Introduction Urban Reproductive Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Informal Microfinance and Economic Activities of Rural Dwellers in Kwara South Senatorial District of Nigeria
International Journal of Business and Social Science Vol. 2 No. 15; August 2011 INFORMAL MICROFINANCE AND ECONOMIC ACTIVITIES OF RURAL DWELLERS IN KWARA SOUTH SENATORIAL DISTRICT OF NIGERIA IJAIYA, Muftau Adeniyi Department of Accounting and Finance University of Ilorin, Ilorin, Nigeria E-mail : [email protected], Phone: +2348036973561 Abstract Rural areas, like urban areas have increasing demand for credit because such credit reduces the impact of seasonality on incomes. However, formal financial institutions have maintained low presence in the rural areas. This has affected the rural dwellers’ access to deposit savings and credits that can improve their economic activities. This study examined the influence of informal microfinance on economic activities of rural dwellers in the selected rural areas of Kwara South Senatorial District. Using a multiple regression analysis, six hundred (600) questionnaire was administered on members of informal microfinance institution in the study area, the study found that fund provided as credit facilities for transaction purposes, funds for housing and combating diseases have significant influence on the economic activities of the rural areas. The study recommends group savings and group lending in order to increase savings and credits to the rural dwellers. Government should also provide improved infrastructural facilities that would enable rural dwellers have more access to their economic activities Key Words: Microfinance, Informal, Economic Activities, Rural, Kwara 1.0 Introduction Africa‟s development challenges go deeper than low income, falling trade shares, low savings and slow growth. They also include inequality and uneven access to productive resources, social exclusion and insecurity especially among the women (Pitamber, 2003). However, more specific concern is raised in Nigeria due to rural-urban disparities in income distribution, access to education and health care services, and prevalence of ethnic or cross-boundary conflicts. -

Geotechnical Investigation of Road Failure Along Ilorin-Ajase – Ipo Road Kwara State, Nigeria
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by International Institute for Science, Technology and Education (IISTE): E-Journals Journal of Environment and Earth Science www.iiste.org ISSN 2224-3216 (Paper) ISSN 2225-0948 (Online) Vol. 3, No.7, 2013 Geotechnical Investigation of Road Failure along Ilorin-Ajase – Ipo Road Kwara State, Nigeria. Dr. I.P. Ifabiyi [email protected] Department of Geography and Environmental Management Faculty of Business and Social Science P.M.B 1515, University Of Ilorin, Ilorin. Kwara State, Nigeria. Mr. Kekere, A.A [email protected] Department of Art and Social Science, Unilorin Secondary School, University Of Ilorin, Ilorin, Nigeria. Abstract The incessant failure of road network in Nigeria has generated a lot of concern by road users and government. Apart from lives and properties that are lost annually to road crashes, road rehabilitation across the country has become a financial burden to the federal government. Several factors have been identified to be responsible to road failure in Nigeria; they include geological, geomorphological, road usage, bad construction and wrong approach to maintenance. Hence, this paper examines some of the factors responsible for road failure along Ilorin-Ajase Ipo road, Kwara State Nigeria. Soil samples were collected from Five (5) portions of the road that are badly affected by road failure. These portions include: Agricultural and Rural Management Training Institute (ARMTI) 17+800km, Kabba Owode 18+00Km, Idofian 23+700Km, Koko 29+700Km and Omupo 35+700Km axis. The soil samples collected were analyzed four engineering properties: particle size distribution (PSD),atterberg limit, compaction test California Bearing Ratio (CBR). -

