(IPT) of Malaria in Pregnancy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Annual Meeting
Volume 97 | Number 5 Volume VOLUME 97 NOVEMBER 2017 NUMBER 5 SUPPLEMENT SIXTY-SIXTH ANNUAL MEETING November 5–9, 2017 The Baltimore Convention Center | Baltimore, Maryland USA The American Journal of Tropical Medicine and Hygiene The American Journal of Tropical astmh.org ajtmh.org #TropMed17 Supplement to The American Journal of Tropical Medicine and Hygiene ASTMH FP Cover 17.indd 1-3 10/11/17 1:48 PM Welcome to TropMed17, our yearly assembly for stimulating research, clinical advances, special lectures, guests and bonus events. Our keynote speaker this year is Dr. Paul Farmer, Co-founder and Chief Strategist of Partners In Health (PIH). In addition, Dr. Anthony Fauci, Director of the National Institute of Allergy and Infectious Diseases, will deliver a plenary session Thursday, November 9. Other highlighted speakers include Dr. Scott O’Neill, who will deliver the Fred L. Soper Lecture; Dr. Claudio F. Lanata, the Vincenzo Marcolongo Memorial Lecture; and Dr. Jane Cardosa, the Commemorative Fund Lecture. We are pleased to announce that this year’s offerings extend beyond communicating top-rated science to direct service to the global community and a number of novel events: • Get a Shot. Give a Shot.® Through Walgreens’ Get a Shot. Give a Shot.® campaign, you can not only receive your free flu shot, but also provide a lifesaving vaccine to a child in need via the UN Foundation’s Shot@Life campaign. • Under the Net. Walk in the shoes of a young girl living in a refugee camp through the virtual reality experience presented by UN Foundation’s Nothing But Nets campaign. -
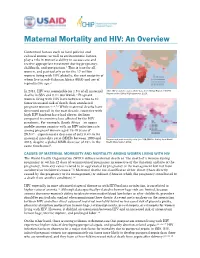
Maternal Mortality and HIV: an Overview
Maternal Mortality and HIV: An Overview Contextual factors such as local policies and cultural norms, as well as socioeconomic factors, play a role in women’s ability to access care and receive appropriate treatment during pregnancy, childbirth, and postpartum.1 This is true for all women, and particularly so for the 17 million women living with HIV globally, the vast majority of whom live in sub-Saharan Africa (SSA) and are of reproductive age.2 In 2013, HIV was responsible for 1.5% of all maternal Adult HIV prevalence rates, 2012 data from Global Report: UNAIDS Report on the Global AIDS Epidemic 2013. deaths in SSA and 0.4% worldwide.3 Pregnant women living with HIV have between a two to 10 times increased risk of death than uninfected pregnant women.4,5,6,7,8 While maternal deaths have decreased overall in the past decade, countries with high HIV burdens have had slower declines compared to countries less affected by the HIV pandemic. For example, South Africa—an upper middle-income country with an HIV infection rate among pregnant women aged 15-49 years of 29.5%9—experienced a decrease of only 0.4% in its maternal mortality ratio (MMR) between 1990 and Data on maternal mortality ratio (per 100,000 live births) from World 2013, despite a global MMR decrease of 45% in the Health Organization 2012. same timeframe10. CAUSES OF MATERNAL MORBIDITY AND MORTALITY AMONG WOMEN LIVING WITH HIV The World Health Organization (WHO) defines maternal death as “the death of a woman during pregnancy or within 42 days of termination of pregnancy irrespective -

Introduction to the Maternal and Newborn Quality of Care Surveys
INTRODUCTION TO THE MATERNAL AND NEWBORN QUALITY OF CARE SURVEYS Introduction To The Quality of Care Surveys i The Maternal and Child Health Integrated Program (MCHIP) is the United States Agency for International Development’s Bureau for Global Health flagship maternal, neonatal and child health program. MCHIP supports programming in maternal, newborn and child health, immunization, family planning, malaria and HIV/AIDS, and strongly encourages opportunities for integration. Cross-cutting technical areas include water, sanitation, hygiene, urban health and health systems strengthening. This study was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Leader with Associates Cooperative Agreement GHS-A-00-08-00002-00. The contents are the responsibility of the Maternal and Child Health Integrated Program (MCHIP) and do not necessarily reflect the views of USAID or the United States Government. Published by: Jhpiego Brown’s Wharf 1615 Thames Street Baltimore, Maryland 21231-3492, USA January 2013 Introduction To The Quality of Care Surveys ii 1. BACKGROUND Improving the quality of obstetric care in facilities has recently been identified as a neglected and essential approach to reducing maternal deaths and enabling developing countries to achieve Millennium Development Goal (MDG) 4 and 5.1 Postpartum hemorrhage is the most frequent cause of maternal deaths globally and in developing countries, accounting for 25% of maternal deaths. Next are hypertensive disorders in pregnancy (PE/E) at 15%, sepsis (8%) and obstructed labor (7%).2 Effective interventions exist for screening, preventing and treating obstetric and newborn complications, and they can be readily provided by skilled providers in facilities. -
