PV Systems for Rural Health Facilities in Developing Areas
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

FAHRENHEIT 451 by Ray Bradbury This One, with Gratitude, Is for DON CONGDON
FAHRENHEIT 451 by Ray Bradbury This one, with gratitude, is for DON CONGDON. FAHRENHEIT 451: The temperature at which book-paper catches fire and burns PART I: THE HEARTH AND THE SALAMANDER IT WAS A PLEASURE TO BURN. IT was a special pleasure to see things eaten, to see things blackened and changed. With the brass nozzle in his fists, with this great python spitting its venomous kerosene upon the world, the blood pounded in his head, and his hands were the hands of some amazing conductor playing all the symphonies of blazing and burning to bring down the tatters and charcoal ruins of history. With his symbolic helmet numbered 451 on his stolid head, and his eyes all orange flame with the thought of what came next, he flicked the igniter and the house jumped up in a gorging fire that burned the evening sky red and yellow and black. He strode in a swarm of fireflies. He wanted above all, like the old joke, to shove a marshmallow on a stick in the furnace, while the flapping pigeon- winged books died on the porch and lawn of the house. While the books went up in sparkling whirls and blew away on a wind turned dark with burning. Montag grinned the fierce grin of all men singed and driven back by flame. He knew that when he returned to the firehouse, he might wink at himself, a minstrel man, Does% burntcorked, in the mirror. Later, going to sleep, he would feel the fiery smile still gripped by his Montag% face muscles, in the dark. -

Songs by Title Karaoke Night with the Patman
Songs By Title Karaoke Night with the Patman Title Versions Title Versions 10 Years 3 Libras Wasteland SC Perfect Circle SI 10,000 Maniacs 3 Of Hearts Because The Night SC Love Is Enough SC Candy Everybody Wants DK 30 Seconds To Mars More Than This SC Kill SC These Are The Days SC 311 Trouble Me SC All Mixed Up SC 100 Proof Aged In Soul Don't Tread On Me SC Somebody's Been Sleeping SC Down SC 10CC Love Song SC I'm Not In Love DK You Wouldn't Believe SC Things We Do For Love SC 38 Special 112 Back Where You Belong SI Come See Me SC Caught Up In You SC Dance With Me SC Hold On Loosely AH It's Over Now SC If I'd Been The One SC Only You SC Rockin' Onto The Night SC Peaches And Cream SC Second Chance SC U Already Know SC Teacher, Teacher SC 12 Gauge Wild Eyed Southern Boys SC Dunkie Butt SC 3LW 1910 Fruitgum Co. No More (Baby I'm A Do Right) SC 1, 2, 3 Redlight SC 3T Simon Says DK Anything SC 1975 Tease Me SC The Sound SI 4 Non Blondes 2 Live Crew What's Up DK Doo Wah Diddy SC 4 P.M. Me So Horny SC Lay Down Your Love SC We Want Some Pussy SC Sukiyaki DK 2 Pac 4 Runner California Love (Original Version) SC Ripples SC Changes SC That Was Him SC Thugz Mansion SC 42nd Street 20 Fingers 42nd Street Song SC Short Dick Man SC We're In The Money SC 3 Doors Down 5 Seconds Of Summer Away From The Sun SC Amnesia SI Be Like That SC She Looks So Perfect SI Behind Those Eyes SC 5 Stairsteps Duck & Run SC Ooh Child SC Here By Me CB 50 Cent Here Without You CB Disco Inferno SC Kryptonite SC If I Can't SC Let Me Go SC In Da Club HT Live For Today SC P.I.M.P. -

(Pdf) Download
Artist Song 2 Unlimited Maximum Overdrive 2 Unlimited Twilight Zone 2Pac All Eyez On Me 3 Doors Down When I'm Gone 3 Doors Down Away From The Sun 3 Doors Down Let Me Go 3 Doors Down Behind Those Eyes 3 Doors Down Here By Me 3 Doors Down Live For Today 3 Doors Down Citizen Soldier 3 Doors Down Train 3 Doors Down Let Me Be Myself 3 Doors Down Here Without You 3 Doors Down Be Like That 3 Doors Down The Road I'm On 3 Doors Down It's Not My Time (I Won't Go) 3 Doors Down Featuring Bob Seger Landing In London 38 Special If I'd Been The One 4him The Basics Of Life 98 Degrees Because Of You 98 Degrees This Gift 98 Degrees I Do (Cherish You) 98 Degrees Feat. Stevie Wonder True To Your Heart A Flock Of Seagulls The More You Live The More You Love A Flock Of Seagulls Wishing (If I Had A Photograph Of You) A Flock Of Seagulls I Ran (So Far Away) A Great Big World Say Something A Great Big World ft Chritina Aguilara Say Something A Great Big World ftg. Christina Aguilera Say Something A Taste Of Honey Boogie Oogie Oogie A.R. Rahman And The Pussycat Dolls Jai Ho Aaliyah Age Ain't Nothing But A Number Aaliyah I Can Be Aaliyah I Refuse Aaliyah Never No More Aaliyah Read Between The Lines Aaliyah What If Aaron Carter Oh Aaron Aaron Carter Aaron's Party (Come And Get It) Aaron Carter How I Beat Shaq Aaron Lines Love Changes Everything Aaron Neville Don't Take Away My Heaven Aaron Neville Everybody Plays The Fool Aaron Tippin Her Aaron Watson Outta Style ABC All Of My Heart ABC Poison Arrow Ad Libs The Boy From New York City Afroman Because I Got High Air -

