (AASTU) quarantine facility. -
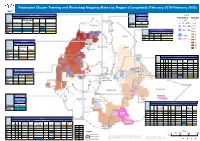
Protection Cluster Training and Workshop Mapping Matrix by Region (Completed) (February 2019-February 2020)
Protection Cluster Training and Workshop Mapping Matrix by Region (Completed) (February 2019-February 2020) Addis Ababa Tigray Legend Organizing Agency(ies) Organizing Population Hotspot UN Women/ Agency ! < 50 1 Cluster UN Women UNHCR UNFPA UNHCR UNHCR/IOM Cluster IRC ! 51 - 150 2 GBV Tigray GBV ! 151 - 300 3 GP 4 PSEA Mekele HaHraarriari 301 - 500 ! ! 5 SMS OrOgragnaizninizgi nAgg eAngceyn(iceys()ies) 6 Cluster IMC PAPDA UNHCR/IOM > 500 Afar GBV ! 7 Targeted woredas Gonder SMS 8 Amhara City Adm. 9 Organizing Agency(ies) 10 OHCHR/ Amhara Semera ! 11 Bahir Dar Cluster AAH EARO UNICEF ! CP Beneshangul Somali GBV Organizing AgeSnomcya(liies) HR Gumuz Organizing Agency(ies) OHCHR/ PSEA UNHCR/ Cluster AAH HI IRC NRC EARO Network UNHCR IOM UNICEF Assosa ! CP GBV Dire Dawa ! GP Benishangul Gumuz Harar Jijiga HLP ! ! Harari HR Organizing Agency(ies) Addis Ababa Nekemte Town ! Babile PSEA Addis Ababa Kebribayah Cluster AAH IRC UNICEF City SMS Bishoftu Town CP Adama Town Gambella ! GBV Lagahida Gambela Oromia Somali Hawassa Selahad Hawas!a Town Gambela Kudunbur Lehel-Yucub Organizing SNNPR Dila City Admin Agency SSNNNNPP Kochere Organizing Agency(ies) Cluster UN Women Gedeb UNFPA/ PSEA Bule Hora Town OHCHR/ UNICEF/ UNHCR/ Cluster EMA NRC EARO PAPDA PI UNFPA UNHCR UNHCR IOM UNICEF CP Deka Filtu suftu GBV GP Oromia HLP Organizing Agency(ies) HR Dolo Odo OHCHR/ UN Women/ UNHCR/ USC/ PSEA Cluster AAH IRC NRC EARO PAPDA UNHCR UNFPAUNHCR OHCHR UNICEF CP AoR SMS CP CP Moyale GBV GBV (Oromia) GP GP Legend Kms HLP 0 50 100 200 300 HLP ! Region Capitals HR The boundaries and names shown, and the designations used on this ´ HR PSEA Region boundary map do not imply official endorsement or acceptance by the United Create Date: 02 March-2020 Nations. -
Student Perception on Group Work and Group Assignments In
Vol. 12(17), pp. 860-866, 10 September, 2017 DOI: 10.5897/ERR2016.3006 Article Number: 2C89E2965822 ISSN 1990-3839 Educational Research and Reviews Copyright © 2017 Author(s) retain the copyright of this article http://www.academicjournals.org/ERR Full Length Research Paper Student perception on group work and group assignments in classroom teaching: The case of Bule Hora university second year biology students, South Ethiopia: An action research Tolessa Muleta Daba1*, Sorale Jilo Ejersa2 and Sultan Aliyi2 1Social Anthropology Department, Bule Hora University, Bule Hora, Ethiopia. 2 English Language and Literature Department, Bule Hora University, Bule Hora, Ethiopia. Received 16 September, 2016; Accepted 6 October, 2016 Group learning has become a common practice in schools and tertiary institutions. It provides more comfortable and supportive learning environment than solitary work. It fosters critical thinking skills, develops individual accountability, increases levels of reasoning and positive interdependence, improves problem-solving strategies and internalizes content knowledge. But many factors influence the group relation, such as members’ perceptions, attitudes and willingness to cooperate and contribute as a team. Therefore, this study was conducted on students’ perceptions and attitudes towards the usefulness of group work mainly, and how the students evaluate factors that may affect their participation specifically. This cross-sectional study was conducted in Bule Hora University from February to June, 2015. Quantitative research approaches had been applied; using semi-structured face-to-face interviews and focus group discussion with Biology students and Instructors. Of the total number of 47 students who participated in the study, 25 (53%) of the students’ responded that they prefer group work than other types of assessment while few of them 4 (8.51%) replied that they disagree with group work use. -