05 Onyango-Ouma
HEALTH POLICY AND PLANNING; 16(Suppl. 1): 24–32 © Oxford University Press 2001 An evaluation of Health Workers for Change in seven settings: a useful management and health system development tool WASHINGTON ONYANGO-OUMA,1 ROSE LAISSER,2 MUSIBA MBILIMA,3 MARGARET ARAOYE,4 PATRICIA PITTMAN,5 IRENE AGYEPONG,6 MAIRO ZAKARI,7 SHARON FONN,8 MARCEL TANNER9 AND CAROL VLASSOFF10 1KEDAHR Project, Division of Vector-Borne Diseases, Ministry of Health, Kisumu, Kenya, 2Institute of Allied Health Sciences, School of Nursing, Dar es Salaam, Tanzania, 3University Health Centre, Dar es Salaam, Tanzania, 4Department of Epidemiology and Community Health, University of Ilorin, Nigeria, 5Women, Health and Development Program, Division of Health and Human Development, Pan American Health Organization, Washington, DC, 6Ministry of Health, Dangme West Health Research Centre, Dodowa, Ghana, 7Entomology and Parasitology Division, National Institute for Trypanosomiasis Research, Kadua, Nigeria, 8Women’s Health Project, Department of Community Health. University of the Witwatersrand, Johannesburg, South Africa, 9Swiss Tropical Institute, Basel, Switzerland and 10Canadian International Development Agency, Hull, Quebec, Canada This paper presents the findings of a multi-centre study assessing the impact of Health Workers for Change (HWFC) workshops in seven different primary care sites, based on the common core protocol described in this paper. The paper discusses a common methodology used by the studies, consisting of a triangulation of qualitative and quantitative methods. Such methodologies are inherently complex as they require com- parisons across systems, sites and procedures. The studies were conducted in six sites in Africa and one site in Argentina. Generally, the intervention resulted either in positive change or in no change, except in the area of staff relationships where conflicts were more frequent after the intervention than before. -

Mannitol Dosing Error During Pre-Neurosurgical Care of Head Injury: a Neurosurgical In-Hospital Survey from Ibadan, Nigeria
Published online: 2021-01-29 THIEME Original Article 171 Mannitol Dosing Error during Pre-neurosurgical Care of Head Injury: A Neurosurgical In-Hospital Survey from Ibadan, Nigeria Amos Olufemi Adeleye1,2 Toyin Ayofe Oyemolade2 Toluyemi Adefolarin Malomo2 Oghenekevwe Efe Okere2 1Department of Surgery, Division of Neurological Surgery, College Address for correspondence Amos Olufemi Adeleye, MBBS, of Medicine, University of Ibadan, Ibadan, Nigeria Department of Neurological Surgery, University College Hospital, 2Department of Neurological Surgery, University College Hospital, UCH, Ibadan, Owo, PMB 1053, Nigeria Ibadan, Nigeria (e-mail: [email protected]). J Neurosci Rural Pract:2021;12:171–176 Abstract Objectives Inappropriate use of mannitol is a medical error seen frequently in pre-neurosurgical head injury (HI) care that may result in serious adverse effects. This study explored this medical error amongst HI patients in a Nigerian neurosurgery unit. Methods We performed a cross-sectional analysis of a prospective cohort of HI patients who were administered mannitol by their initial non-neurosurgical health care givers before referral to our center over a 22-month period. Statistical Analysis A statistical software was used for the analysis with which an α value of <0.05 was deemed clinically significant. Results Seventy-one patients were recruited: 17 (23.9%) from private hospitals, 13 (18.3%) from primary health facilities (PHFs), 20 (28.2%) from secondary health facilities (SHFs), and 21 (29.6%) from tertiary health facilities (THFs). Thirteen patients (18.3%) had mild HI; 29 (40.8%) each had moderate and severe HI, respectively. Pupillary abnormalities were documented in five patients (7.04%) with severe HI and neurological deterioration in two with mild HI. -