Next-Generation Lab-On-A-Chip Devices
Next-generation lab-on-a-chip devices Samuel Sia, Ph.D. Associate Professor Department of Biomedical Engineering Columbia University APHL, Little Rock June 4, 2014 Clinical ELISA testing... ELISA ideal method low cost? - capital -per test compact? rapid? simple to operate? sensitive (pM)? distinguishes quantitative differences? amenable to parallel analysis? operable without ground electricity? works in field conditions (sunlight)? • coat surface with antigen (overnight) • block with 1% BSA or 0.05% Tween-20 (1 hr) uses accessible • add sample containing antibody to be tested (1 hr) reagents? • add enzyme-conjugated antibody (1 hr) • add substrate (10 min.) “Plug-in cartridge” (bubble-based reagent delivery) 17 pM 170 pM 1.7 nM 17 nM 170 nM 1.7 M Fluorescent antibody Sample Wash Wash Fluorescent Air spacers antibody 200 m Vacuum Antibody in sample Antigen 1200 1000 800 500-m 600 width 250-m 400 50-m width width total time = 2 min. 200 500-m (hands-free) width 0 Normalized fluorescence (a.u.) fluorescence Normalized 0.1 10 1000 Concentration of anti-rabbit IgG (nM) Linder, Sia, and Whitesides, Anal. Chem., 77:64 (2005) Silver reduction enables the use of microfluidics Angew Chemie, 43:498 (2004) ELISA mChip signal generation enzyme/substrate silver precipitation reaction (photography) light source lasers, lenses, filters LEDs (ambient lighting) detector photomultiplier tubes photodetector (photocopier) manufacturing plastic 96-well plates injection-molded plastic (consumer toys) Point-of-care ELISA Founded in 2004 (with Vincent Linder and David Steinmiller), based in Boston area raised ~$12M in VC funding First product: prostate cancer monitoring ISO-certified manufacturing facility and clean room approved in Europe (CE Mark) acquired by Opko Health in 2011 (~$50M) awaiting FDA approval and launch of PSA test and eventually 4K panel (total PSA, free PSA, intact PSA, HK2) Clinical scenario Pregnant woman in high burden-of-disease area (health clinic in U.S. -

Prevention and Control of Malaria in Pregnancy in the African Region
P R E V E N T I O N A N D C O N T R O L O F M A L A R I A I N PREGNANC Y I N THE A FRIC AN R EGION A Program Implementation Guide P R E V E N T I O N A N D C O N T R O L O F M A L A R I A I N PREGNANC Y I N THE A FRIC AN R EGION A Program Implementation Guide For information: Jhpiego 1615 Thames Street Baltimore, MD 21231-3492, USA Tel: 410.537.1800 www.jhpiego.org Editor: Ann Blouse Graphic Design: Trudy Conley The ACCESS Program is the U.S. Agency for International Developments global program to improve maternal and newborn health. The ACCESS Program works to expand coverage, access and use of key maternal and newborn health services across a continuum of care from the household to the hospitalwith the aim of making quality health services accessible as close to the home as possible. Jhpiego implements the program in partnership with Save the Children, the Futures Group, the Academy for Educational Development, the American College of Nurse- Midwives and IMA World Health. www.accesstohealth.org Jhpiego is an international, non-profit health organization affiliated with The Johns Hopkins University. For nearly 40 years, Jhpiego has empowered front-line health workers by designing and implementing effective, low-cost, hands-on solutions to strengthen the delivery of health care services for women and their families. By putting evidence-based health innovations into everyday practice, Jhpiego works to break down barriers to high-quality health care for the worlds most vulnerable populations. -
Equity Matters: Lessons from MCHIP and CSHGP in Measuring and Improving Equity
Equity Matters: Lessons from MCHIP and CSHGP in Measuring and Improving Equity June 2014 Authors: Jennifer Winestock Luna Tanvi Monga Lindsay Morgan Suggested citation: Winestock Luna J, Monga T, and Morgan L. 2014. Equity Matters – Lessons from MCHIP and CSHGP in Measuring and Improving Equity. Maternal Child Health Integrated Program. This report was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Leader with Associates Cooperative Agreement GHS-A-00-08-00002-00. The contents are the responsibility of the Maternal and Child Health Integrated Program (MCHIP) and do not necessarily reflect the views of USAID or the United States Government. The Maternal and Child Health Integrated Program (MCHIP) is the USAID Bureau for Global Health’s flagship maternal, neonatal and child health (MNCH) program. MCHIP supports programming in maternal, newborn and child health, immunization, family planning, malaria, nutrition, and HIV/AIDS, and strongly encourages opportunities for integration. Cross-cutting technical areas include water, sanitation, hygiene, urban health and health systems strengthening. www.mchip.net Table of Contents ABBREVIATIONS AND ACRONYMS ......................................................................................................... iv INTRODUCTION ....................................................................................................................................... 1 CONTRIBUTIONS BY MCHIP AND -