ETHIOPIA IDP Situation Report May 2019
ETHIOPIA IDP Situation Report May 2019 Highlights • Government return operations continue at full scale and sites are being dismantled. • Where security is assured and rehabilitation support provided, IDPs have opted to return to their areas of origin. IDPs who still feel insecure and have experienced trauma prefer to relocate elsewhere or integrate within the community. Management of IDP preferences differs in every IDP caseload. • There is minimal to no assistance in areas of return. Local authorities have requested international partner sup- port to address the gap. Meanwhile, public-private initiatives continue to fundraise for the rehabilitation of IDPs. • The living condition of the already vulnerable host communities has deteriorated having shared their limited resources with the IDPs for over a year. I. Displacement context Government IDP return operations have been implemented at full scale since early May 2019 following the 8 April 2019 announcement of the Federal Government’s Strategic Plan to Address Internal Displacement and a costed Re- covery/Rehabilitation Plan. By end May, most IDP sites/camps were dismantled, in particular in East/West Wollega and Gedeo/West Guji zones. Humanitarian partners have increased their engagement with Government at all levels aiming to improve the implementation of the Government return operation, in particular advocating for the returns to happen voluntarily, in safety, sustainably and with dignity. Overall, humanitarian needs remain high in both areas of displacement and of return. Most assistance in displace- ment areas is disrupted following the mass Government return operation and the dismantling of sites, while assis- tance in areas of return remain scant to non-existent, affecting the sustainability of the returns. -

Pbs Iii Audited Entities That Received Management Letter Identifying Internal Control Weaknesses with the Recommendation
Annex I PBS III AUDITED ENTITIES THAT RECEIVED MANAGEMENT LETTER IDENTIFYING INTERNAL CONTROL WEAKNESSES WITH THE RECOMMENDATION DURING THE 2008/9 AUDIT PERIOD Ser no Audited Entity I PBS III 2008 EFY 3RD QUARTER 1 AMHARA REGIONAL STATE . 1. MOTA TOWN ADMINISTRATION 2. GONCHA SISO ENESIE WOREDA 3. GUBALAFTO WOREDA 4. ENEBSIE SAR MIDER WOREDA 5. HAGERE MARIAM WOREDA 6. KALU WOREDA 7. HULET EJU ENESSE WOREDA 2. OROMIA REGIONAL STATE 1. Arsi Negele Woreda 2. Ambo Town Administration 3. Bekoji Town administration 4. Limu Bilbilo Woreda 5. Ade’a Woreda 6. Digalu na Tijo Woreda 7. Munesa Woreda 8. Tiyo Woreda 9. Bedelle Woreda 10. Bedelle Town Administration 11. Beddesa Woreda 12. Gechi Woreda 3. BENISHANGUL-GUMUZ REGIONAL STATE 1. Banbis Woreda 4. SOUTHERN N/N/P/ REGIONAL STATE 1. Arbegona Woreda 2. Aroresa Woreda 3. Bona Zuria Woreda 4. Chire Woreda 5. Gedeb Woreda 6. Gorche Woreda 7. Bitta woreda. 8. Masha town administration. 9. Masha woreda. 10. Yem special woreda. 11. lomma woreda. 12. mareka wored. 5. HARARI PEOPLE NATIONAL REGIONAL STATE 1. Education Bureau 2. Agriculture Development Bureau 3. Health Bureau 4. Rural Road Authority 6. DIRE DAWA TOWN ADMINISTRATION 1. Education Bureau II PBS III 2008 EFY 4TH QUARTER 1 TIGRAY REGIONSL STATE 1. WATER RESOURCE BUREAU 2. ADIGRAT TOWN ADMINISTRATION 3. HEALTH BUREAU 2 AMHARA NATIONAL REGIONAL STATE 1. WORELUEWOREDA 2. DENBIA WOREDA 3. GONJ KOLLELA WOREDA 4. TAKUSSAWOREDA 5. GUAGUSA SHEKUDAD WOREDA 6. ADIARKIY WOREDA 7. KUTABER WOREDA 8. WOLDIA TOWN ADMINISTRATION 9. AMBASEL WOREDA 10. ANDABET WOREDA/former name was WEST ESTIE WOREDA/ 11. -