Songs by Title
Songs by Title Title Artist Versions Title Artist Versions #1 Crush Garbage SC 1999 Prince PI SC #Selfie Chainsmokers SS 2 Become 1 Spice Girls DK MM SC (Can't Stop) Giving You Up Kylie Minogue SF 2 Hearts Kylie Minogue MR (Don't Take Her) She's All I Tracy Byrd MM 2 Minutes To Midnight Iron Maiden SF Got 2 Stars Camp Rock DI (I Don't Know Why) But I Clarence Frogman Henry MM 2 Step DJ Unk PH Do 2000 Miles Pretenders, The ZO (I'll Never Be) Maria Sandra SF 21 Guns Green Day QH SF Magdalena 21 Questions (Feat. Nate 50 Cent SC (Take Me Home) Country Toots & The Maytals SC Dogg) Roads 21st Century Breakdown Green Day MR SF (This Ain't) No Thinkin' Trace Adkins MM Thing 21st Century Christmas Cliff Richard MR + 1 Martin Solveig SF 21st Century Girl Willow Smith SF '03 Bonnie & Clyde (Feat. Jay-Z SC 22 Lily Allen SF Beyonce) Taylor Swift MR SF ZP 1, 2 Step Ciara BH SC SF SI 23 (Feat. Miley Cyrus, Wiz Mike Will Made-It PH SP Khalifa And Juicy J) 10 Days Late Third Eye Blind SC 24 Hours At A Time Marshall Tucker Band SG 10 Million People Example SF 24 Hours From Tulsa Gene Pitney MM 10 Minutes Until The Utilities UT 24-7 Kevon Edmonds SC Karaoke Starts (5 Min 24K Magic Bruno Mars MR SF Track) 24's Richgirl & Bun B PH 10 Seconds Jazmine Sullivan PH 25 Miles Edwin Starr SC 10,000 Promises Backstreet Boys BS 25 Minutes To Go Johnny Cash SF 100 Percent Cowboy Jason Meadows PH 25 Or 6 To 4 Chicago BS PI SC 100 Years Five For Fighting SC 26 Cents Wilkinsons, The MM SC SF 100% Chance Of Rain Gary Morris SC 26 Miles Four Preps, The SA 100% Pure Love Crystal Waters PI SC 29 Nights Danni Leigh SC 10000 Nights Alphabeat MR SF 29 Palms Robert Plant SC SF 10th Avenue Freeze Out Bruce Springsteen SG 3 Britney Spears CB MR PH 1-2-3 Gloria Estefan BS SC QH SF Len Barry DK 3 AM Matchbox 20 MM SC 1-2-3 Redlight 1910 Fruitgum Co. -

