Born Too Soon: Care for the Preterm Baby
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Diagnostic Accuracy of Procalcitonin in Critically Ill Immunocompromised
Bele et al. BMC Infectious Diseases 2011, 11:224 http://www.biomedcentral.com/1471-2334/11/224 RESEARCHARTICLE Open Access Diagnostic accuracy of procalcitonin in critically ill immunocompromised patients Nicolas Bele1, Michael Darmon1,2,3, Isaline Coquet1, Jean-Paul Feugeas4, Stéphane Legriel1, Nadir Adaoui4, Benoît Schlemmer1 and Élie Azoulay1* Abstract Background: Recognizing infection is crucial in immunocompromised patients with organ dysfunction. Our objective was to assess the diagnostic accuracy of procalcitonin (PCT) in critically ill immunocompromised patients. Methods: This prospective, observational study included patients with suspected sepsis. Patients were classified into one of three diagnostic groups: no infection, bacterial sepsis, and nonbacterial sepsis. Results: We included 119 patients with a median age of 54 years (interquartile range [IQR], 42-68 years). The general severity (SAPSII) and organ dysfunction (LOD) scores on day 1 were 45 (35-62.7) and 4 (2-6), respectively, and overall hospital mortality was 32.8%. Causes of immunodepression were hematological disorders (64 patients, 53.8%), HIV infection (31 patients, 26%), and solid cancers (26 patients, 21.8%). Bacterial sepsis was diagnosed in 58 patients and nonbacterial infections in nine patients (7.6%); 52 patients (43.7%) had no infection. PCT concentrations on the first ICU day were higher in the group with bacterial sepsis (4.42 [1.60-22.14] vs. 0.26 [0.09- 1.26] ng/ml in patients without bacterial infection, P < 0.0001). PCT concentrations on day 1 that were > 0.5 ng/ml had 100% sensitivity but only 63% specificity for diagnosing bacterial sepsis. The area under the receiver operating characteristic (ROC) curve was 0.851 (0.78-0.92). -

Polymicrobial Septic Shock with Multiorgan Dysfunction in An
JOMA Polymicrobial Septic Shock10.5005/jp-journals-100 with Multiorgan Dysfunction70-0012 CASE REPORT Polymicrobial Septic Shock with Multiorgan Dysfunction in an Otherwise Healthy Immunocompetent Patient 1Anuradha Makkar, 2Inam D Khan, 3KS Rajmohan, 4Syed A Hashmi, 5Lakshmi Nair, 6Alpana Gupta, 7Harleen Chopra, 8Priyanka Banerjee, 9Pragyan S Panda, 10Rajiv M Gupta ABSTRACT Source of support: Nil Background: Sepsis is a significant cause of morbidity and Conflict of interest: None mortality worldwide despite advanced critical life-support. Septic shock and multiorgan dysfunction is the terminal stage INTRODUCTION in critically ill patients leading to perfusion abnormalities, lactic acidosis, oliguria and altered mental status creating a rapid Sepsis is a major cause of morbidity and mortality world- downhill course and mortality. Sepsis ensues through stages wide despite advanced critical life-support. It is the 11th - of exaggerated immune response including systemic inflamma leading cause of death overall with attributable mortality tory response syndrome, in the backdrop of infectious stimuli. to sepsis and severe sepsis being 30 to 50% and 50 to 60%. Case report: Polymicrobial septic shock with multiorgan Following a non-infectious or infectious insult, there is dysfunction leads to demise in an otherwise healthy immuno- competent patient. Microbiological profile revealedEscherichia a preliminary systemic response which becomes over- coli urinary tract infection (UTI), Staphylococcus sciuri bactere- whelming leading to systemic inflammatory response mia, Acinetobacter baumanii ventilator-associated pneumonia, syndrome. When the compensatory anti-inflammatory and central line catheter tip Pseudomonas aeruginosa, thereby reaction fails, it leads to immunomodulatory failure, pointing towards polymicrobial sepsis. Neutropenia of 290/ dL along with serum procalcitonin 5 ng/mL was detected. -

Annual Meeting