S/No Placement 1
S/NO PLACEMENT ADO - ODO/OTA LOCAL GOVERNMENT SECRETARIAT, SANGO - OTA, OGUN 1 STATE AGEGE LOCAL GOVERNMENT, BALOGUN STREET, MATERNITY, SANGO, 2 AGEGE, LAGOS STATE 3 AHMAD AL-IMAM NIG. LTD., NO 27, ZULU GAMBARI RD., ILORIN 4 AKTEM TECHNOLOGY, ILORIN, KWARA STATE 5 ALLAMIT NIG. LTD., IBADAN, OYO STATE 6 AMOULA VENTURES LTD., IKEJA, LAGOS STATE CALVERTON HELICOPTERS, 2, PRINCE KAYODE, AKINGBADE CLOSE, 7 VICTORIA ISLAND, LAGOS STATE CHI-FARM LTD., KM 20, IBADAN/LAGOS EXPRESSWAY, AJANLA, IBADAN, 8 OYO STATE CHINA CIVIL ENGINEERING CONSTRUCTION CORPORATION (CCECC), KM 3, 9 ABEOKUTA/LAGOS EXPRESSWAY, OLOMO - ORE, OGUN STATE COCOA RESEARCH INSTITUTE OF NIGERIA (CRIN), KM 14, IJEBU ODE ROAD, 10 IDI - AYANRE, IBADAN, OYO STATE COKER AGUDA LOCAL COUNCIL, 19/29, THOMAS ANIMASAUN STREET, 11 AGUDA, SURULERE, LAGOS STATE CYBERSPACE NETWORK LTD.,33 SAKA TIINUBU STREET. VICTORIA ISLAND, 12 LAGOS STATE DE KOOLAR NIGERIA LTD.,PLOT 14, HAKEEM BALOGUN STREET, OPP. 13 TECHNICAL COLLEGE, AGIDINGBI, IKEJA, LAGOS STATE DEPARTMENT OF PETROLEUM RESOURCES, 11, NUPE ROAD, OFF AHMAN 14 PATEGI ROAD, G.R.A, ILORIN, KWARA STATE DOLIGERIA BIOSYSTEMS NIGERIA LTD, 1, AFFAN COMPLEX, 1, OLD JEBBA 15 ROAD, ILORIN, KWARA STATE ESFOOS STEEL CONSTRUCTION COMPANY, OPP. SDP, OLD IFE ROAD, 16 AKINFENWA, EGBEDA, IBADAN, OYO STATE 17 FABIS FARMS NIGERIA LTD., ILORIN, KWARA STATE FEDERAL AIRPORT AUTHORITY, MURTALA MOHAMMED AIRPORT, IKEJA, 18 LAGOS STATE FEDERAL INSTITUTE OF INDUSTRIAL RESEARCH OSHODI (FIIRO), 3, FIIRO 19 ROAD, OFF CAPPA BUS STOP, AGEGE MOTOR ROAD, OSHODI, LAGOS FEDERAL MINISTRY OF AGRICULTURE & RURAL DEVELOPMENT, FOOD & STRATEGIC GRAINS RESERVE DEPARTMENT (FRSD) SILO COMPLEX, KWANA 20 WAYA, YOLA, ADAMAWA STATE 21 FRESH COUNTRY CHICKEN ENTERPRISES, SHONGA, KWARA STATE 22 GOLDEN PENNY FLOUR MILLLS, APAPA WHARF, APAPA, LAGOS STATE HURLAG TECHNOLOGIES, 7, LADIPO OLUWOLE STREET, OFF ADENIYI JONES 23 AVENUE, IKEJA, LAGOS STATE 24 IBN DEND, FARM, KM. -

Muslims of Kwara State: a Survey
Nigeria Research Network (NRN) Oxford Department of International Development Queen Elizabeth House University of Oxford NRN BACKGROUND PAPER NO. 3 Muslims of Kwara State: A Survey Abdulganiy Abimbola Abdussalam* January 2012 Acknowledgements The author gratefully acknowledges financial support from the Islam Research Programme - Abuja, funded by the Ministry of Foreign Affairs of the Kingdom of the Netherlands. The views presented in this paper represent those of the author and are in no way attributable to the Ministry. * Dr Abdulganiy Abimbola Abdussalam obtained his Ph.D. in Arabic Linguistics at the University of Ilorin, in 2003, with a dissertation entitled An Analytical Study of Arabic Works of Ulama in Yorubaland of Nigeria. He is senior lecturer in the Department of Languages and Linguistics, Nasarawa State University, Keffi. NRN Background Paper 3 Abstract The paper begins with an overview of Kwara State, then proceeds to a brief discussion of categories of Muslims in the state, with estimates of percentages of Muslims in various categories. There follow discussions of Islamic education in the state, and of Muslims and Islam in politics and government. The last two substantive sections discuss Muslim NGOs, with details on four groups, and then three notable Muslim personages active in the state, and the paper ends with a brief conclusion. Table of Contents 1. Overview 3 2. Categories of Muslims 3 a. Estimated percentages belonging to various groups 3 b. Relations among the various groups of Muslims 3 3. Islamic education 4 a. Qur’anic education 4 b. Islamiyya schools 4 c. Tertiary Islamic education 4 i. Private 4 ii. -