Songs by Artist
Songs by Artist Title Title (Hed) Planet Earth 2 Live Crew Bartender We Want Some Pussy Blackout 2 Pistols Other Side She Got It +44 You Know Me When Your Heart Stops Beating 20 Fingers 10 Years Short Dick Man Beautiful 21 Demands Through The Iris Give Me A Minute Wasteland 3 Doors Down 10,000 Maniacs Away From The Sun Because The Night Be Like That Candy Everybody Wants Behind Those Eyes More Than This Better Life, The These Are The Days Citizen Soldier Trouble Me Duck & Run 100 Proof Aged In Soul Every Time You Go Somebody's Been Sleeping Here By Me 10CC Here Without You I'm Not In Love It's Not My Time Things We Do For Love, The Kryptonite 112 Landing In London Come See Me Let Me Be Myself Cupid Let Me Go Dance With Me Live For Today Hot & Wet Loser It's Over Now Road I'm On, The Na Na Na So I Need You Peaches & Cream Train Right Here For You When I'm Gone U Already Know When You're Young 12 Gauge 3 Of Hearts Dunkie Butt Arizona Rain 12 Stones Love Is Enough Far Away 30 Seconds To Mars Way I Fell, The Closer To The Edge We Are One Kill, The 1910 Fruitgum Co. Kings And Queens 1, 2, 3 Red Light This Is War Simon Says Up In The Air (Explicit) 2 Chainz Yesterday Birthday Song (Explicit) 311 I'm Different (Explicit) All Mixed Up Spend It Amber 2 Live Crew Beyond The Grey Sky Doo Wah Diddy Creatures (For A While) Me So Horny Don't Tread On Me Song List Generator® Printed 5/12/2021 Page 1 of 334 Licensed to Chris Avis Songs by Artist Title Title 311 4Him First Straw Sacred Hideaway Hey You Where There Is Faith I'll Be Here Awhile Who You Are Love Song 5 Stairsteps, The You Wouldn't Believe O-O-H Child 38 Special 50 Cent Back Where You Belong 21 Questions Caught Up In You Baby By Me Hold On Loosely Best Friend If I'd Been The One Candy Shop Rockin' Into The Night Disco Inferno Second Chance Hustler's Ambition Teacher, Teacher If I Can't Wild-Eyed Southern Boys In Da Club 3LW Just A Lil' Bit I Do (Wanna Get Close To You) Outlaw No More (Baby I'ma Do Right) Outta Control Playas Gon' Play Outta Control (Remix Version) 3OH!3 P.I.M.P. -

Chronobiology with Katherine Hatcher Ologies Podcast December 10, 2019
Chronobiology with Katherine Hatcher Ologies Podcast December 10, 2019 Oh hey, it’s your invisible aligners you don’t wear anywhere near 22 hours a day, and they know it, and you know it, Alie Ward, back with another episode of Ologies. I’m alive, y’all! I slept so many hours over the last couple of weeks dealing with this flu… Whooo! When are you listening to this? Are you turning the coffee pot on and feeding the dog? Are you on the 7am train to work? Is it your lunch break and you have half a burrito spinning slowly in a microwave? Maybe the sun is setting while you walk to your car. Are you nursing a human who has decided to snack on your boobage at 4am? At least once a day it seems we look at a clock and we’re cranky about it. Myself, very much so, all the time. So, we are here to talk about why. But first, we’re going to talk about you, saying thank you so much for supporting via Patreon.com/Ologies, for sending in your questions that way, for wearing Ologies shirts and hats from OlogiesMerch.com – we have some great new designs up by the by – and for telling friends, and maybe foes, and in-laws about Ologies, and keeping it up in the charts by rating it and subscribing on all of your devices. And of course for leaving a review; you know I’m gonna lurk them, just like a gentle, happy, creep so I can read one back to you. -
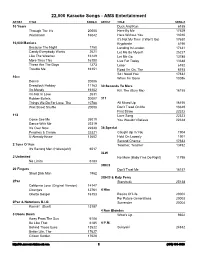
2 Column Indented
22,000 Karaoke Songs - AMS Entertainment ARTIST TITLE SONG # ARTIST TITLE SONG # 10 Years Duck And Run 6188 Through The Iris 20005 Here By Me 17629 Wasteland 16042 Here Without You 13010 It's Not My Time (I Won't Go) 17630 10,000 Maniacs Kryptonite 6190 Because The Night 1750 Landing In London 17631 Candy Everybody Wants 2621 Let Me Be Myself 25227 Like The Weather 16149 Let Me Go 13785 More Than This 16150 Live For Today 13648 These Are The Days 1273 Loser 6192 Trouble Me 16151 Road I'm On, The 6193 So I Need You 17632 10cc When I'm Gone 13086 Donna 20006 Dreadlock Holiday 11163 30 Seconds To Mars I'm Mandy 16152 Kill, The (Bury Me) 16155 I'm Not In Love 2631 Rubber Bullets 20007 311 Things We Do For Love, The 10788 All Mixed Up 16156 Wall Street Shuffle 20008 Don't Tread On Me 13649 First Straw 22322 112 Love Song 22323 Come See Me 25019 You Wouldn't Believe 22324 Dance With Me 22319 It's Over Now 22320 38 Special Peaches & Cream 22321 Caught Up In You 1904 U Already Know 13602 Hold On Loosely 1901 Second Chance 17633 2 Tons O' Fun Teacher, Teacher 13492 It's Raining Men (Hallelujah!) 6017 3LW 2 Unlimited No More (Baby I'ma Do Right) 11795 No Limits 6183 3Oh!3 20 Fingers Don't Trust Me 16157 Short Dick Man 1962 3OH!3 & Katy Perry 2Pac Starstrukk 25138 California Love (Original Version) 14147 Changes 12761 4 Him Ghetto Gospel 16153 Basics Of Life 20002 For Future Generations 20003 2Pac & Notorious B.I.G. -

