Long Leg Arthropathy* by A
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Juvenile Spondyloarthropathies: Inflammation in Disguise
PP.qxd:06/15-2 Ped Perspectives 7/25/08 10:49 AM Page 2 APEDIATRIC Volume 17, Number 2 2008 Juvenile Spondyloarthropathieserspective Inflammation in DisguiseP by Evren Akin, M.D. The spondyloarthropathies are a group of inflammatory conditions that involve the spine (sacroiliitis and spondylitis), joints (asymmetric peripheral Case Study arthropathy) and tendons (enthesopathy). The clinical subsets of spondyloarthropathies constitute a wide spectrum, including: • Ankylosing spondylitis What does spondyloarthropathy • Psoriatic arthritis look like in a child? • Reactive arthritis • Inflammatory bowel disease associated with arthritis A 12-year-old boy is actively involved in sports. • Undifferentiated sacroiliitis When his right toe starts to hurt, overuse injury is Depending on the subtype, extra-articular manifestations might involve the eyes, thought to be the cause. The right toe eventually skin, lungs, gastrointestinal tract and heart. The most commonly accepted swells up, and he is referred to a rheumatologist to classification criteria for spondyloarthropathies are from the European evaluate for possible gout. Over the next few Spondyloarthropathy Study Group (ESSG). See Table 1. weeks, his right knee begins hurting as well. At the rheumatologist’s office, arthritis of the right second The juvenile spondyloarthropathies — which are the focus of this article — toe and the right knee is noted. Family history is might be defined as any spondyloarthropathy subtype that is diagnosed before remarkable for back stiffness in the father, which is age 17. It should be noted, however, that adult and juvenile spondyloar- reported as “due to sports participation.” thropathies exist on a continuum. In other words, many children diagnosed with a type of juvenile spondyloarthropathy will eventually fulfill criteria for Antinuclear antibody (ANA) and rheumatoid factor adult spondyloarthropathy. -

Bursae Around the Knee Joints Priyank S Chatra Department of Radiology, Yenepoya Medical College, Mangalore, Karnataka, India
MUSCULOSKELETAL RADIOLOGY Bursae around the knee joints Priyank S Chatra Department of Radiology, Yenepoya Medical College, Mangalore, Karnataka, India Correspondence: Dr. Priyank S. Chatra, Department of Radiology, Yenepoya Medical College, Deralakatte, Mangalore – 575 018, Karnataka, India. E-mail: [email protected] Abstract A bursa is a fluid-filled structure that is present between the skin and tendon or tendon and bone. The main function of a bursa is to reduce friction between adjacent moving structures. Bursae around the knee can be classified as those around the patella and those that occur elsewhere. In this pictorial essay we describe the most commonly encountered lesions and their MRI appearance. Key words: Iliotibial bursa; infrapatellar bursa; pes anserine bursa Introduction and the gastrocnemius-semimembranosus bursa. On MRI imaging, bursitis appears as an oblong fluid collection in A bursa is a fluid-filled structure that is present between its expected anatomical location. the skin and tendon or tendon and bone. The main function of a bursa is to reduce friction between adjacent Prepatellar Bursitis moving structures. Typically, bursae are located around large joints such as the shoulder, knee, hip, and elbow.[1] The prepatellar bursa is located between the patella and the Inflammation of this fluid-filled structure is called bursitis. overlying subcutaneous tissue. Chronic trauma in the form Trauma, infection, overuse, and hemorrhage are some of prolonged or repeated kneeling leads to inflammation of the common -