(IITA) Oyo Road, PMB 5320 Ibadan, Nigeria Regional Cocoa Symposium
TRAVEL ADVICE International Institute of Tropical Agriculture (IITA) Oyo Road, PMB 5320 Ibadan, Nigeria Regional Cocoa Symposium Contact at IITA: [email protected] CRIN contact: [email protected] WCF contact: [email protected] Before departure You need a valid passport, a visa (depending on your nationality), and a health certificate verifying an up-to-date yellow fever inoculation1. Citizens of countries belonging to the Economic Community of West African States (ECOWAS) are exempted from the visa requirement. Kindly be aware that Ibadan is located in the Humid Tropics and that malaria is endemic in the area. It is advised to dress accordingly and take doctor’s advice before traveling. Obtaining a Nigerian Visa Applications for visas can be made at any Nigerian Embassy, Consulate, or High Commission in your country of residence or the nearest to you. The website https://portal.immigration.gov.ng/visa/freshVisa can give you more information. The application process may be time consuming. IITA will generate an invitation and visa support letter that will accompany your request. It is also possible to arrange for a visa on arrival if you reside in a country where Nigeria has no legal representation; please contact us for that one. You cannot buy a visa at the airport on arrival! Arriving at Lagos Airport Murtala Mohammed International Airport, Ikeja, is the port of disembarkation. Representatives from IITA will meet you after the baggage collection area to take you to the IITA vehicles. Airport assistance is also available (on request) to take you through immigration, customs and checking-in at a cost of USD 40 including arrival and departures. -

An Estimated Dynamic Model of African Agricultural Storage and Trade
High Trade Costs and Their Consequences: An Estimated Dynamic Model of African Agricultural Storage and Trade Obie Porteous Online Appendix A1 Data: Market Selection Table A1, which begins on the next page, includes two lists of markets by country and town population (in thousands). Population data is from the most recent available national censuses as reported in various online databases (e.g. citypopulation.de) and should be taken as approximate as census years vary by country. The \ideal" list starts with the 178 towns with a population of at least 100,000 that are at least 200 kilometers apart1 (plain font). When two towns of over 100,000 population are closer than 200 kilometers the larger is chosen. An additional 85 towns (italics) on this list are either located at important transport hubs (road junctions or ports) or are additional major towns in countries with high initial population-to-market ratios. The \actual" list is my final network of 230 markets. This includes 218 of the 263 markets on my ideal list for which I was able to obtain price data (plain font) as well as an additional 12 markets with price data which are located close to 12 of the missing markets and which I therefore use as substitutes (italics). Table A2, which follows table A1, shows the population-to-market ratios by country for the two sets of markets. In the ideal list of markets, only Nigeria and Ethiopia | the two most populous countries | have population-to-market ratios above 4 million. In the final network, the three countries with more than two missing markets (Angola, Cameroon, and Uganda) are the only ones besides Nigeria and Ethiopia that are significantly above this threshold. -

