Effectiveness of an Integrated Care Package for Refugee Mothers and Children: Protocol for a Cluster Randomized Controlled Trial
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Remaking Rakhine State
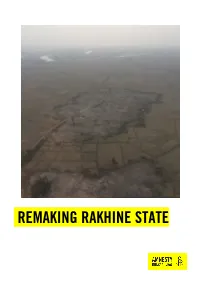
REMAKING RAKHINE STATE Amnesty International is a global movement of more than 7 million people who campaign for a world where human rights are enjoyed by all. Our vision is for every person to enjoy all the rights enshrined in the Universal Declaration of Human Rights and other international human rights standards. We are independent of any government, political ideology, economic interest or religion and are funded mainly by our membership and public donations. © Amnesty International 2017 Except where otherwise noted, content in this document is licensed under a Creative Commons Cover photo: Aerial photograph showing the clearance of a burnt village in northern Rakhine State (attribution, non-commercial, no derivatives, international 4.0) licence. © Private https://creativecommons.org/licenses/by-nc-nd/4.0/legalcode For more information please visit the permissions page on our website: www.amnesty.org Where material is attributed to a copyright owner other than Amnesty International this material is not subject to the Creative Commons licence. First published in 2017 by Amnesty International Ltd Peter Benenson House, 1 Easton Street London WC1X 0DW, UK Index: ASA 16/8018/2018 Original language: English amnesty.org INTRODUCTION Six months after the start of a brutal military campaign which forced hundreds of thousands of Rohingya women, men and children from their homes and left hundreds of Rohingya villages burned the ground, Myanmar’s authorities are remaking northern Rakhine State in their absence.1 Since October 2017, but in particular since the start of 2018, Myanmar’s authorities have embarked on a major operation to clear burned villages and to build new homes, security force bases and infrastructure in the region. -

Download File
UNICEF ADVOCACY ALERT | August 2019 UNICEF ADVOCACY ALERT | August 2019 BEYOND SURVIVAL SURVIVAL ROHINGYA REFUGEE ROHINGYACHILDREN REFUGEE IN BANGLADESH CHILDREN IN BANGLADESH WANT TO LEARN WANT TO LEARN UNICEF Bangladesh thanks its partners and donors without whom its work on behalf of Rohingya children would not be possible Cover photo: Children at a UNICEF-supported Learning Centre in Kutupalong refugee camp © UNICEF/Brown Published by UNICEF Bangladesh BSL Offi ce Complex, 1 Minto Road, Dhaka – 1000, Bangladesh © United Nations Children’s Fund (UNICEF) August 2019 #AChildisAChild BEYOND SURVIVAL ROHINGYA REFUGEE CHILDREN IN BANGLADESH WANT TO LEARN Refugee Population in Cox’s Bazar District April 2019 | Sources: ISCG, RRRC, UNHCR, IOM-NPM, Site Management Sector | Projection: BUTM CONTENTS 4 BEYOND SURVIVAL 6 Frustration in a fragile setting 8 DESPERATE TO LEARN 10 First steps towards quality learning 12 Big issues remain 14 Adolescents risk missing out 18 A CLARION CALL FOR EDUCATION 20 MEETING THE NEEDS OF ROHINGYA REFUGEE CHILDREN 22 Building bridges between the communities 24 Darkness exposes women and girls to danger 27 At the mercy of traffi ckers 30 Vigilance against the threat of cholera 32 Youngest children remain at risk 34 Piped networks give more families access to safe water 38 CALL TO ACTION 42 UNICEF BANGLADESH ROHINGYA RESPONSE HIGHLIGHTS 2017-19 43 UNICEF FUNDING NEEDS 2019 Monsoon rainclouds loom overhead as Mohamed Amin (facing camera centre) and other family members rebuild their shelter which was destroyed during heavy monsoon rains on the night of July 6 2019. In the space of 25 days in July, authorities in the vast Rohingya camps had to assist over 5,700 refugee households with damaged shelters. -