Report on COVID-19 Emergency Responses (April-May 2020)
Reaching and Serving the most Vulnerable! Action for the Needy in Ethiopia (ANE) Headquarters (HQ) Report on COVID-19 Emergency Responses (April-May 2020) May 2020 Introduction In light of the ongoing integrated interventions led by Ethiopian Government to combat the rapid proliferation of COVID-19, Action for the Needy in Ethiopia (ANE) has continued its commitment on social responsibilities, by allocating large portion of budget of more than ETB 1,000,000 from its own internal resource and also by using the funding resources mobilized through the partnership it established from UN Agencies, to tackle the social and economic impacts leaving on the daily condition of refugees, internal displaced persons (IDPs), returnees and vulnerable host communities in Ethiopia. ANE’s COVID-19 Prevention Programs cover identified settlement areas of refugee, internally displaced persons (IDPs) and returnees from internal displacement in Oromia, Somali, Gambella, Benishangul Gumuz Regional States and Addis Ababa City Administration. ANE strongly believes that COVID-19 has serious posed a series of threats on daily living conditions of vulnerable people leading them to encounter crisis associated with health, 1 social and economic. COVID-19 can disrupt the ongoing humanitarian assistance and can worsen the poverty level conditions unless otherwise it is mitigated through application health advisory notes alerted by the Ethiopian Ministry of Health to contain its transmission. Below extracts brief report on ANE COVID-19 plans and achievements obtained -

DRC East Africa and Great Lakes Annual Report 2018
ANNUAL REPORT 2018 East AFRICA & great lakes 2018 KEY HIGHLIGHTS Beneficiaries assisted together various regional initiatives engaged in data • In 2018, Danish Refugee Council (DRC) and Danish collection, research, analysis and policy development on Demining Group (DDG) assisted more than 1,796,623 mixed migration issues providing a new global network beneficiaries (refugees, IDPs and host communities) of mixed migration expertise. The re-branding process through our sectors of expertise including emergency also led to the launch of a new global MMC website response assistance, solutions programming and activities http://www.mixedmigration.org/, which provides quality aimed at addressing root causes. DRC/DDG strives information and analysis to improve decision-making for quality while reaching as many people as possible for people on the move through East Africa and Yemen, integrating our activities across sectors, keeping our work as well as for host governments, donors, academia, grounded on humanitarian principles, and ensuring that researchers and humanitarian organizations who are protection is at the centre of our efforts to reach those interested in mixed migration. most in need. DRC Dynamics Regional presence expansion • A gradual roll out and implementation of a new Enterprise • Given the increased complexity and scale of crises in the Resource Planning (ERP) system, called DRC Dynamics, region, DRC’s commitment to provide direct assistance to that supports the management and oversight of Finance, conflict affected populations in the region remains key. In Grants, Supply Chain, Human Resources and Customer 2018, DRC successfully registered and set up a new office Relationship Management (CRM) began in 2018. DRC in Burundi. -

ETHIOPIA HUMANITARIAN SITUATION REPORT 30 November 2018
UNICEF ETHIOPIA HUMANITARIAN SITUATION REPORT 30 November 2018 ETHIOPIA Humanitarian Situation Report Classmates and best friends, Solomon and Jabir. “We are both 12 years old too” said Solomon, 5th grade at Tsore Arumela Primary School, Assosa. © UNICEF Ethiopia/2018/Tedesse SITUATION IN NUMBERS SitRep # 11– Reporting Period 01-30 November 2018 Highlights 7.95 million* ▪ UNICEF and the Federal Ministry of Health have validated Acute Malnutrition People in need of relief food/cash Guidelines that revise the Mid-Upper Arm Circumference (MUAC) for Severe Acute Malnutrition (SAM) from 11.0 to 11.5 cm. The change will have a 370,000* significant impact on reported SAM cases in 2019. Children in need of treatment for severe acute malnutrition ▪ In collaboration with the World Health Organization (WHO), UNICEF supported a yellow fever vaccination campaign from 16-23 November in nine woredas of Wolayita and Gamo Gofa zones in Southern Nations, 2.6 million* Nationalities Peoples’ region reaching over 1.5 million people. School-aged children, including adolescents, in need of emergency school feeding and learning material ▪ As 2018 comes to an end, the Ethiopian Humanitarian and Disaster assistance Resilience Plan (HDRP) remains substantially underfunded while the needs of conflict displaced populations remain critical. Conflict displacement is expected to continue through 2019. 2.8 million** Internally displaced people in Ethiopia (80 per cent UNICEF’s response with partners displaced due to conflict) Sector/Cluster UNICEF 919,938*** Registered