Reaching Underserved Populations: Leveraging Point-Of-Care Tests for Sexually Transmitted and Blood-Borne Infections to Explore New Program Options in Canada
Reaching Underserved Populations: Leveraging Point-of-Care Tests for Sexually Transmitted and Blood-Borne Infections to Explore New Program Options in Canada Review of the Evidence March, 2018 Prepared by Megan Smallwood, MSc, Reaching Underserved populations: Leveraging Point-of-Care Tests for Sexually Transmitted and Blood-Borne Infections to Explore New Program Options in Canada Review of the Evidence March, 2018 Prepared by Megan Smallwood, MSc Contact us at: National Collaborating Centre for Infectious Diseases Rady Faculty of Health Sciences, University of Manitoba Tel: (204) 318‐2591 Email: [email protected] www.nccid.ca This is NCCID Project number 382 Production of this document has been made possible through a financial contribution from the Public Health Agency of Canada through funding for the National Collaborating Centre for Infectious Diseases. The views expressed herein do not necessarily represent the views of the Public Health Agency of Canada. Table of Contents Introduction .................................................................................................................................................. 1 Sexually Transmitted and Blood‐borne Infections (STBBIs) in Canada ..................................................... 1 Point‐of‐Care Diagnostics ......................................................................................................................... 2 Aim of this Evidence Review .................................................................................................................... -

Cultural Beliefs and Perceptions of Maternal Diet and Weight Gain During Pregnancy and Postpartum Family Planning in Egypt
Cultural Beliefs and Perceptions of Maternal Diet and Weight Gain during Pregnancy and Postpartum Family Planning in Egypt Authors: Justine Kavle, Sohair Mehanna, Ghada Khan, Mohamed Hassan, Gulsen Saleh, and Rae Galloway April 2014 Table of Contents TABLES AND FIGURES ........................................................................................................................... iv ACKNOWLEDGMENTS ............................................................................................................................ v ABBREVIATIONS .................................................................................................................................... vi EXECUTIVE SUMMARY .......................................................................................................................... vii Introduction .................................................................................................................................................... vii Methods.......................................................................................................................................................... vii Key Findings .................................................................................................................................................. viii Discussion and Recommendations ................................................................................................................ x Conclusion ...................................................................................................................................................... -

Dual Elimination of Mother-To-Child Transmission of HIV and Congenital Syphilis DIAGNOSTIC TECHNOLOGY LANDSCAPE
2014 Dual elimination of mother-to-child transmission of HIV and congenital syphilis DIAGNOSTIC TECHNOLOGY LANDSCAPE APRIL 2014 UNITAID Secretariat World Health Organization Avenue Appia 20 CH-1211 Geneva 27 Switzerland T +41 22 791 55 03 F +41 22 791 48 90 [email protected] www.unitaid.eu UNITAID is hosted and administered by the World Health Organization © 2014 World Health Organization (Acting as the host organization for the Secretariat of UNITAID) The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind either expressed or implied. The responsibility and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. This report was prepared by Maurine M. Murtagh with support from the Bill & Melinda Gates Foundation and UNITAID. All reasonable precautions have been taken by the author to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. -

