2011-2012 Student Handbook
Total Page:16
File Type:pdf, Size:1020Kb
Load more
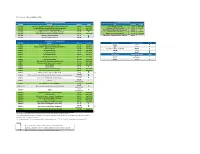
Recommended publications
-

31-Thirty Hunters Point Avenue
31-THIRTY HUNTERS POINT AVENUE FACTORY DISTRICT / LONG ISLAND CITY, NY 11101 / FOR LEASE FIRST FLOOR FLOOR PLAN VAN DAM STREET 18,000 SF FEATURES: • 18,000 sf first floor (additonally 4,000 sf can be made available on the second floor) • 16’ ceiling • 1 drive-in door (can create another drive-in EXISITING DRIVE-IN or loading dock) AMENITIES: • 25’ x 30’ column spacing • Bus Line • Built in 1962 • Metro/Subway • Zone M2-1 HUNTER’S POINT AVENUE POTENTIAL LOCATION & TRANSIT: LOADING DOCK OR DRIVE-IN Subway: #7 (33rd Street Rawson stop) Buses: Q67, Q32, & Q60 bus lines 31ST PLACE Facing LIE with easy access BQE, Midtown Tunnel & 59th Street Bridge FOR MORE INFORMATION, PLEASE CONTACT: Commission computed and earned in accordance with the rates and conditions of our agency agreement with our MICHAEL DEUTSCH JOSEPH MEYERSON JOSEPH GROTTO JR. principal, when received from our principal, will be paid to a cooperating broker who consummates a sublease which 914 299 1302 718 512 2620 212 318 9727 is unconditionally executed and delivered by and between sublandlord and subtenant. (A copy of the rates and [email protected] [email protected] [email protected] conditions referred to above are available upon request.) 31-THIRTY HUNTERS POINT AVENUE FACTORY DISTRICT / LONG ISLAND CITY, NY 11101 / FOR LEASE Transit/Subway Distance 33 Street (7 Line) Transit Stop 0.7 mi Hunters Point Avenue Transit Stop 0.8 mi Queens Plaza Transit Stop (E, M, R) 0.9 mi 40 Street-Lowery Street Transit Stop (7) 0.9 mi Long Island City-Court Square Transit Stop (G) 1.0 mi Commuter Rail Distance Hunter’s Point Avenue Station Commuter Rail(Oyster Bay 0.8 mi Branch, Hempstead Branch) Woodside Station Commuter Rail (Ronkonkoma Branch,Long Beach Branch, Port Jefferson Branch, 3.6 mi Hempstead Branch, Montauk Branch, Babylon Branch) Airport Drive Distance La Guardia Airport 10 min 5.9 mi John F. -
May 2020 Update
PTC Dashboard - LIRR and MNR (May 2020) System Software Baseline Releases PTC Safety Plan (PTCSP) Release Purpose Deadline Status RR Planned Current 3.5 MNR System Level Software (Wayside, Office, Onboard Equipment) May-19 May-19 (A) PTCSP submitted to LIRR Jun-19 Jun-19 (A) 3.5 LIRR Supports RSD on pilots and ERSD on non-pilot segments Jun-19 Jun-19 (A) LIRR submits PTCSP to the FRA Jul-19 Jul-19 (A) 3.6 LIRR Supports ERSD for non-pilot segments Oct-19 Oct-19 (A) LIRR PTCSP in review by FRA for Approval Oct-20 3.6 MNR System Release for Variance Fix (Wayside, Office) Jun-20 PTCSP submitted to MNR Jul-19 Jul-19 (A) 3.7 LIRR Supports ERSD for non-pilot segments with B2B Mar-20 Mar-20 (A) MNR submits PTCSP to the FRA Aug-19 Aug-19 (A) 3.8 LIRR HMAC and STS-STS Interface Jun-20 MNR PTCSP in review by FRA for Approval Oct-20 3.9 LIRR Operational Improvements Sep-20 Line Segments in Revenue Service Railroad Segment Planned Current MNR Tenants Interoperability date Status LIRR/3.5 Port Washington Branch (Pilot Line 2) Dec-18 Dec-18 (A) Amtrak Dec-20 LIRR/3.5 Montauk Branch - Babylon to Patchogue (Pilot Line 1) Dec-18 Dec-18 (A) CSX Dec-20 LIRR/3.5 Oyster Bay Branch Oct-19 Oct-19 (A) Providence & Worcester (P&W) Dec-20 LIRR/3.5 Hempstead Branch Oct-19 Aug-19 (A) PanAm Dec-20 LIRR/3.5 Long Beach Branch Oct-19 Oct-19 (A) Cdot Dec-20 LIRR/3.5 Far Rockaway Branch Nov-19 Oct-19 (A) LIRR TenantsInteroperability date Status Oct-20 LIRR/3.5 West Hempstead Branch Nov-19 Oct-19 (A) Amtrak (was Sep-20) LIRR/3.5 Port Jefferson Branch Nov-19 Nov-19 (A) NYAR -