Songs by Artist
Songs by Artist Karaoke Collection Title Title Title +44 18 Visions 3 Dog Night When Your Heart Stops Beating Victim 1 1 Block Radius 1910 Fruitgum Co An Old Fashioned Love Song You Got Me Simon Says Black & White 1 Fine Day 1927 Celebrate For The 1st Time Compulsory Hero Easy To Be Hard 1 Flew South If I Could Elis Comin My Kind Of Beautiful Thats When I Think Of You Joy To The World 1 Night Only 1st Class Liar Just For Tonight Beach Baby Mama Told Me Not To Come 1 Republic 2 Evisa Never Been To Spain Mercy Oh La La La Old Fashioned Love Song Say (All I Need) 2 Live Crew Out In The Country Stop & Stare Do Wah Diddy Diddy Pieces Of April 1 True Voice 2 Pac Shambala After Your Gone California Love Sure As Im Sitting Here Sacred Trust Changes The Family Of Man 1 Way Dear Mama The Show Must Go On Cutie Pie How Do You Want It 3 Doors Down 1 Way Ride So Many Tears Away From The Sun Painted Perfect Thugz Mansion Be Like That 10 000 Maniacs Until The End Of Time Behind Those Eyes Because The Night 2 Pac Ft Eminem Citizen Soldier Candy Everybody Wants 1 Day At A Time Duck & Run Like The Weather 2 Pac Ft Eric Will Here By Me More Than This Do For Love Here Without You These Are Days 2 Pac Ft Notorious Big Its Not My Time Trouble Me Runnin Kryptonite 10 Cc 2 Pistols Ft Ray J Let Me Be Myself Donna You Know Me Let Me Go Dreadlock Holiday 2 Pistols Ft T Pain & Tay Dizm Live For Today Good Morning Judge She Got It Loser Im Mandy 2 Play Ft Thomes Jules & Jucxi So I Need You Im Not In Love Careless Whisper The Better Life Rubber Bullets 2 Tons O Fun -

Download 1941-06-12
^ r-«-* *•»••'•'»'»v«' H-i-?in.m!in. Library Page Eight THE BRANFORD REVIEW, BRANFORD, COKN., JUNE 6, 1941 THE HOME TOWS PAPER nations are ot non-White or mixed this young inen should visit on THE HOME NEWSPAPER IS A ot blood. The Nazi and Communist his leave from <:amp. Neither in VITAL FORCE IN EVERY TOWN NORTH BRANFORD THE POCKETBOOK propagandists down there point dustrialists nor laborer has as yet Business Directory BRANFORD—NORTH BRANFORD with malicious glee at our race shown any willingness to make any STONY CREEK—PINE ORCHARD PORTRAYING AS IT DOES (/KNOWLEDGE pride and Intolerance here. They sacrifice tor the preservation of SHORT BEACH — INDIAN NECK LOCAL HAPPENINGS IN Services In the local churches on alumni dinner at the commence say with very plausible credibility this land unless they are well paid 42 Inoh sink ana tab osmblnatlm GRANNIS CORNER—MORRIS FAMILIAR LANGUAGE Sunday will be: ment exercises of the Berkeley that we are not to be trusted. Our for it. Instead of all classes joining COVE—EAST HAVEN CJe Ptanfotb i^ebteto $29.95 complete. Toilet ontflts Mass at 0:15 o'clock at St, Augus Divinity School on Wednesday, Ronulne interest In an Internation together in a really Democratic campleta $12.95. Bath tubs I14.S*. AND EAST HAVEN NEWS tine's R, C. Church, Rev William al democracy upon which our sur fashion, we, all ot us, want to make The North Branford Fife and Wall Basins $5.45. Conn. Plumblnf Brewer, pastor, Mrs. Edward Daly, vival as nation depends Is betrayed ourselves as rich as we can through VOL, XIV—No, 9 Braivtord, Connecticut, Thursday, June 12, 1041 organist and choir director., Drum Corps held a special meeting by our lack ot true democracy at this present trouble as rich as we and Heattng Materials Co., 1730 Price Five Ceata Dominican Nuns from New Haven on Tuesday evening at the club home which recognizes the equal can make ourselves In a gentle State St, New Baven, Conn., •will instruct children ol St, Augus house. -
Songs in the Key of Z
covers complete.qxd 7/15/08 9:02 AM Page 1 MUSIC The first book ever about a mutant strain ofZ Songs in theKey of twisted pop that’s so wrong, it’s right! “Iconoclast/upstart Irwin Chusid has written a meticulously researched and passionate cry shedding long-overdue light upon some of the guiltiest musical innocents of the twentieth century. An indispensable classic that defines the indefinable.” –John Zorn “Chusid takes us through the musical looking glass to the other side of the bizarro universe, where pop spelled back- wards is . pop? A fascinating collection of wilder cards and beyond-avant talents.” –Lenny Kaye Irwin Chusid “This book is filled with memorable characters and their preposterous-but-true stories. As a musicologist, essayist, and humorist, Irwin Chusid gives good value for your enter- tainment dollar.” –Marshall Crenshaw Outsider musicians can be the product of damaged DNA, alien abduction, drug fry, demonic possession, or simply sheer obliviousness. But, believe it or not, they’re worth listening to, often outmatching all contenders for inventiveness and originality. This book profiles dozens of outsider musicians, both prominent and obscure, and presents their strange life stories along with photographs, interviews, cartoons, and discographies. Irwin Chusid is a record producer, radio personality, journalist, and music historian. He hosts the Incorrect Music Hour on WFMU; he has produced dozens of records and concerts; and he has written for The New York Times, Pulse, New York Press, and many other publications. $18.95 (CAN $20.95) ISBN 978-1-55652-372-4 51895 9 781556 523724 SONGS IN THE KEY OF Z Songs in the Key of Z THE CURIOUS UNIVERSE OF O U T S I D E R MUSIC ¥ Irwin Chusid Library of Congress Cataloging-in-Publication Data Chusid, Irwin. -