Ibadan, Nigeria by Laurent Fourchard
The case of Ibadan, Nigeria by Laurent Fourchard Contact: Source: CIA factbook Laurent Fourchard Institut Francais de Recherche en Afrique (IFRA), University of Ibadan Po Box 21540, Oyo State, Nigeria E-mail: [email protected] [email protected] INTRODUCTION: THE CITY A. URBAN CONTEXT 1. Overview of Nigeria: Economic and Social Trends in the 20th Century During the colonial period (end of the 19th century – agricultural sectors. The contribution of agriculture to 1960), the Nigerian economy depended mainly on agri- the Gross Domestic Product (GDP) fell from 60 percent cultural exports and on proceeds from the mining indus- in the 1960s to 31 percent by the early 1980s. try. Small-holder peasant farmers were responsible for Agricultural production declined because of inexpen- the production of cocoa, coffee, rubber and timber in the sive imports and heavy demand for construction labour Western Region, palm produce in the Eastern Region encouraged the migration of farm workers to towns and and cotton, groundnut, hides and skins in the Northern cities. Region. The major minerals were tin and columbite from From being a major agricultural net exporter in the the central plateau and from the Eastern Highlands. In 1960s and largely self-sufficient in food, Nigeria the decade after independence, Nigeria pursued a became a net importer of agricultural commodities. deliberate policy of import-substitution industrialisation, When oil revenues fell in 1982, the economy was left which led to the establishment of many light industries, with an unsustainable import and capital-intensive such as food processing, textiles and fabrication of production structure; and the national budget was dras- metal and plastic wares. -

Effect of Membership of Group-Farming Cooperatives on Farmers Food Production and Poverty Status in Nigeria
Effect of Membership of Group-Farming Cooperatives on Farmers Food Production and Poverty Status in Nigeria A. Adekunle; University of Ilorin, Agricultural Economics and Farm Management, Nigeria Corresponding author email: [email protected] Abstract: The problems of agriculture affect mostly the smallholder farmers who have small fields in different places. Group-farming cooperatives serves as good alternative to boost food production as well as lifting people out of poverty. In this study we used a recent survey data in Nigeria to examine the effect of membership of group-farming cooperatives on food production and poverty status. Probit regression model estimate is used to analyse the decision to join group-farming cooperatives and the effect of membership of group- farming cooperatives on poverty status and ordinary least square is employed to examine the effect of membership of group-farming cooperatives on food production and productivity of farmers. We find that, group-farming cooperatives have positive and statistically significant effect on food proction at 5% level of significance; prevalence of poverty is higher among non-members of group-farming cooperatives. Being a member of other forms of cooperative also helps to reduce poverty among the farming households. Therefore, we recommend that both the government and non-governmental organization should develop strategies that will encourage participation in group-farming cooperatives and also create more awareness among farming households, which can motivate more farmers to partake in this form of farmers organizations. Acknowledegment: I acknowledge the effort of Dr R.O. Babatunde in this project. JEL Codes: Q18, Q18 #307 Effect of Membership of Group-Farming Cooperatives on Farmers Food Production and Poverty Status in Nigeria Abstract The problems of agriculture affect mostly the small scale farmers who have small fields in different places. -