BJ's Wholesale Club-30 Route 17, Blk 501, Lot 5
STONEFIELD August 4, 2020 Borough of Paramus Planning Board 1 West Jockish Square #1 Paramus, New Jersey 07652 RE: Traffic & Parking Assessment Report Proposed Fueling Service Addition to BJ’s Wholesale Club Block 501, Lot 5 and Block 502, Lots 2.02 & 9 30 NJSH Route 17 North Borough of Paramus, Bergen County, New Jersey SE&D Job No. S-19114 Dear Board Members: Stonefield Engineering and Design, LLC (“Stonefield”) has prepared this analysis to examine the potential traffic and parking impacts of the proposed fuel service addition to the existing BJ’s Wholesale Club on the adjacent roadway network. The subject property is located along NJSH Route 17 North to the south of NJSH Route 4 in the Borough of Paramus, Bergen County, New Jersey. The subject property is designated as Block 501, Lot 5, and Block 502, Lot 9 and 2.02 as depicted on the Borough of Paramus Tax Map. The site has approximately 905 feet of frontage along the NJSH Route 17 North off-ramp to NJSH Route 4. The existing site is currently developed with a BJ’s Wholesale Club. Access is currently provided via one (1) right-turn ingress- only driveway along NJSH Route 17 North, one (1) right-turn ingress-only driveway along South Farview Avenue, and one (1) right-turn egress-only driveway along South Farview Avenue. Under the proposed development program, a fueling station with 10 fueling positions would be constructed in the southerly portion of the existing parking area. The construction of the fueling station would result in a net reduction to the overall parking supply of 103 parking spaces, and 445 parking spaces would be provided for the existing BJ’s Wholesale Club. -

2000 LIRR Report Card Results of the Annual, Independent Rider Survey from the Long Island Rail Road Commuters' Council
The 2000 LIRR Report Card Results of the Annual, Independent Rider Survey from the Long Island Rail Road Commuters' Council Michael T. Doyle Associate Director Joshua Schank Transportation Planner October 2000 Long Island Rail Road Commuters' Council 347 Madison Avenue, New York, NY 10017 (212) 878-7087 • www.lirrcc.org © 2000 LIRRCC Acknowledgements The authors would like to thank the members of the LIRRCC for their invaluable efforts in performing survey research in the field, and the Long Island Rail Road for its cooperation during survey activities. The authors also gratefully acknowledge technical assistance provided by former PCAC Associate Director Alan Foster. The Long Island Rail Road Commuters' Council (LIRRCC) is the legislatively mandated representative of the ridership of MTA Long Island Rail Road. Our 12 volunteer members are regular users of the LIRR system and are appointed by the Governor upon the recommendation of the Nassau and Suffolk County Executives, and Brooklyn and Queens Borough Presidents. The Council is an affiliate of the Permanent Citizens Advisory Committee to the MTA (PCAC). For more information, please visit our website: www.lirrcc.org. Table of Contents Executive Summary 1 Methodology 3 Results for Performance Indicators 5 Systemwide Results 5 Results by Branch 10 Results for Customer Comments 17 Systemwide Results 17 Results by Branch 20 Representative Customer Comments 25 Service Delivery 25 Service Requirements 25 Scheduling 28 On-Time Performance 31 Operations 32 Maintenance of Service During Severe -

Long Island Rail Road T E a Shelter Island) Montauk D M U N S S O H Ip D C N O L A
B r i d Cross Sound Ferry g e p o (Orient Point, LI- r t & New London, Conn) P Greenport o r North Ferry Co. t J e (Greenport-Shelter Island) f f e r s o Southold n South Ferry Co. S (North Haven- Long Island Rail Road t e a Shelter Island) Montauk d m u n s o h S i p d C n o l a . Key I s Mattituck g Amagansett o n East Hampton Full Time rail station L Peconic Port Jefferson Bridgehampton Accessible station Bay Stony Brook Part Time rail station Riverhead PORT JEFFERSON BRANCH Southampton Kings Park Major Transit Hub St. James Hampton Bays Locust Valley Northport MONTAUK BRANCH © 2020 Metropolitan Transportation Authority Oyster Bay Glen Cove Greenlawn Smithtown SUFFOLK Westhampton Glen Street OYSTER BAY BRANCH Huntington Speonk Port Sea Cliff RONKONKOMA BRANCH Yaphank Washington Cold Spring Harbor PORT WASHINGTON BRANCH Glen Head Medford Manhas Syosset Ronkonkoma G Plandome Greenvale Mastic-Shirley r THE ea s t e NA SSAU BRONX Li Nec t Central Islip t Bellport Doug tle Nec k Roslyn Brentwood Fl N N M ush Aubu Patchogue A B B l et i Murra a asto k Albertson Hicksville Great Oakdale T s ng–M road Deer Park -W rnda ysi Davis Park T n River i y w d New Mer East Wyandanch A ll a Hi le e M Sayville Ferry Co. et in S ay i Williston W s l i neol Pinelawn Islip Poin l F H llon Westbury NH oo t loral y d B de P a Farmingdale A s t e A Carle Place Bethpage Bay Shore Sayville Ferry id QUEENS lle Par v M e Queens k s ros Service, Inc. -