Volume 97 | Number 5 Volume VOLUME 97 NOVEMBER 2017 NUMBER 5 SUPPLEMENT SIXTY-SIXTH ANNUAL MEETING November 5–9, 2017 The Baltimore Convention Center | Baltimore, Maryland USA The American Journal of Tropical Medicine and Hygiene The American Journal of Tropical astmh.org ajtmh.org #TropMed17 Supplement to The American Journal of Tropical Medicine and Hygiene ASTMH FP Cover 17.indd 1-3 10/11/17 1:48 PM Welcome to TropMed17, our yearly assembly for stimulating research, clinical advances, special lectures, guests and bonus events. Our keynote speaker this year is Dr. Paul Farmer, Co-founder and Chief Strategist of Partners In Health (PIH). In addition, Dr. Anthony Fauci, Director of the National Institute of Allergy and Infectious Diseases, will deliver a plenary session Thursday, November 9. Other highlighted speakers include Dr. Scott O’Neill, who will deliver the Fred L. Soper Lecture; Dr. Claudio F. Lanata, the Vincenzo Marcolongo Memorial Lecture; and Dr. Jane Cardosa, the Commemorative Fund Lecture. We are pleased to announce that this year’s offerings extend beyond communicating top-rated science to direct service to the global community and a number of novel events: • Get a Shot. Give a Shot.® Through Walgreens’ Get a Shot. Give a Shot.® campaign, you can not only receive your free flu shot, but also provide a lifesaving vaccine to a child in need via the UN Foundation’s Shot@Life campaign. • Under the Net. Walk in the shoes of a young girl living in a refugee camp through the virtual reality experience presented by UN Foundation’s Nothing But Nets campaign. -
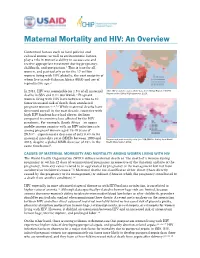
Maternal Mortality and HIV: an Overview
Maternal Mortality and HIV: An Overview Contextual factors such as local policies and cultural norms, as well as socioeconomic factors, play a role in women’s ability to access care and receive appropriate treatment during pregnancy, childbirth, and postpartum.1 This is true for all women, and particularly so for the 17 million women living with HIV globally, the vast majority of whom live in sub-Saharan Africa (SSA) and are of reproductive age.2 In 2013, HIV was responsible for 1.5% of all maternal Adult HIV prevalence rates, 2012 data from Global Report: UNAIDS Report on the Global AIDS Epidemic 2013. deaths in SSA and 0.4% worldwide.3 Pregnant women living with HIV have between a two to 10 times increased risk of death than uninfected pregnant women.4,5,6,7,8 While maternal deaths have decreased overall in the past decade, countries with high HIV burdens have had slower declines compared to countries less affected by the HIV pandemic. For example, South Africa—an upper middle-income country with an HIV infection rate among pregnant women aged 15-49 years of 29.5%9—experienced a decrease of only 0.4% in its maternal mortality ratio (MMR) between 1990 and Data on maternal mortality ratio (per 100,000 live births) from World 2013, despite a global MMR decrease of 45% in the Health Organization 2012. same timeframe10. CAUSES OF MATERNAL MORBIDITY AND MORTALITY AMONG WOMEN LIVING WITH HIV The World Health Organization (WHO) defines maternal death as “the death of a woman during pregnancy or within 42 days of termination of pregnancy irrespective -

Introduction to the Maternal and Newborn Quality of Care Surveys
INTRODUCTION TO THE MATERNAL AND NEWBORN QUALITY OF CARE SURVEYS Introduction To The Quality of Care Surveys i The Maternal and Child Health Integrated Program (MCHIP) is the United States Agency for International Development’s Bureau for Global Health flagship maternal, neonatal and child health program. MCHIP supports programming in maternal, newborn and child health, immunization, family planning, malaria and HIV/AIDS, and strongly encourages opportunities for integration. Cross-cutting technical areas include water, sanitation, hygiene, urban health and health systems strengthening. This study was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Leader with Associates Cooperative Agreement GHS-A-00-08-00002-00. The contents are the responsibility of the Maternal and Child Health Integrated Program (MCHIP) and do not necessarily reflect the views of USAID or the United States Government. Published by: Jhpiego Brown’s Wharf 1615 Thames Street Baltimore, Maryland 21231-3492, USA January 2013 Introduction To The Quality of Care Surveys ii 1. BACKGROUND Improving the quality of obstetric care in facilities has recently been identified as a neglected and essential approach to reducing maternal deaths and enabling developing countries to achieve Millennium Development Goal (MDG) 4 and 5.1 Postpartum hemorrhage is the most frequent cause of maternal deaths globally and in developing countries, accounting for 25% of maternal deaths. Next are hypertensive disorders in pregnancy (PE/E) at 15%, sepsis (8%) and obstructed labor (7%).2 Effective interventions exist for screening, preventing and treating obstetric and newborn complications, and they can be readily provided by skilled providers in facilities. -