'Dialysis Related Arthropathy': a Survey of 95 Patients Receiving Chronic Haemodialysis with Special Reference to 132 Microglobulin Related Amyloidosis
Ann Rheum Dis: first published as 10.1136/ard.48.5.409 on 1 May 1989. Downloaded from Annals of the Rheumatic Diseases, 1989; 48, 409-420 'Dialysis related arthropathy': a survey of 95 patients receiving chronic haemodialysis with special reference to 132 microglobulin related amyloidosis N P HURST,' R VAN DEN BERG,' A DISNEY,2 M ALCOCK,3 L ALBERTYN,3 M GREEN,' AND V PASCOE4 From the 'Rheumatology Unit, the 2Renal Unit, the 3Department of Radiology, and the 4Department of Pathology, The Queen Elizabeth Hospital, Woodville, South Australia SUMMARY Ninety five patients receiving chronic haemodialysis (CHD) were surveyed to determine the prevalence of rheumatic disease and, where possible, its aetiology. At least three distinct rheumatic syndromes were identified-a group of patients with a syndrome consisting of large and medium joint synovial swelling, restricted hips and shoulders, tenosynovitis, carpal tunnel syndrome, and bone cysts due to deposition of 132 microglobulin related amyloid (AMP2m); a second group with erosive azotaemic osteoarthropathy; and a third group with age related degenerative disease of small, large, and axial joints. The data presented suggest that in patients receiving CHD (a) the prevalence of AM2i2m deposition and the associated syndrome increases with duration of dialysis, but in patients who have been dialysed for more than 10 years the risk of developing AM2n2m is related to age; (b) AM2i2m deposition in subchondral cysts, but not synovium, causes joint destruction; also, AMp2m may be more prone to deposition in synovium of joints already damaged by other processes; (c) in the absence of synovial iron deposition synovial AM2n2m is not associated with an inflammatory infiltrate; (d) hyperparathyroidism and perhaps other factors such as synovial iron deposition are probably more important than AMgi2m as causes http://ard.bmj.com/ of peripheral joint degeneration and destructive spondyloarthropathy in patients receiving CHD. -

Hallux Valgus
MedicalContinuing Education Building Your FOOTWEAR PRACTICE Objectives 1) To be able to identify and evaluate the hallux abductovalgus deformity and associated pedal conditions 2) To know the current theory of etiology and pathomechanics of hallux valgus. 3) To know the results of recent Hallux Valgus empirical studies of the manage- ment of hallux valgus. Assessment and 4) To be aware of the role of conservative management, faulty footwear in the develop- ment of hallux valgus deformity. and the role of faulty footwear. 5) To know the pedorthic man- agement of hallux valgus and to be cognizant of the 10 rules for proper shoe fit. 6) To be familiar with all aspects of non-surgical management of hallux valgus and associated de- formities. Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Continu- ing Medical Education by the Council on Podiatric Medical Education. You may enroll: 1) on a per issue basis (at $15 per topic) or 2) per year, for the special introductory rate of $99 (you save $51). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the near future, you may be able to submit via the Internet. If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned credits. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test at no additional cost. A list of states currently honoring CPME approved credits is listed on pg. -

Rotator Cuff and Subacromial Impingement Syndrome: Anatomy, Etiology, Screening, and Treatment
Rotator Cuff and Subacromial Impingement Syndrome: Anatomy, Etiology, Screening, and Treatment The glenohumeral joint is the most mobile joint in the human body, but this same characteristic also makes it the least stable joint.1-3 The rotator cuff is a group of muscles that are important in supporting the glenohumeral joint, essential in almost every type of shoulder movement.4 These muscles maintain dynamic joint stability which not only avoids mechanical obstruction but also increases the functional range of motion at the joint.1,2 However, dysfunction of these stabilizers often leads to a complex pattern of degeneration, rotator cuff tear arthropathy that often involves subacromial impingement.2,22 Rotator cuff tear arthropathy is strikingly prevalent and is the most common cause of shoulder pain and dysfunction.3,4 It appears to be age-dependent, affecting 9.7% of patients aged 20 years and younger and increasing to 62% of patients of 80 years and older ( P < .001); odds ratio, 15; 95% CI, 9.6-24; P < .001.4 Etiology for rotator cuff pathology varies but rotator cuff tears and tendinopathy are most common in athletes and the elderly.12 It can be the result of a traumatic event or activity-based deterioration such as from excessive use of arms overhead, but some argue that deterioration of these stabilizers is part of the natural aging process given the trend of increased deterioration even in individuals who do not regularly perform overhead activities.2,4 The factors affecting the rotator cuff and subsequent treatment are wide-ranging. The major objectives of this exposition are to describe rotator cuff anatomy, biomechanics, and subacromial impingement; expound upon diagnosis and assessment; and discuss surgical and conservative interventions. -