Rohingya Refugee Crisis and Forest Cover Change in Teknaf, Bangladesh
remote sensing Article Rohingya Refugee Crisis and Forest Cover Change in Teknaf, Bangladesh Mohammad Mehedy Hassan 1,*, Audrey Culver Smith 1, Katherine Walker 1 ID , Munshi Khaledur Rahman 2 and Jane Southworth 1 1 Department of Geography, University of Florida, 3141 Turlington Hall, P.O. Box 117315, Gainesville, FL 32611-7315, USA; audreyculver@ufl.edu (A.C.S.); kqwalker@ufl.edu (K.W.); jsouthwo@ufl.edu (J.S.) 2 Department of Geography, Virginia Tech, 115 Major Williams Hall, 220 Stanger Street, Blacksburg, VA 24061, USA; [email protected] * Correspondence: mehedy@ufl.edu; Tel.: +1-352-745-9364 Received: 6 March 2018; Accepted: 25 April 2018; Published: 30 April 2018 Abstract: Following a targeted campaign of violence by Myanmar military, police, and local militias, more than half a million Rohingya refugees have fled to neighboring Bangladesh since August 2017, joining thousands of others living in overcrowded settlement camps in Teknaf. To accommodate this mass influx of refugees, forestland is razed to build spontaneous settlements, resulting in an enormous threat to wildlife habitats, biodiversity, and entire ecosystems in the region. Although reports indicate that this rapid and vast expansion of refugee camps in Teknaf is causing large scale environmental destruction and degradation of forestlands, no study to date has quantified the camp expansion extent or forest cover loss. Using remotely sensed Sentinel-2A and -2B imagery and a random forest (RF) machine learning algorithm with ground observation data, we quantified the territorial expansion of refugee settlements and resulting degradation of the ecological resources surrounding the three largest concentrations of refugee camps—Kutupalong–Balukhali, Nayapara–Leda and Unchiprang—that developed between pre- and post-August of 2017. -

FOREWORD in 2017, Asia and the Pacific Was Home to More Than 60 Per Cent of the World’S Population
REGIONAL SUMMARIES FOREWORD In 2017, Asia and the Pacific was home to more than 60 per cent of the world’s population. With some 4.4 billion people, the region is an engine for global development, characterized by economic growth, rising living standards, and people on the move seeking new opportunities. However, in 2017, millions of people were not following this upward trajectory. The region hosted 9.5 million people of concern to UNHCR, including 4.2 million refugees, 2.7 million IDPs, and an estimated 2.2 million stateless persons. Of the total population of concern to UNHCR, half were children; more than half were women and girls; and many had no nationality, documentation or place to call home. The long-standing tradition of hospitality towards many displaced people remained strong across the region. This was demonstrated by the remarkable response of Bangladesh, which kept its borders open to nearly 655,000 stateless refugees fleeing violence in Myanmar. The influx dramatically altered the operational context for UNHCR in Bangladesh. As a result of the urgent humanitarian needs, UNHCR ramped up its capacity in support of refugees, the Government and local communities generously hosting them. The solutions to this crisis lie in Myanmar, and it is there that the search must start for them. The efforts needed to enable the voluntary and sustainable repatriation of refugees failed to materialize in 2017, and they must begin with humanitarian access for UNHCR. Preserving the right of return, however, remained a central priority for UNHCR and Asia and the Office welcomed the commitments made by Bangladesh and Myanmar on dignified, safe, and voluntary repatriation in 2017. -

Weekly Situation Report 3
Weekly Situation Report # 2 Date of issue: 8 November 2017 Period covered: 1 to 7 November 2017 Location: Bangladesh Emergency type: Arrival of Rohingya population from Myanmar following conflict in Rakhine state 609 000 300 000 105 1727 1.2 million new arrivals refugees from Myanmar children over 1 year of age people targeted for in Bangladesh who arrived previously vaccinated with oral cholera humanitarian assistance in B angladesh vaccine (58% of target at end of day 3 of 6-day campaign) KEY HIGHLIGHTS As of 6 November 2017, the cumulative number of new arrivals in all sites (Ukiah, Teknaf, Cox’s Bazar and Ramu) was 609 0001. This number includes over 329 000 arrivals in Kutupalong Balukhali expansion site, 230 000 in other camps and settlements, and 46 000 arrivals in host communities. According to data generated by WHO’s disease early warning and response system (EWARS), a total of 245 389 consultations were provided to the new arrivals and other vulnerable populations between 25 August to 4 November 2017. A total of 412 suspected cases of measles have been reported through EWARS. Case investigation/finding is ongoing. The preliminary results of a recent inter-agency assessment conducted in Kutupalong refugee camp from 22 to 28 October 2017 shows that severe acute malnutrition rates are running at 7.5% (well above emergency thresholds). The second phase of an oral cholera vaccination campaign started on 4 November. Around 180 000 children aged between one and five years will be given a second dose of oral cholera vaccine for added protection, and 210 000 children under five years of age will be given oral polio vaccine (bOPV). -