Procalcitonin and Its Limitations: Why a Biomarker's Best Isn't Good Enough
POINT/COUNTERPOINT Counterpoint Procalcitonin and Its Limitations: Why a Biomarker's Best Isn't Good Enough Ayesha Farooq1 and Jessica M. Colón-Franco1* Sepsis-related conditions remain the leading Intended uses now include supporting antibiotic Downloaded from https://academic.oup.com/jalm/article/3/4/716/5603063 by guest on 23 September 2021 causes of mortality, morbidity, and expenditures management decisions in respiratory infections worldwide despite efforts to standardize care and and sepsis. There is no reference method for PCT. expedite diagnosis and treatment, which are de- The BRAHMS Kryptor sensitive PCT assay (Thermo- terminants of outcome. As with most syndromes Fisher Scientific) and its predecessor were initially with complex pathophysiology, no gold standard available and used to derive PCT cutoffs. The diagnostic test exists. Diagnosis is complicated by BRAHMS assay can be run in automated immuno- nonspecific symptoms and lengthy blood cultures assay instruments from partner companies. Simi- with high false-negative rates. Empiric antibiotic larly, the Diazyme PCT immunotubidimetric assay treatment upon signs of sepsis is an increasing (Diazyme Laboratories) can be implemented in concern for antibiotic overuse and resistance. The common chemistry analyzers. This widespread need for biochemical biomarkers for sepsis diag- availability of PCT assays is facilitating clinical use nosis is well accepted. Several pro- and antiinflam- but analytical considerations come into play. The matory biomarkers have been investigated, but functional sensitivity of the Diazyme PCT assay is only few are incorporated in clinical practice (1). higher than the BRAHMS assay and above the Procalcitonin (PCT)2 is one such molecule that reference interval of healthy individuals (2, 3). -

Procalcitonin (PCT)
Procalcitonin (PCT) Guidance Background: Up to 50% of antimicrobial use in the inpatient setting is unneeded or inappropriate.1 For example, viruses are typically the cause of acute bronchitis but despite this as much as 80% of patients will be prescribed antibiotics.2 Also the length of treatment for most infections has been poorly studied and it is likely that treatment durations are inappropriately long.3 The appropriate use of antimicrobials is essential because they are associated with patient harm including drug toxicity, increased drug resistance, and collateral damage such as Clostridium diffiicile-associated diarrhea.4-6 Procalcitonin has been evaluated as a biomarker to assist the clinician in the diagnosis and treatment of bacterial infection. Procalcitonin has been studied most thoroughly for lower respiratory tract infections and sepsis and its use is associated with decreased antimicrobial usage without worsening of clinical outcomes.7-13 What is Procalcitonin?14-16 Procalcitonin (PCT) is a 116 amino acid precursor of calcitonin which under normal circumstances is produced by the thyroid C-cells. Serum concentrations of PCT are normally <0.05 ng/mL but in circumstances of systemic inflammation, particularly bacterial infection, PCT is produced in large quantities by many body tissues. It is detectable within 2-4 hours and peaks within 6-24 hours (as opposed to CRP which begins to rise after 12-24 hours and peaks at 48 hours). 14-16 PCT production is not impaired by neutropenia or other immunosuppressive states. PCT levels parallel the severity of the inflammatory insult or infection meaning those with more severe disease have higher levels. -
Next-Generation Lab-On-A-Chip Devices
