Montserrat, an Island in the Leeward Group in the Eastern Caribbean
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Caribbean Food Crops Society
PROCEEDINGS OF THE CARIBBEAN FOOD CROPS SOCIETY EIGHTH ANNUAL MEETING SANTO DOMINGO DOMINICAN REPUBLIC 197 0 VOLUME VIII 29 THE EVALUATION OF TOMATO VARIETIES IN THE LEEWARD ISLANDS: A PROGRESS REPORT St. C. M. Forde Leeward Islands Agronomist University of the West Indies St. John's Antigua INTRODUCTION In the Leeward Islands the production of tomatoes is largely in the hands of peasant farmers who make use of commercially available varieties. The crop is established during the period September- November and matures in December-March which coincides with the dry season and also the period, of lowest mean minimum temperatures (70- 72°F). Even at the peak of production, local market demands in Antigua and St. Kitts are not satisfied, but production levels in Montserrat allow for some export of produce to the New York as well as other Caribbean markets. The main problems associated with the industry are the evalua tion of commercially available varieties according to time of plan- ting, and extending production into the dry season by the introduc- tion of irrigation. At the University of the West Indies research in tomato breeding is aimed at developing varieties for increased yield under dry season conditions and high yielding varieties that will set fruit at night temperatures above 72° for wet season production. However there is a pressing need in the Leeward Islands to examine the performance of the commercial varieties available in the area, especially in relation to time of planting. It is against this background that this work was undertaken. MATERIALS AND METHODS Five 6x5 randomised complete block trials were carried out in Antigua, Montserrat and St. -

Modelling Australian Dollar Volatility at Multiple Horizons with High-Frequency Data
risks Article Modelling Australian Dollar Volatility at Multiple Horizons with High-Frequency Data Long Hai Vo 1,2 and Duc Hong Vo 3,* 1 Economics Department, Business School, The University of Western Australia, Crawley, WA 6009, Australia; [email protected] 2 Faculty of Finance, Banking and Business Administration, Quy Nhon University, Binh Dinh 560000, Vietnam 3 Business and Economics Research Group, Ho Chi Minh City Open University, Ho Chi Minh City 7000, Vietnam * Correspondence: [email protected] Received: 1 July 2020; Accepted: 17 August 2020; Published: 26 August 2020 Abstract: Long-range dependency of the volatility of exchange-rate time series plays a crucial role in the evaluation of exchange-rate risks, in particular for the commodity currencies. The Australian dollar is currently holding the fifth rank in the global top 10 most frequently traded currencies. The popularity of the Aussie dollar among currency traders belongs to the so-called three G’s—Geology, Geography and Government policy. The Australian economy is largely driven by commodities. The strength of the Australian dollar is counter-cyclical relative to other currencies and ties proximately to the geographical, commercial linkage with Asia and the commodity cycle. As such, we consider that the Australian dollar presents strong characteristics of the commodity currency. In this study, we provide an examination of the Australian dollar–US dollar rates. For the period from 18:05, 7th August 2019 to 9:25, 16th September 2019 with a total of 8481 observations, a wavelet-based approach that allows for modelling long-memory characteristics of this currency pair at different trading horizons is used in our analysis. -
View Currency List
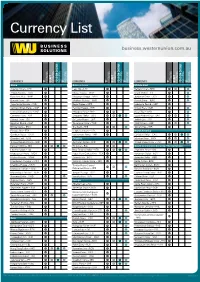
Currency List business.westernunion.com.au CURRENCY TT OUTGOING DRAFT OUTGOING FOREIGN CHEQUE INCOMING TT INCOMING CURRENCY TT OUTGOING DRAFT OUTGOING FOREIGN CHEQUE INCOMING TT INCOMING CURRENCY TT OUTGOING DRAFT OUTGOING FOREIGN CHEQUE INCOMING TT INCOMING Africa Asia continued Middle East Algerian Dinar – DZD Laos Kip – LAK Bahrain Dinar – BHD Angola Kwanza – AOA Macau Pataca – MOP Israeli Shekel – ILS Botswana Pula – BWP Malaysian Ringgit – MYR Jordanian Dinar – JOD Burundi Franc – BIF Maldives Rufiyaa – MVR Kuwaiti Dinar – KWD Cape Verde Escudo – CVE Nepal Rupee – NPR Lebanese Pound – LBP Central African States – XOF Pakistan Rupee – PKR Omani Rial – OMR Central African States – XAF Philippine Peso – PHP Qatari Rial – QAR Comoros Franc – KMF Singapore Dollar – SGD Saudi Arabian Riyal – SAR Djibouti Franc – DJF Sri Lanka Rupee – LKR Turkish Lira – TRY Egyptian Pound – EGP Taiwanese Dollar – TWD UAE Dirham – AED Eritrea Nakfa – ERN Thai Baht – THB Yemeni Rial – YER Ethiopia Birr – ETB Uzbekistan Sum – UZS North America Gambian Dalasi – GMD Vietnamese Dong – VND Canadian Dollar – CAD Ghanian Cedi – GHS Oceania Mexican Peso – MXN Guinea Republic Franc – GNF Australian Dollar – AUD United States Dollar – USD Kenyan Shilling – KES Fiji Dollar – FJD South and Central America, The Caribbean Lesotho Malati – LSL New Zealand Dollar – NZD Argentine Peso – ARS Madagascar Ariary – MGA Papua New Guinea Kina – PGK Bahamian Dollar – BSD Malawi Kwacha – MWK Samoan Tala – WST Barbados Dollar – BBD Mauritanian Ouguiya – MRO Solomon Islands Dollar – -