Persecution of the Rohingya Muslims
OCTOBER 2015 PERSECUTION OF THE ROHINGYA MUSLIMS: IS GENOCIDE OCCURRING IN MYANMAR’S RAKHINE STATE? A LEGAL ANALYSIS PREPARED FOR FORTIFY RIGHTS ALLARD K. LOWENSTEIN INTERNATIONAL HUMAN RIGHTS CLINIC, YALE LAW SCHOOL OCTOBER 2015 PERSECUTION OF THE ROHINGYA MUSLIMS: IS GENOCIDE OCCURRING IN MYANMAR’S RAKHINE STATE? A LEGAL ANALYSIS Prepared by the ALLARD K. LOWENSTEIN INTERNATIONAL HUMAN RIGHTS CLINIC, YALE LAW SCHOOL for FORTIFY RIGHTS ACKNOWLEDGMENTS This paper was written by Alina Lindblom, Elizabeth Marsh, Tasnim Motala, and Katherine Munyan of the Allard K. Lowenstein International Human Rights Clinic at Yale Law School. The team was supervised and the paper edited by Professor James Silk, director of the Lowenstein Clinic, and Soo-Ryun Kwon, formerly the Robert M. Cover - Allard K. Lowenstein Fellow in International Human Rights at Yale Law School. Former clinic member Veronica Jordan-Davis contributed to the initial research for the paper. The team would like to thank the students in the Fall 2015 Lowenstein Clinic for helping to check the paper’s citations. CONTENTS I. SUMMARY ................................................................................................ 1 II. METHODOLOGY ......................................................................................4 III. HISTORY OF HUMAN RIGHTS ABUSES AGAINST ROHINGYA IN MYANMAR ...........................................................................................5 A. ROHINGYA UNDER MILITARY RULE: FROM MYANMAR’S INDEPENDENCE THR OUGH 2011 ..............................................................5 -

Coronavirus Closes in on Rohingya Refugees in Bangladesh's
Boise State University ScholarWorks University Author Recognition Bibliography: 2020 The Albertsons Library 4-20-2020 Coronavirus Closes in on Rohingya Refugees in Bangladesh’s Cramped, Unprepared Camps Saleh Ahmed Boise State University Academic rigor, journalistic flair Nary a mask in sight at a market area in Bangladesh’s Kutupalong refugee camp for Rohingya, Ukhia, March 24, 2020. Suzauddin Rubel/AFP via Getty Images Coronavirus closes in on Rohingya refugees in Bangladesh’s cramped, unprepared camps April 20, 2020 2.05pm EDT Coronavirus is spreading quickly in densely populated Bangladesh, despite a Author nationwide shutdown put in place a month ago. This preventive measure has proven challenging to implement due to lack of awareness of the coronavirus and the absence of a social safety net. Extreme poverty Saleh Ahmed also forces many Bangladeshis to keep working and looking for food despite the risks. Assistant Professor, School of Public Bangladesh had 2,948 confirmed COVID-19 cases as of April 20. Service, Boise State University The disease has not yet spread into the refugee camps that house the Rohingya Muslims who fled ethnic violence in Myanmar in 2017, according to a recent update from the humanitarian organizations that work in the camps. But an outbreak in the overcrowded camps is almost certain to come eventually – and when it does, experts say, the damage could be severe. Crisis response in the camps Even in normal times people in refugee camps often struggle to survive, living as they do with minimal resources, food and housing. I saw this grim reality with my own eyes when I visited the Rohingya refugee camps in Bangladesh – my home country – in 2017 and 2018. -