Master Plan for the Borough of Montvale, Bergen County, NJ
Master Plan for the Borough of Montvale, Bergen County, NJ Prepared for the Montvale Planning Board by Phillips Preiss Shapiro Associates, Inc. Planning & Real Estate Consultants Adopted April 1, 2008 MASTER PLAN FOR THE BOROUGH OF MONTVALE BERGEN COUNTY, NEW JERSEY Prepared for The Montvale Planning Board Prepared by Phillips Preiss Shapiro Associates, Inc. Planning and Real Estate Consultants 434 Sixth Avenue New York, New York 10011 125 Half Mile Road—Suite 200 Red Bank, New Jersey 07701 Adopted April 1, 2008 Table of Contents Page CHAPTER 1. INTRODUCTION 1 A. Introduction 1 B. Purpose 1 C. Brief History of Montvale 1 1. Early History 1 2. Incorporation (1894 to 1950) 3 3. 1950 to the Present 4 D. Scope of Master Plan 4 E. Context for Preparation of Master Plan 5 1. Development in Corporate Office Sector 5 2. Downtown Renaissance 6 3. Diversification of Housing Stock 6 4. Acquisition and Improvement of Public Parks and Open Space 6 5. New Community Facilities 7 CHAPTER 2. COMMUNITY RESIDENT AND BUSINESS SURVEYS 8 A. Introduction 8 B. Community Resident Survey 8 1. Purpose and Scope of Survey 8 2. Survey Results 10 C. Community Business Survey 30 1. Purpose and Scope of Survey 30 2. Results of the Survey 31 3. Analysis of the Survey Results 42 CHAPTER 3. GOALS AND OBJECTIVES 44 CHAPTER 4. LAND USE 47 A. Introduction 47 B. Existing Uses 47 1. Residential 47 2. Non-Residential 52 C. Existing Zoning 56 1. Residential 58 D. Consistency of Existing Uses With Current Zoning 61 E. Montvale’s Land Use Plan 62 F. -
Department of Energy. Remedial Action Work Plan For
# - i-aq'f 'l.n't{i(ni; ',.Jp ..f*{ oRo-850 REMEDIAL ACTION WORK PLAN FOR THE MAYI'IOOD SITE JULY I9B4 UNITED STATES DEPARTMENT OF ENERGY OAK RIDGE OPERATIONS TABLE OF CONTENTS Page 1.0 Introduction and Objectives I l.I Background I L.2 Site ldentification I 1.3 Purpose 3 2.O Site Description 4 2.L Site Location and Description 4 2.2 Radiological Description 4 2.3 Site Geology and Hydrology 7 3.0 Management Approach 9 4.0 Work Plan 11 4.L Remedial Action Criteria I1 4.2 Site Characterization L4 4.3 Prelininary Engineering I5 . 4.4 NEPA 16 4.5 Design Engineering L7 4.6 Access Agreenents I7 4.7 Renedial Actions L7 4.8 Occupational Exposures 2L 4.9 Verification Sampling and Analysis 23 4. l0 Waste Volume Projections 25 4.Il Quality Assurance 25 4.L2 l"taintenance and Surveillance 25 5.0 Schedule and Cost 28 6.0 References 30 Appendix A Radiological Survey/t'tonitoring Plan 111 LIST OF FIGURES FIGURE TITLE PAGE I-L t"laywood Interim Storage Site and Vicinity Properties 2-L Waste Burial Sites on Stepan Company Property 4-L Proposed Storage Pile at the MISS 22 5-1 Maywood Site Schedule and Cost Summary 29 LIST OF TABLES TABLE TITLE PAGE 4-L Sunmary of Residual Contamination Guidelines L2 for the Maywood Site 4-2 Approximate Waste Volume Projections 27 tv I.O INTRODUCTIONAND OBJECTIVES }.1 BACKGROUND The United States Government initiated the Forurerly Utilized Sites Remedial Action Program (FUSRAP) in L974. -