Montserrat Is a Small Island in the Lesser Antilles, Approximately 30 Miles From
Ceramics Final Report: A Comparison of Ceramic Types from Montserrat Date of Submission: May 7, 2010 Kristie Chin Katherine Harrington Peter Johnson 1 Table of Contents I. INTRODUCTION AND ARCHAEOLOGICAL BACKGROUND ... ERROR! BOOKMARK NOT DEFINED. II. SAMPLE SELECTION ................................................................................................................... 7 III. Research Questions................................................................................................................... 8 IV. Experimental Procedure ......................................................................................................... 9 A. X-RAY FLUORESCENCE 1. Apparatus .............................................................................................................................. 10 2. Procedure .............................................................................................................................. 11 B. SEM-EDS 1. Apparatus .............................................................................................................................. 12 2. Procedure .............................................................................................................................. 12 C. PETROGRAPHY 1. Apparatus .............................................................................................................................. 13 2. Procedure ............................................................................................................................. -

Antigua and Barbuda Citizenship-By-Investment Programme: OPTION 1
INVESTMENT OPTIONS There are two investment options which serve as a qualifier for your ANTIGUA AND application to the Antigua and Barbuda citizenship-by-investment programme: OPTION 1 BARBUDA National Development Fund (NDF) Contribution Main applicant or a family of up to 4: USD 100,000. CITIZENSHIP BY INVESTMENT PROGRAMME For a family of 5 or more: USD 125,000. Global community - Global citizenship OPTION 2 Real Estate Investment ABOUT ANTIGUA AND BARBUDA Approved property: USD 200,000 or 400,000. Antigua and Barbuda is an independent Commonwealth state in the Eastern Caribbean. With GOVERNMENT FEES some 365 beaches of clean turquoise waters, the lush tropical islands of Antigua and Barbuda are an inviting paradise and considered to be one of the most beautiful places in the world. As a NDF: result, tourism is the key driver of Gross Domestic Product (GDP) and generates around 60% of Family up to 4: USD 25,000. the island’s income, with key target markets being the U.S., Canada and Europe. Antigua and Each additonal dependant: USD 15,000. Barbuda is a member of the United Nations, the British Commonwealth, CARICOM and the Real Estate: Organisation of American States (OAS) among many other international organisations. Family up to 4: USD 50,000. Each additional dependent: USD 15,000. WHY ANTIGUA AND BARBUDA TRAVEL WITH EASE PROCESS AND TIMELINE Month 1-2 Sign a retainer agreement and pay the first retainer invoice. The Antigua passport unlocks visa-free travel to over 140 countries including Hong Kong, Preparation Prepare required documentation. Singapore, the UK and the Schengen states.The passport is valid for a period of 5 years and will 10% payment of government fees. -