Born Too Soon: Care for the Preterm Baby
Lawn et al. Reproductive Health 2013, 10(Suppl 1):S5 http://www.reproductive-health-journal.com/content/10/S1/S5 REVIEW Open Access Born Too Soon: Care for the preterm baby Joy E Lawn*1,2, Ruth Davidge3,4,5, Vinod K Paul6, Severin von Xylander7, Joseph de Graft Johnson8, Anthony Costello9, Mary V Kinney10, Joel Segre11 and Liz Molyneux12 Abstract As part of a supplement entitled “Born Too Soon”, this paper focuses on care of the preterm newborn. An estimated 15 million babies are born preterm, and the survival gap between those born in high and low income countries is widening, with one million deaths a year due to direct complications of preterm birth, and around one million more where preterm birth is a risk factor, especially amongst those who are also growth restricted. Most premature babies (>80%) are between 32 and 37 weeks of gestation, and many die needlessly for lack of simple care. We outline a series of packages of care that build on essential care for every newborn comprising support for immediate and exclusive breastfeeding, thermal care, and hygienic cord and skin care. For babies who do not breathe at birth, rapid neonatal resuscitation is crucial. Extra care for small babies, including Kangaroo Mother Care, and feeding support, can halve mortality in babies weighing <2000 g. Case management of newborns with signs of infection, safe oxygen management and supportive care for those with respiratory complications, and care for those with signifi cant jaundice are all critical, and are especially dependent on competent nursing care. Neonatal intensive care units in high income settings are de-intensifying care, for example increasing use of continuous positive airway pressure (CPAP) and this makes comprehensive preterm care more transferable. -
2010 Revision
For more information, contact: HIV/AIDS Programme World Health Organization Strengthening health services to fight HIV/AIDS Department of HIV/AIDS 20, avenue Appia 1211 Geneva 27 Switzerland E-mail: [email protected] www.who.int/hiv 2010 revision ANTIRETROVIRAL THERAPY FOR HIV INFECTION IN ADULTS AND ADOLESCENTS Recommendations for a public health approach a public health approach for Recommendations Recommendations for a public health approach 2010 revision ISBN 978 92 4 159976 4 Antiretroviral therapyfor HIV infection in adults and adolescents in adults and adolescents HIV infection therapyfor Antiretroviral WHO Library Cataloguing-in-Publication Data Antiretroviral therapy for HIV infection in adults and adolescents: recommendations for a public health approach. – 2010 rev. 1.Anti-retroviral agents - therapeutic use. 2.Anti-retroviral agents - pharmacology. 3.HIV infections – drug therapy. 4.Adult. 5.Adolescent. 6.Guidelines. 7.Developing countries. I.World Health Organization. ISBN 978 92 4 159976 4 (NLM classification: WC 503.2) © World Health Organization 2010 All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. -

Postpartum Family Planning Annotated Bibliography 2008–2014
Postpartum Family Planning Annotated Bibliography 2008–2014 The Maternal and Child Survival Program (MCSP), is a global U.S. Agency for International Development (USAID) cooperative agreement to introduce and support high-impact health interventions in 24 priority countries with the ultimate goal of ending preventable child and maternal deaths (EPCMD) within a generation. MCSP supports programming in in maternal, newborn and child health, immunization, family planning and reproductive health, nutrition, health systems strengthening, water/sanitation/hygiene, malaria, prevention of mother-to-child transmission of HIV, and pediatric HIV care and treatment. MCSP will tackle these issues through approaches that also focus on health systems strengthening, household and community mobilization, gender integration and eHealth, among others. Visit www.mcsprogram.org to learn more. This annotated bibliography was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Leader with Associates Cooperative Agreement GHS-A-00-08-00002-00 and Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of The Maternal and Child Health Integrated Program (MCHIP) and The Maternal and Child Survival Program (MCSP), and do not necessarily reflect the views of USAID or the United States Government. INTRODUCTION Beginning in 2006, the ACCESS-FP program compiled an annotated bibliography of postpartum family planning literature to promote documented best practices and serve as a reference for both researchers and program managers. Updates to the original bibliography were made under ACCESS- FP in 2007, 2008, and 2010, and then again under the Maternal and Child Health Integrated Program, Family Planning team in 2011 and, finally, 2014.