Next-generation lab-on-a-chip devices Samuel Sia, Ph.D. Associate Professor Department of Biomedical Engineering Columbia University APHL, Little Rock June 4, 2014 Clinical ELISA testing... ELISA ideal method low cost? - capital -per test compact? rapid? simple to operate? sensitive (pM)? distinguishes quantitative differences? amenable to parallel analysis? operable without ground electricity? works in field conditions (sunlight)? • coat surface with antigen (overnight) • block with 1% BSA or 0.05% Tween-20 (1 hr) uses accessible • add sample containing antibody to be tested (1 hr) reagents? • add enzyme-conjugated antibody (1 hr) • add substrate (10 min.) “Plug-in cartridge” (bubble-based reagent delivery) 17 pM 170 pM 1.7 nM 17 nM 170 nM 1.7 M Fluorescent antibody Sample Wash Wash Fluorescent Air spacers antibody 200 m Vacuum Antibody in sample Antigen 1200 1000 800 500-m 600 width 250-m 400 50-m width width total time = 2 min. 200 500-m (hands-free) width 0 Normalized fluorescence (a.u.) fluorescence Normalized 0.1 10 1000 Concentration of anti-rabbit IgG (nM) Linder, Sia, and Whitesides, Anal. Chem., 77:64 (2005) Silver reduction enables the use of microfluidics Angew Chemie, 43:498 (2004) ELISA mChip signal generation enzyme/substrate silver precipitation reaction (photography) light source lasers, lenses, filters LEDs (ambient lighting) detector photomultiplier tubes photodetector (photocopier) manufacturing plastic 96-well plates injection-molded plastic (consumer toys) Point-of-care ELISA Founded in 2004 (with Vincent Linder and David Steinmiller), based in Boston area raised ~$12M in VC funding First product: prostate cancer monitoring ISO-certified manufacturing facility and clean room approved in Europe (CE Mark) acquired by Opko Health in 2011 (~$50M) awaiting FDA approval and launch of PSA test and eventually 4K panel (total PSA, free PSA, intact PSA, HK2) Clinical scenario Pregnant woman in high burden-of-disease area (health clinic in U.S. -

Prevention and Control of Malaria in Pregnancy in the African Region
P R E V E N T I O N A N D C O N T R O L O F M A L A R I A I N PREGNANC Y I N THE A FRIC AN R EGION A Program Implementation Guide P R E V E N T I O N A N D C O N T R O L O F M A L A R I A I N PREGNANC Y I N THE A FRIC AN R EGION A Program Implementation Guide For information: Jhpiego 1615 Thames Street Baltimore, MD 21231-3492, USA Tel: 410.537.1800 www.jhpiego.org Editor: Ann Blouse Graphic Design: Trudy Conley The ACCESS Program is the U.S. Agency for International Developments global program to improve maternal and newborn health. The ACCESS Program works to expand coverage, access and use of key maternal and newborn health services across a continuum of care from the household to the hospitalwith the aim of making quality health services accessible as close to the home as possible. Jhpiego implements the program in partnership with Save the Children, the Futures Group, the Academy for Educational Development, the American College of Nurse- Midwives and IMA World Health. www.accesstohealth.org Jhpiego is an international, non-profit health organization affiliated with The Johns Hopkins University. For nearly 40 years, Jhpiego has empowered front-line health workers by designing and implementing effective, low-cost, hands-on solutions to strengthen the delivery of health care services for women and their families. By putting evidence-based health innovations into everyday practice, Jhpiego works to break down barriers to high-quality health care for the worlds most vulnerable populations. -
Equity Matters: Lessons from MCHIP and CSHGP in Measuring and Improving Equity
Equity Matters: Lessons from MCHIP and CSHGP in Measuring and Improving Equity June 2014 Authors: Jennifer Winestock Luna Tanvi Monga Lindsay Morgan Suggested citation: Winestock Luna J, Monga T, and Morgan L. 2014. Equity Matters – Lessons from MCHIP and CSHGP in Measuring and Improving Equity. Maternal Child Health Integrated Program. This report was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Leader with Associates Cooperative Agreement GHS-A-00-08-00002-00. The contents are the responsibility of the Maternal and Child Health Integrated Program (MCHIP) and do not necessarily reflect the views of USAID or the United States Government. The Maternal and Child Health Integrated Program (MCHIP) is the USAID Bureau for Global Health’s flagship maternal, neonatal and child health (MNCH) program. MCHIP supports programming in maternal, newborn and child health, immunization, family planning, malaria, nutrition, and HIV/AIDS, and strongly encourages opportunities for integration. Cross-cutting technical areas include water, sanitation, hygiene, urban health and health systems strengthening. www.mchip.net Table of Contents ABBREVIATIONS AND ACRONYMS ......................................................................................................... iv INTRODUCTION ....................................................................................................................................... 1 CONTRIBUTIONS BY MCHIP AND -