Antigua and Barbuda Bahamas Barbados Belize British Overseas Territories (Anguilla, Bermuda, British Virgin Islands, Cayman Isla
UNHCR staff monitoring programmes attheLoveAChild field hospital in Fond Parisien, Haiti. Antigua and Barbuda Bahamas Barbados Belize British overseas territories (Anguilla, Bermuda, British Virgin Islands, Cayman Islands, Turks and Caicos Islands, Montserrat) Canada Dominica Dominican Republic Dutch overseas territories in the Caribbean (Aruba, Curaçao, Saint Maarten, Bonaire, Saint Eustatius, Saba) French overseas departments (Martinique, Guadeloupe) Grenada Guyana Haiti Jamaica St. Kitts and Nevis St. Lucia St. Vincent and the Grenadines Suriname Trinidad and Tobago United States of America 348 UNHCR Global Report 2010 and the OPERATIONAL HIGHLIGHTS l UNHCR continued to seek the political and financial l More than 80 per cent of UNHCR’s global resettlement support of the Governments of the United States and referrals are to the United States and Canada. Canada in order to fulfil its protection mandate and find comprehensive solutions for refugees. Working environment l In the United States, UNHCR sought to ensure that the country’s laws and policies, as well as their implementation, In the United States, the Government has confirmed its were in accordance with its obligations under the 1967 commitment to international obligations, particularly with Protocol Relating to the Status of Refugees. Specifically, regard to the parole of asylum-seekers. However, UNHCR promoted reforms to the way in which the refugee adjudications by the immigration courts and administrative definition is being applied under US law and monitored the and federal -

Countries Codes and Currencies 2020.Xlsx
World Bank Country Code Country Name WHO Region Currency Name Currency Code Income Group (2018) AFG Afghanistan EMR Low Afghanistan Afghani AFN ALB Albania EUR Upper‐middle Albanian Lek ALL DZA Algeria AFR Upper‐middle Algerian Dinar DZD AND Andorra EUR High Euro EUR AGO Angola AFR Lower‐middle Angolan Kwanza AON ATG Antigua and Barbuda AMR High Eastern Caribbean Dollar XCD ARG Argentina AMR Upper‐middle Argentine Peso ARS ARM Armenia EUR Upper‐middle Dram AMD AUS Australia WPR High Australian Dollar AUD AUT Austria EUR High Euro EUR AZE Azerbaijan EUR Upper‐middle Manat AZN BHS Bahamas AMR High Bahamian Dollar BSD BHR Bahrain EMR High Baharaini Dinar BHD BGD Bangladesh SEAR Lower‐middle Taka BDT BRB Barbados AMR High Barbados Dollar BBD BLR Belarus EUR Upper‐middle Belarusian Ruble BYN BEL Belgium EUR High Euro EUR BLZ Belize AMR Upper‐middle Belize Dollar BZD BEN Benin AFR Low CFA Franc XOF BTN Bhutan SEAR Lower‐middle Ngultrum BTN BOL Bolivia Plurinational States of AMR Lower‐middle Boliviano BOB BIH Bosnia and Herzegovina EUR Upper‐middle Convertible Mark BAM BWA Botswana AFR Upper‐middle Botswana Pula BWP BRA Brazil AMR Upper‐middle Brazilian Real BRL BRN Brunei Darussalam WPR High Brunei Dollar BND BGR Bulgaria EUR Upper‐middle Bulgarian Lev BGL BFA Burkina Faso AFR Low CFA Franc XOF BDI Burundi AFR Low Burundi Franc BIF CPV Cabo Verde Republic of AFR Lower‐middle Cape Verde Escudo CVE KHM Cambodia WPR Lower‐middle Riel KHR CMR Cameroon AFR Lower‐middle CFA Franc XAF CAN Canada AMR High Canadian Dollar CAD CAF Central African Republic -