Saethre-Chotzen Syndrome
Saethre-Chotzen syndrome Authors: Professor L. Clauser1 and Doctor M. Galié Creation Date: June 2002 Update: July 2004 Scientific Editor: Professor Raoul CM. Hennekam 1Department of craniomaxillofacial surgery, St. Anna Hospital and University, Corso Giovecca, 203, 44100 Ferrara, Italy. [email protected] Abstract Keywords Disease name and synonyms Excluded diseases Definition Prevalence Management including treatment Etiology Diagnostic methods Genetic counseling Antenatal diagnosis Unresolved questions References Abstract Saethre-Chotzen Syndrome (SCS) is an inherited craniosynostotic condition, with both premature fusion of cranial sutures (craniostenosis) and limb abnormalities. The most common clinical features, present in more than a third of patients, consist of coronal synostosis, brachycephaly, low frontal hairline, facial asymmetry, hypertelorism, broad halluces, and clinodactyly. The estimated birth incidence is 1/25,000 to 1/50,000 but because the phenotype can be very mild, the entity is likely to be underdiagnosed. SCS is inherited as an autosomal dominant trait with a high penetrance and variable expression. The TWIST gene located at chromosome 7p21-p22, is responsible for SCS and encodes a transcription factor regulating head mesenchyme cell development during cranial tube formation. Some patients with an overlapping SCS phenotype have mutations in the FGFR3 (fibroblast growth factor receptor 3) gene; especially the Pro250Arg mutation in FGFR3 (Muenke syndrome) can resemble SCS to a great extent. Significant intrafamilial -

Non-Cardiac Manifestations of Marfan Syndrome
Keynote Lecture Series Non-cardiac manifestations of Marfan syndrome Anne H. Child Molecular and Clinical Sciences Research Institute, St George’s University of London, Cranmer Terrace, London, UK Correspondence to: Dr. Anne H. Child, MD, FRCP. Reader in Cardiovascular Genetics, Molecular and Clinical Sciences Research Institute, St George's University of London, Cranmer Terrace, London SW17 0RE, UK. Email: [email protected]. Because of the widespread distribution of fibrillin 1 in the body, Marfan syndrome (MFS) affects virtually every system. The expression of this single dominantly inherited gene is variable within a family, and between families. There is some genotype-phenotype correlation which is helpful in guiding long-term prognosis, and management. In general gene mutations have been reported in clusters, with those having mainly ocular manifestations occurring in exons 1 to 15 of this 65-exon gene; those causing cardiac problems often involving cysteine replacement in a calcium binding EGF-like sequence; the most severe mutations occurring in exons 25–32, causing neonatal MFS diagnosed at birth, and severe enough to cause death frequently before the age of 2. Other correlations will certainly be found in future. This condition is progressive, and the manifestations unfold according to age. For example, if the lens is going to dislocate this usually occurs by age 10; scoliosis usually presents itself between the ages of 8 and 15; height should be monitored carefully between the onset of puberty and cessation of growth approximately age 17 or 18. Holistic care should be offered by one doctor who oversees the patient’s welfare. This should be a paediatrician, paediatric cardiologist, or general practitioner in the case of an affected child. -

Angular Limb Deformities in Foals: Treatment and Prognosis*
Article #4 CE Angular Limb Deformities in Foals: Treatment and Prognosis* Nicolai Jansson, DVM, PhD, DECVS Skara Equine Hospital Skara, Sweden Norm G. Ducharme, DVM, MSc, DACVS Cornell University ABSTRACT: This article presents an overview of the clinical management of foals with angular limb deformities. Both conservative and surgical treatment options exist; the choice of which to use should be based on the type, severity, and location of the deformity as well as the age of the foal. Conservative measures include controlled exercise, rigid external limb support, and corrective hoof trimming. Surgical treatment modalities comprise tech- niques for manipulating physeal growth and, after physeal closure, various corrective osteotomy or ostectomy methods. The prognosis is generally good if treatment is initi- ated well in advance of physeal closure. ngular limb deformities and their treat- Conservative Treatment ment in foals and young horses constitute In most foals born with mild to moderate a significant part of the orthopedic prob- angular deformities, spontaneous resolution A 2 lems that veterinarians must manage. This article occurs within the first 2 to 4 weeks of life. In discusses the clinical management and prognosis newborn foals, periarticular laxity is the most of these postural deformities. likely cause, and these foals require no special treatment other than a short period of con- TREATMENT trolled exercise. In our opinion, mildly and The absence of controlled studies has moderately affected foals should not be confined impaired the accumulation of scientific data to a stall because exercise is important for nor- guiding the management of angular limb defor- mal muscular development and resolution of the mities in foals (Table 1). -