Reaching Underserved Populations: Leveraging Point-Of-Care Tests for Sexually Transmitted and Blood-Borne Infections to Explore New Program Options in Canada
Reaching Underserved Populations: Leveraging Point-of-Care Tests for Sexually Transmitted and Blood-Borne Infections to Explore New Program Options in Canada Review of the Evidence March, 2018 Prepared by Megan Smallwood, MSc, Reaching Underserved populations: Leveraging Point-of-Care Tests for Sexually Transmitted and Blood-Borne Infections to Explore New Program Options in Canada Review of the Evidence March, 2018 Prepared by Megan Smallwood, MSc Contact us at: National Collaborating Centre for Infectious Diseases Rady Faculty of Health Sciences, University of Manitoba Tel: (204) 318‐2591 Email: [email protected] www.nccid.ca This is NCCID Project number 382 Production of this document has been made possible through a financial contribution from the Public Health Agency of Canada through funding for the National Collaborating Centre for Infectious Diseases. The views expressed herein do not necessarily represent the views of the Public Health Agency of Canada. Table of Contents Introduction .................................................................................................................................................. 1 Sexually Transmitted and Blood‐borne Infections (STBBIs) in Canada ..................................................... 1 Point‐of‐Care Diagnostics ......................................................................................................................... 2 Aim of this Evidence Review .................................................................................................................... -

Procalcitonin and C-Reactive Protein in the Diagnosis of Spontaneous Bacterial Peritonitis
10 Original Article Procalcitonin and C-reactive protein in the diagnosis of spontaneous bacterial peritonitis Rajanshu Verma1, Sanjaya K. Satapathy2,3, Muhammad Bilal4 1Transplant Hepatology/Gastroenterology fellow, University of Tennessee Health Sciences Center, Memphis, TN, USA; 2Department of Transplant Surgery, Methodist University Hospital Transplant Institute/University of Tennessee Health Sciences Center, Memphis, TN, USA; 3Medical Director of Liver Transplantation, Division of Hepatology, Sandra Atlas Bass Center for Liver Diseases and Liver Transplantation, Northwell Health/North Shore University Hospital, Manhasset, New York, USA; 4Department of Gastroenterology, University of Tennessee Health Sciences Center, Memphis, Tennessee, USA Contributions: (I) Conception and design: M Bilal; (II) Administrative support: SK Satapathy, M Bilal; (III) Provision of study materials or patients: M Bilal; (IV) Collection and assembly of data: M Bilal, R Verma; (V) Data analysis and interpretation: R Verma, SK Satapathy; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Muhammad Bilal, MD. Department of Gastroenterology, University of Tennessee Health Sciences Center, Memphis, Tennessee, USA. Email: [email protected]. Background: Spontaneous bacterial peritonitis (SBP) is a serious complication of cirrhosis and is associated with high morbidity and mortality. Rapid institution of appropriate antibiotics is central to the improved patient outcome. Correctly obtaining ascites fluid for analysis has several technical and logistic limitations resulting in overuse of empiric antibiotics when patients are admitted to the hospital with suspected SBP. Procalcitonin and C-reactive protein (CRP) are non-invasive markers of infection. We conducted a study to illustrate the role of these markers in making the diagnosis of SBP in patients with cirrhosis.