New France (Ca
New France (ca. 1600-1770) Trade silver, beaver, eighteenth century Manufactured in Europe and North America for trade with the Native peoples, trade silver came in many forms, including ear bobs, rings, brooches, gorgets, pendants, and animal shapes. According to Adam Shortt,5 the great France, double tournois, 1610 Canadian economic historian, the first regular Originally valued at 2 deniers, the system of exchange in Canada involving Europeans copper “double tournois” was shipped to New France in large quantities during occurred in Tadoussac in the early seventeenth the early 1600s to meet the colony’s century. Here, French traders bartered each year need for low-denomination coins. with the Montagnais people (also known as the Innu), trading weapons, cloth, food, silver items, and tobacco for animal pelts, especially those of the beaver. Because of the risks associated with In 1608, Samuel de Champlain founded transporting gold and silver (specie) across the the first colonial settlement at Quebec on the Atlantic, and to attract and retain fresh supplies of St. Lawrence River. The one universally accepted coin, coins were given a higher value in the French medium of exchange in the infant colony naturally colonies in Canada than in France. In 1664, became the beaver pelt, although wheat and moose this premium was set at one-eighth but was skins were also employed as legal tender. As the subsequently increased. In 1680, monnoye du pays colony expanded, and its economic and financial was given a value one-third higher than monnoye needs became more complex, coins from France de France, a valuation that held until 1717 when the came to be widely used. -

How One Dollar Grew Over Time
MFS ADVISOR EDGESM INVESTING BASICS How One Dollar Grew Over Time mfs.com Stocks — historically, a good place for long-term investors Worldwide Despite the many national and international crises throughout the past 30 years, COVID-19 investing in stocks has kept investors on track in pursuing their long-term goals. pandemic N. Korea STOCK defies $21.11 world with missile testing Oil prices Oil prices War plunge at record to 5-year with Iraq levels 9/11 begins Looming US low Y2K terrorist S&P 500 and “Fiscal Cliff” concerns attacks Hurricanes Dow fall to crisis on US Corporate Katrina and 10-year lows Wilma Dow Asian accounting breaks economic scandals President turmoil US BONDS 5000, $5.53 Bush Soviet market signs Union “too high” CASH NAFTA $2.14 collapses INFLATION $1 $1.95 1/91 1/96 1/01 1/06 1/11 1/16 12/20 Source: SPAR, Bureau of Labor Statistics. Important risk considerations MARKET SEGMENT REPRESENTED BY IMPORTANT RISK CONSIDERATIONS Stocks Standard & Poor’s 500 Stock Index1 Stocks: Common stocks generally provide an opportunity for more capital appreciation than fixed-income investments US Bonds Bloomberg Barclays U.S. Aggregate Bond Index2 but are also subject to greater market fluctuations. US Bonds and Cash: Corporate bonds, US Treasury bills, and US Cash FTSE 3-month Treasury Bill Index3 government bonds fluctuate in value, but if held to maturity, offer a fixed rate of return and a fixed principal value. Inflation Consumer Price Index4 Keep in mind that all investments, including mutual funds, carry a certain amount of risk including the possible loss of the principal amount invested. -

The Post-Slavery Caribbean Plantation Complex∗
Franchise Extension and Elite Persistence: The Post-Slavery Caribbean Plantation Complex∗ Christian Dippely July 20th 2011 Preliminary - Comments Welcome Abstract What determines the extension of the franchise to the poor? This paper studies the 19th century development of parliamentary institutions in the 17 British Caribbean slave colonies. After abolition, freed slaves began to obtain the franchise as small- holders. I document that the elite’s response was a series of constitutional changes in which local parliaments voted to restrict their own powers or abolish themselves altogether in favor of direct colonial rule. This “defensive franchise contraction” hap- pened later or not at all where the franchise expanded less and political turnover re- mained lower, suggesting it was aimed at excluding the new smallholder class from the political process. Against its stated aim, direct colonial rule led to increases in coercive expenditure and decreases in public good provision, suggesting it did not reduce planter elites’ insider access to the colonial administration. A new data-set on the identity of all elected and nominated politicians in the colonies from 1838 to 1900 confirms that planter interests continued to dominate the reformed legislatures under direct colonial rule. Keywords: Economic Development, Elite Persistence, Political Inequality, Institutions, Fran- chise Extension. ∗I thank Toke Aidt, Dwayne Benjamin, Loren Brandt, Mauricio Drelichman, Gilles Duranton, Peter Morrow and Dan Trefler and participants of the 2011 CEGE conference for valuable discussions and insightful comments yDepartment of Economics, University of Toronto (email: [email protected]) 1 Introduction The 19th century is generally viewed as the century in which the franchise was for the first time extended to broad segments of society. -