Rotator Cuff Tear Arthropathy: Pathophysiology, Diagnosis And
yst ar S em ul : C c u s r u r e M n t & R Orthopedic & Muscular System: c e Aydin, et al., Orthopedic Muscul Syst 2014, 3:2 i s d e e a p ISSN: 2161-0533r o c DOI: 10.4172/2161-0533-3-1000159 h h t r O Current Research Review Article Open Access Rotator Cuff Tear Arthropathy: Pathophysiology, Diagnosis and Treatment Nuri Aydin*, Okan Tok and Bariş Görgün Istanbul University Cerrahpaşa, School of Medicine, Istanbul, Turkey *Corresponding author: Nuri Aydin, Istanbul University Cerrahpaşa, School of Medicine, Orthopaedics and Traumatology, Istanbul, Turkey, Tel: +905325986232; E- mail: [email protected] Rec Date: Jan 25, 2014, Acc Date: Mar 22, 2014, Pub Date: Mar 28, 2014 Copyright: © 2014 Aydin N, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract The term rotator cuff tear arthropathy is a broad spectrum pathology but it involves common characteristic features as rotator cuff tear, leading to glenohumeral joint arthritis and superior migration of the humeral head. Although there are several factors described causing rotator cuff tear arthropathy, the exact mechanism is still unknown because the rotator cuff tear arthropathy develops in only a group of patients with chronic rotator cuff tear. The aim of this article is to review pathophysiology of rotator cuff tear arthropathy, to explain the diagnostic features and to discuss the management of the disease. Keywords: Arthropathy; Glenohumeral joint; Articular fluid Rotator cuff tear not only plays a role at the beginning of the disease, but also a developed rotator cuff tear is a result of the inflammatory Introduction process. -