Developments
Highlights: Camp Conditions: • The Bhashan Char housing project is complete and ready to accommodate 1-lakh Rohingya refugees, but the relocation is uncertain after Bangladesh authorities failed to gain support for the plan from UN agencies. High-level Statements: • UN Secretary General António Guterres said Myanmar was responsible for ensuring a conducive environment for the safe, voluntary and dignified return of Rohingya refugees currently residing in Bangladesh. • Responding to the UN Secretary General’s remarks on the Rohingya issue, State Counselor Aung San Suu Kyi said the Myanmar government will not shirk from its responsibility and reaffirmed that the country will work with friends who approach the issue in a “practical and balanced way.” Accountability: • Rohingya victims from the village of Tula Toli have submitted a victim statement to the ICC, requesting the case be allowed forward. Developments: On Rohingya, Myanmar Will Not Shrink From Responsibility: Suu Kyi, The Irrawaddy (Nov. 4) Responding to the UN Secretary General’s remarks on the Rohingya issue, State Counselor Daw Aung San Suu Kyi said the Myanmar government will not shirk from its responsibility and reaffirmed that the country will work with friends who approach the issue in a “practical and balanced way.” She added that the Myanmar government was fully committed to taking back verified returnees based on the bilateral agreement signed with Bangladesh and the trilateral agreement signed with the UNHCR and UNDP. She also expressed her appreciation to ASEAN, the ASEAN Secretariat and the ASEAN Coordinating Center for Humanitarian Assistance on Disaster Management for their assistance on the issue. It’s needed in regional interests, The Daily Star (November 4) A speedy, safe and sustainable return of the Rohingya refugees sheltered in Bangladesh is in the interest of the region, Indian Prime Minister Narendra Modi said when he met Myanmar State Counsellor Aung San Suu Kyi. -
The Impact of Covid-19 on Global Migration
THE IMPACT OF COVID-19 ON GLOBAL MIGRATION Nasar Meer and Leslie Villegas University of Edinburgh 27 May 2020 This working paper is part of the Governance of the Local Integration of Migrants and Europe’s Refugees (GLIMER) which has received funding in the framework of the Joint Programming Initiative Urban Europe, with support from the European Union’s Horizon 2020 Research and Innovation Programme under grant agreement No 693443. Table of Contents Introduction and Overview ......................................................................................................... 2 Temporarily Reintroduced Border Controls ............................................................................. 4 Travel restrictions by the numbers ................................................................................................. 4 European Union Policy and Guidance ............................................................................................. 5 Asylum, refugee, and immigrant protections during the COVID-19 pandemic ................... 6 Evidence of Impact .............................................................................................................................. 7 Access to Asylum ................................................................................................................................................. 7 Refugee camps and other humanitarian response areas .................................................................................... 11 Domestic issues affecting displaced and -

The Rohingya Genocide and the Consequent Influx of Refugees Into Bangladesh and Find Ways to Solve Its Problems
ISSN (Online): 2350-0530 International Journal of Research -GRANTHAALAYAH ISSN (Print): 2394-3629 October 2020, Vol 8(10), 131 – 137 DOI: https://doi.org/10.29121/granthaalayah.v8.i10.2020.1882 THE ROHINGYA GENOCIDE AND THE CONSEQUENT INFLUX OF REFUGEES INTO BANGLADESH AND FIND WAYS TO SOLVE ITS PROBLEMS Sanjib Sardar *1 *1 Research Scholar, Sri Satya Sai University of Technology and Medical Sciences, Madhya Pradesh, India DOI: https://doi.org/10.29121/granthaalayah.v8.i10.2020.1882 Article Type: Research Article ABSTRACT Rohingya is the name of a persecuted and oppressed nation of the Article Citation: Sanjib Sardar. world. Ethnic genocide against the Rohingya is not a new issue, the planned (2020). THE ROHINGYA GENOCIDE attack by the Burmese army on the Rohingya dates back to the 1960s. As a AND THE CONSEQUENT INFLUX OF result of a new level of attack on August 25, 2017, about seven to eight lakh REFUGEES INTO BANGLADESH AND FIND WAYS TO SOLVE ITS Rohingya refugees have been forced to flee in Bangladesh. Rohingyas have PROBLEMS. International Journal of also been subjected to genocide, rape, torture and attacks from a section of Research -GRANTHAALAYAH, Buddhist society in Myanmar. The main purposes of this study are to find 8(10), 131-137. out the causes of Rohingya genocide and the consequent influx of refugees https://doi.org/10.29121/granthaa into Bangladesh. The present study is based on intensive analysis of layah.v8.i10.2020.1882 secondary data. The sources of secondary data are books, journals etc. It focuses on the Rohingya citizenship issue in Myanmar, its root causes, the Received Date: 01 October 2020 persecution of the Rohingya and their socio-economic conditions. -