Tier 1 Countries Annual Dues
Tier 1 Countries Tier 1 Countries Tier 2 Countries Tier 3 Countries Tier 4 Countries Annual Dues - $250 (continued) Annual Dues - $100 Annual Dues - $50 Annual Dues - $20 Qatar Andorra San Marino Albania Angola Afghanistan Antigua and Barbuda Saudi Arabia Algeria Anguilla Benin Argentina Seychelles American Samoa Bangladesh Burkina Faso Aruba Singapore Armenia Bhutan Burundi Australia Sint Maarten Azerbaijan Bolivia Central African Rep. Austria Slovak Republic Belarus Cabo Verde Chad Bahamas Slovenia Belize Cambodia Comoros Bahrain South Korea Bosnia/Herzegovina Cameroon Dem. Rep. of Congo Barbados Spain Botswana Congo Eritrea Belgium St Kitts/Nevis Brazil Cook Islands Ethiopia Bermuda St Martin Bulgaria Côte d’Ivoire Gambia British Virgin Islands Sweden China Djibouti Guinea Brunei Darussalam Switzerland Colombia Egypt Guinea-Bissau Canada Taiwan Costa Rica El Salvador Haiti Cayman Islands Trinidad/Tobago Cuba French Guiana Liberia Channel Islands Turks and Caicos Dominica French So. Territories Madagascar Chile United Arab Emirates Dominican Republic Georgia Malawi Croatia United Kingdom Ecuador Ghana Mali Curacao United States Equatorial Guinea Guadeloupe Mozambique Cyprus Uruguay Fiji Honduras Nepal Czech Republic Virgin Islands Gabon India Niger Denmark Grenada Indonesia North Korea Estonia Guatemala Kenya Rwanda Faroe Islands Guyana Kiribati Senegal Falkland Islands (Malvinas) Iran Kosovo Sierra Leon Finland Iraq Kyrgyz Republic Somalia France Jamaica Lao PDR South Sudan French Polynesia Jordan Lesotho Syrian Arab Republic Germany -

Citizenship, Descent and Place in the British Virgin Islands
Bill Maurer Sta1iford University Children of Mixed Marriages on Virgin Soil: Citizenship, Descent and Place in the British Virgin Islands In this essay, I describe a three-stranded argument over who has rightful claim to citizenship in the British Virgin Islands (BVI). Specifically, this essay demonstrates how the law conjures up a domain of "nature" that infonns positions in this argument. There are three parties to this debate: citizens of the BVI who never went abroad for education and employment, citizens of the BVI who left the territory in the 1960s and are now returning, and immigrants to the BVI and their children. For citizens who never emigrated, the law helps construct the nature of identity in tenns of descent, blood, and "race." For immigrants and their children, who make up fifty percent of the present population, the law lends emphasis to region and jurisdiction to construct identity in tenns of predetennined places. For return emigre British Virgin Islanders, the law enables notions of individual ability that appear to make place- and race-based identities superfluous. I will demonstrate how conceptions of belonging and identity based on place and conceptions based on descent work in concert with notions of individual ability to naturalize inequalities between British Virgin Islanders and immigrants. Specifically, I will focus on the inequalities between those who emigrated and those who stayed behind, and between those who emigrated and those BVIslander and immigrants who now work for them. I argue that the law, especially citizenship but also the laws of jurisdictional division, is critical to the creation and maintenance of these competing identities and the inequalities they cover over or remove from discussion.