CPT® Procedural Coding 110 L with Areportoftheprocedure
20610-20611 2017 Illustrated Coding and Billing Expert for Orthopedics Lower 20610-20611 ICD-9-CM Diagnostic Codes M16.7 Other unilateral secondary 711.05 Pyogenic arthritis involving pelvic osteoarthritis of hip 20610 Arthrocentesis, aspiration and/or region and thigh M17.0 Bilateral primary osteoarthritis of injection, major joint or bursa (eg, 711.06 Pyogenic arthritis involving lower leg knee shoulder, hip, knee, subacromial 713.5 Arthropathy associated with ⇄ M17.11 Unilateral primary osteoarthritis, right bursa); without ultrasound guidance neurological disorders knee 20611 Arthrocentesis, aspiration and/or 714.0 Rheumatoid arthritis ⇄ M17.12 Unilateral primary osteoarthritis, left knee injection, major joint or bursa (eg, 715.15 Osteoarthrosis, localized, primary, pelvic region and thigh M17.2 Bilateral post-traumatic osteoarthritis shoulder, hip, knee, subacromial 715.16 Osteoarthrosis, localized, primary, of knee bursa); with ultrasound guidance, with lower leg M17.5 Other unilateral secondary permanent recording and reporting 715.25 Osteoarthrosis, localized, secondary, osteoarthritis of knee (Do not report 20610, 20611 in pelvic region and thigh ⇄ M1A.051 Idiopathic chronic gout, right hip conjunction with 27370, 76942) 715.26 Osteoarthrosis, localized, secondary, ⇄ M1A.062 Idiopathic chronic gout, left knee (If fluoroscopic, CT, or MRI guidance is lower leg ⇄ M25.052 Hemarthrosis, left hip ⇄ M25.061 Hemarthrosis, right knee performed, see 77002, 77012, 77021) 715.35 Osteoarthrosis, localized, not specified whether primary -
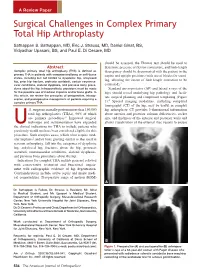
Surgical Challenges in Complex Primary Total Hip Arthroplasty
A Review Paper Surgical Challenges in Complex Primary Total Hip Arthroplasty Sathappan S. Sathappan, MD, Eric J. Strauss, MD, Daniel Ginat, BS, Vidyadhar Upasani, BS, and Paul E. Di Cesare, MD should be assessed, the Thomas test should be used to Abstract determine presence of flexion contracture, and limb-length Complex primary total hip arthroplasty (THA) is defined as discrepancy should be documented with the patient in the primary THA in patients with compromised bony or soft-tissue supine and upright positions (with use of blocks for stand- states, including but not limited to dysplastic hip, ankylosed hip, prior hip fracture, protrusio acetabuli, certain neuromus- ing, allowing the extent of limb-length correction to be 3 cular conditions, skeletal dysplasia, and previous bony proce- estimated). dures about the hip. Intraoperatively, provisions must be made Standard anteroposterior (AP) and lateral x-rays of the for the possible use of modular implants and/or bone grafts. In hips should reveal underlying hip pathology and facili- this article, we review the principles of preoperative, intraop- tate surgical planning and component templating (Figure erative, and postoperative management of patients requiring a 4 complex primary THA. 1). Special imaging modalities, including computed tomography (CT) of the hip, may be useful in complex .S. surgeons annually perform more than 150,000 hip arthroplasty. CT provides 3-dimensional information total hip arthroplasties (THAs), 90% of which about anterior and posterior column deficiencies, socket are primary procedures.1 Improved surgical size, and thickness of the anterior and posterior walls and technique and instrumentation have expanded allows visualization of the external iliac vessels to ensure Uthe clinical indications for THA to include patients who previously would not have been considered eligible for this procedure. -

Current Trends in Tendinopathy Management
Best Practice & Research Clinical Rheumatology 33 (2019) 122e140 Contents lists available at ScienceDirect Best Practice & Research Clinical Rheumatology journal homepage: www.elsevierhealth.com/berh 8 Current trends in tendinopathy management * Tanusha B. Cardoso a, , Tania Pizzari b, Rita Kinsella b, Danielle Hope c, Jill L. Cook b a The Alphington Sports Medicine Clinic, 339 Heidelberg Road, Northcote, Victoria, 3070, Australia b La Trobe University Sport and Exercise Medicine Research Centre, La Trobe University, Corner of Plenty Road and Kingsbury Drive, Bundoora, Victoria, 3083, Australia c MP Sports Physicians, Frankston Clinic, Suite 1, 20 Clarendon Street, Frankston, Victoria, 3199, Australia abstract Keywords: Tendinopathy Tendinopathy (pain and dysfunction in a tendon) is a prevalent Management clinical musculoskeletal presentation across the age spectrum, Rehabilitation mostly in active and sporting people. Excess load above the ten- Achilles tendinopathy don's usual capacity is the primary cause of clinical presentation. Rotator cuff tendinopathy The propensity towards chronicity and the extended times for recovery and optimal function and the challenge of managing tendinopathy in a sporting competition season make this a difficult condition to treat. Tendinopathy is a heterogeneous condition in terms of its pathology and clinical presentation. Despite ongoing research, there is no consensus on tendon pathoetiology and the complex relationship between tendon pathology, pain and func- tion is incompletely understood. The diagnosis of tendinopathy is primarily clinical, with imaging only useful in special circum- stances. There has been a surge of tendinopathy treatments, most of which are poorly supported and warrant further exploration. The evidence supports a slowly progressive loading program, rather than complete rest, with other treatment modalities used as adjuncts mainly targeted at achieving pain relief.