Odo/Ota Local Government Secretariat, Sango - Agric
S/NO PLACEMENT DEPARTMENT ADO - ODO/OTA LOCAL GOVERNMENT SECRETARIAT, SANGO - AGRIC. & BIO. ENGINEERING 1 OTA, OGUN STATE AGEGE LOCAL GOVERNMENT, BALOGUN STREET, MATERNITY, AGRIC. & BIO. ENGINEERING 2 SANGO, AGEGE, LAGOS STATE AHMAD AL-IMAM NIG. LTD., NO 27, ZULU GAMBARI RD., ILORIN AGRIC. & BIO. ENGINEERING 3 4 AKTEM TECHNOLOGY, ILORIN, KWARA STATE AGRIC. & BIO. ENGINEERING 5 ALLAMIT NIG. LTD., IBADAN, OYO STATE AGRIC. & BIO. ENGINEERING 6 AMOULA VENTURES LTD., IKEJA, LAGOS STATE AGRIC. & BIO. ENGINEERING CALVERTON HELICOPTERS, 2, PRINCE KAYODE, AKINGBADE MECHANICAL ENGINEERING 7 CLOSE, VICTORIA ISLAND, LAGOS STATE CHI-FARM LTD., KM 20, IBADAN/LAGOS EXPRESSWAY, AJANLA, AGRIC. & BIO. ENGINEERING 8 IBADAN, OYO STATE CHINA CIVIL ENGINEERING CONSTRUCTION CORPORATION (CCECC), KM 3, ABEOKUTA/LAGOS EXPRESSWAY, OLOMO - ORE, AGRIC. & BIO. ENGINEERING 9 OGUN STATE COCOA RESEARCH INSTITUTE OF NIGERIA (CRIN), KM 14, IJEBU AGRIC. & BIO. ENGINEERING 10 ODE ROAD, IDI - AYANRE, IBADAN, OYO STATE COKER AGUDA LOCAL COUNCIL, 19/29, THOMAS ANIMASAUN AGRIC. & BIO. ENGINEERING 11 STREET, AGUDA, SURULERE, LAGOS STATE CYBERSPACE NETWORK LTD.,33 SAKA TIINUBU STREET. AGRIC. & BIO. ENGINEERING 12 VICTORIA ISLAND, LAGOS STATE DE KOOLAR NIGERIA LTD.,PLOT 14, HAKEEM BALOGUN STREET, AGRIC. & BIO. ENGINEERING OPP. TECHNICAL COLLEGE, AGIDINGBI, IKEJA, LAGOS STATE 13 DEPARTMENT OF PETROLEUM RESOURCES, 11, NUPE ROAD, OFF AGRIC. & BIO. ENGINEERING 14 AHMAN PATEGI ROAD, G.R.A, ILORIN, KWARA STATE DOLIGERIA BIOSYSTEMS NIGERIA LTD, 1, AFFAN COMPLEX, 1, AGRIC. & BIO. ENGINEERING 15 OLD JEBBA ROAD, ILORIN, KWARA STATE Page 1 SIWES PLACEMENT COMPANIES & ADDRESSES.xlsx S/NO PLACEMENT DEPARTMENT ESFOOS STEEL CONSTRUCTION COMPANY, OPP. SDP, OLD IFE AGRIC. & BIO. ENGINEERING 16 ROAD, AKINFENWA, EGBEDA, IBADAN, OYO STATE 17 FABIS FARMS NIGERIA LTD., ILORIN, KWARA STATE AGRIC. -
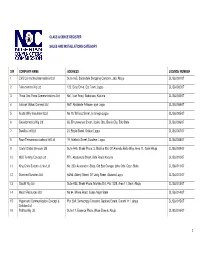
S/N COMPANY NAME ADDRESS LICENSE NUMBER 1 CVS Contracting International Ltd Suite 16B, Sabondale Shopping Complex, Jabi, Abuja CL/S&I/001/07
CLASS LICENCE REGISTER SALES AND INSTALLATIONS CATEGORY S/N COMPANY NAME ADDRESS LICENSE NUMBER 1 CVS Contracting International Ltd Suite 16B, Sabondale Shopping Complex, Jabi, Abuja CL/S&I/001/07 2 Telesciences Nig Ltd 123, Olojo Drive, Ojo Town, Lagos CL/S&I/002/07 3 Three One Three Communications Ltd No1, Isah Road, Badarawa, Kaduna CL/S&I/003/07 4 Latshak Global Concept Ltd No7, Abolakale Arikawe, ajah Lagos CL/S&I/004/07 5 Austin Willy Investment Ltd No 10, Willisco Street, Iju Ishaga Lagos CL/S&I/005/07 6 Geoinformatics Nig Ltd 65, Erhumwunse Street, Uzebu Qtrs, Benin City, Edo State CL/S&I/006/07 7 Dwellins Intl Ltd 21, Boyle Street, Onikan Lagos CL/S&I/007/07 8 Race Telecommunications Intl Ltd 19, Adebola Street, Surulere, Lagos CL/S&I/008/07 9 Clarfel Global Services Ltd Suite A45, Shakir Plaza, 3, Michika Strt, Off Ahmadu Bello Way, Area 11, Garki Abuja CL/S&I/009/07 10 MLD Temmy Concept Ltd FF1, Abeoukuta Street, Bida Road, Kaduna CL/S&I/010/07 11 King Chris Success Links Ltd No, 230, Association Shop, Old Epe Garage, Ijebu Ode, Ogun State CL/S&I/011/07 12 Diamond Sundries Ltd 54/56, Adeniji Street, Off Unity Street, Alakuko Lagos CL/S&I/012/07 13 Olucliff Nig Ltd Suite A33, Shakir Plaza, Michika Strt, Plot 1029, Area 11, Garki Abuja CL/S&I/013/07 14 Mecof Resources Ltd No 94, Minna Road, Suleja Niger State CL/S&I/014/07 15 Hypersand Communication Concept & Plot 29A, Democracy Crescent, Gaduwa Estate, Durumi 111, abuja CL/S&I/015/07 Solution Ltd 16 Patittas Nig Ltd Suite 17, Essence Plaza, Wuse Zone 6, Abuja CL/S&I/016/07 1 17 T.J.