ESL NEWSLETTER a Publication from Spring Semester 2009 English As a Second Language Students
ESL NEWSLETTER A publication from Spring Semester 2009 English as a Second Language Students Superstitions as a Part of or avoid doing in their everyday life out of fear that something bad will happen. For example, Russian Culture people do not whistle indoors because they By Olga Betzel Every culture has a certain set of beliefs might lose all their money, if they do. I have that reflect its history and the way its people been living in the USA for about a year and still view the world. These beliefs can be either do not feel comfortable hearing somebody rational or irrational. For centuries people all whistling indoors or in the car. In Russia, as over the world tried to explain things they did well as in some other cultures, talking about not understand, and one of the ways to get future success, especially boasting about it is control over the considered bad luck. It’s safer to be silent or to unexplainable was to sound pessimistic until the success has been believe in superstitions. achieved even when one is sure of success. If Despite the fact that you cannot help yourself, after saying, “Next modern science has month I will get a promotion”, immediately spit proved most of the three times over your left shoulder. Don’t do it irrational beliefs wrong and literally – three symbolic spits will do. You can senseless, in some also knock on wood. Knocking on wood is cultures people still, cling to practiced in Russia as well as in other superstitions in their countries; however, everyday life. -
Poets on the Prairie
King Essay http://weberjournal.weber.edu/archive/archive%20B%20Vol.%2011-16.1/Vol.%2016.1... Home Archives Reading Room Search Editorial Info Books Subscribe West Links Fall 1998, Volume 16.1 Essay Robert King Poets on the Prairie Robert King received a Ph.D. in English/Creative Writing from the University of Iowa. His publications include two poetry chapbooks (Standing Around Outside, 1979; A Circle of Land, 1990) and poems in such magazines as Ascent, Kansas Quarterly, Nebraska Review, North Dakota Quarterly, and Massachusetts Review. A Professor Emeritus from the University of North Dakota, he is currently a Visiting Professor at the University of Nebraska at Lincoln. Read other work by Robert King published in Weber Studies: Vol. 18.1 (poetry), Vol. 20.3 (essay), and Vol. 23.1 (essay). It was a good idea, it was a bad idea, it could go either way. I was new to Nebraska by a few months and it wasn’t any of my business in the first place so no one was asking me to have an opinion, but I thought I should. It was easy enough to see where the idea came from. The annual Western Literature Conference was coming to Lincoln in the fall. The organizers wanted to do something special with poetry and the idea of a field trip came up. Poets. Prairie poets. A field trip—to a prairie—to hear poets. Lincoln had a small prairie nearby and, God knows, it had enough poets, since it sometimes seems you can’t swing a cat in Nebraska without hitting a poet.