Projecting the Impact in Rohingya Refugee Camps and Beyond
Novel Coronavirus: Projecting the impact in Rohingya refugee camps and beyond March 18, 2020 Aerial view of Kutupalong camp 4 extension, UNHCR, July 2, 2018 Authors: Shaun Truelove PhD MPH1,2,3 Orit Abrahim MPH1,3 Chiara Altare MPH PhD 1,3 Andrew Azman PhD MHS 1,2,3 Paul Spiegel MD MPH 1,3 1 Johns Hopkins Bloomberg School of Public Health 2 Infectious Disease Dynamics 3 Center for Humanitarian Health 1 | Page Executive Summary Background There are over 200,000 confirmed cases of COVID-19, the infection caused by the newly emerged severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), globally. Forcibly displaced populations, especially those who reside in settlements with high density, poor access to water and sanitation, and limited health services, are especially vulnerable to a serious outbreak. Bangladesh, where 10 confirmed cases of COVID-19 have been confirmed, hosts almost 1 million Rohingya refugees from Myanmar in Cox’s Bazar district. Of these, approximately 600,000 refugees are concentrated in the Kutupalong- Balukhali Expansion Site. The capacity to meet the existing health needs of this population are already limited. An outbreak of COVID-19 within this population threatens to severely disrupt an already fragile situation. Methods To explore the potential impact of SARS-CoV-2 virus on the Rohingya refugees in the Kutupalong- Balukhali expansion site, we used a scenario-based approach to model transmission in this population after an introduction of the virus. Using three different assumptions about the transmission potential of SARS-CoV-2 at this site, we estimated the number of infections, hospitalizations, deaths, and health care needs that might be expected. -

Video Transcript- Fact-Finding Mission on Myanmar (FFMM
-Video Transcript- Fact-finding Mission on Myanmar (FFMM) Footage from Kutupalong refugee camp, Cox’s Bazar, Bangladesh 17 and 18 July 2018 00:00-00:12 Christopher Sidoti, member of the FFMM (Australia): The numbers that were involved last year, the intensity over such a short space of time is certainly unique in the history of Myanmar, but it’s not unique in terms of the experience of so many other ethnic minorities. 00:13-00:19 Cutaways inside Kutupalong refugee camp 00:20-00:29 C. Sidoti: The simple fact is that human rights violations are widespread and that much of what has happened to the Rohingya has been experienced as well by other ethnic minorities. 00:29-00:35 Cutaways inside Kutupalong refugee camp 00:36-00:50 C. Sidoti: Myanmar cries out for a total solution: one that embraces the whole country and doesn’t just seek to address the problems of any individual minority group. And that’s the case because the whole country is in human rights crisis. 00:51-00:57 Cutaways inside Kutupalong refugee camp 00:58-01:13 C. Sidoti: Part of the solution is justice; ensuring that those who are responsible for what has happened to them, and to so many others in Myanmar, are brought to justice and held accountable for their actions. This is one of the most important tasks facing the fact-finding mission. 01:14-01:20 Cutaways inside Kutupalong refugee camp 01:21-02:18 Radhika Coomaraswamy, member of the FFMM (Sri Lanka): The Rohingya population had been driven out in 1992, in the 1980s and the 70s; they were just driven out.