SNPLI Long Island REGIONAL #2 SITE INFORMATION April 12 – April 14, 2018
SNPLI Long Island REGIONAL #2 SITE INFORMATION April 12 – April 14, 2018 Event Location Hofstra University Arena 1000 Fulton Avenue Hempstead, NY 11550 Phone: (516) 463-6600 NOTE: The site will not accept or store team robots or toolboxes. http://www.sbpli-lifirst.org/robotics.html http://www.hofstra.edu/home/index.html Directions to Hofstra University Arena For directions and bus and train schedules use the web address below: http://www.hofstra.edu/StudentServ/IC/ic_hofstra_directions.cfm From New York City: From the Queens Midtown Tunnel, continue on the Long Island Expressway (I-495) East to exit 38, Northern State Parkway East, to the Meadowbrook Parkway South (exit 31A) ... Stay on the Meadowbrook Parkway until Exit M4 (sign reads "Hempstead" and "Coliseum") Follow "From All Points," below. From southern New Jersey, southeast Pennsylvania, Maryland, Washington, D.C., and Virginia: Take N.J. Turnpike to Exit 13. Follow Route 278 to Verrazano-Narrows Bridge. Take left exit off bridge onto the Belt Parkway East. Take that to Exit 25A (Southern State Parkway East — the Belt Parkway splits, stay left). Take that to Exit 22N (Meadowbrook Parkway North). Stay on the Meadowbrook Parkway until Exit M4 (sign reads "Hempstead" and "Coliseum"). Follow "From All Points," below. From northwestern New Jersey, northern Pennsylvania, and the Middle States: Take either Interstate 78, Interstate 80, US Route 22, New Jersey Route 4, or New Jersey Route 17 to the George Washington Bridge. Proceed over the bridge to the Cross Bronx Expressway onto the Throgs Neck Bridge:Follow directions from Throgs Neck Bridge, detailed below. -

12-45 River Road, Fair Lawn, New Jersey 1 the Appraisal
12-45 RIVER ROAD, FAIR LAWN, NEW JERSEY THE APPRAISAL OF 12-45 RIVER ROAD BOROUGH OF FAIR LAWN BERGEN COUNTY, NEW JERSEY 07410 Presented by ERICKSON APPRAISAL COMPANY Prepared for MS. JANETH ARIAS FREEDOM BANK 99 WEST ESSEX STREET – 2ND FLOOR MAYWOOD, NEW JERSEY 07607 AS OF AUGUST 18, 2015 “AS IS VALUE” & AS OF NOVEMBER 18, 2015 “STABILIZED VALUE” Prepared by WILLIAM J. DOKA, SRA, SCGREA #00104 ERICKSON APPRAISAL COMPANY 17-10 RIVER ROAD, SUITE 4D FAIR LAWN, NEW JERSEY 07410 201-956-6094 1 12-45 RIVER ROAD, FAIR LAWN, NEW JERSEY DEFINITIONS......................................................................................................................... 5 ASSUMPTIONS AND LIMITING CONDITIONS........................................................ 6-8 CERTIFICATION ............................................................................................................. 9-11 SUMMARY OF PERTINENT FACTS............................................................................... 12 MARKETING AND EXPOSURE TIME.............................................................................13 PURPOSE, RIGHTS, FUNCTION OF THE REPORT.................................................. 14 DEFINITION OF VALUE BEING APPRAISED INTENDED USER ....................... 14 SCOPE OF THE REPORT................................................................................................... 15 COUNTY/CITY/NEIGHBORHOOD DESCRIPTION................................................ 16-19 ZONING/UTILITIES/HISTORY.................................................................................. -

S ST. MARK's FAMILY S
ST. MARK’S FAMILY S s “Celebrating God’s Inclusive Love.” st. mark’s episcopal church 118 Chadwick Road • Teaneck, NJ 07666 (201) 836-7275 HELLO! WE ARE READY!! he members of the Search Committee of St. Mark’s Episcopal Church in T Teaneck, New Jersey say, “Welcome!” We invite you to read about us and prayerfully decideS if this could be your church. You’ll find here a lively, active parish filleds with strong lay leadership, active and talented parishioners of all ages, many races, and varying points of view. We are single, married, with or without children, in various stages of spiritual devel- opment, but all sharing an abiding love of Christ and the St. Mark’s community. We seek a full-time rector who will thrive in our community of souls who love beautiful music and the liturgy, who love to celebrate together, and who serve the people both inside our parish, and outside in our greater Teaneck neighborhood and beyond. The first part of this profile is our collective voice speaking to you, giving you our best understanding of who we are, how we worship, the qualities we love about ourselves and the areas where we are challenged to grow. The second part of this profile is an appendix which gives you the “nuts and bolts” of the parish: descriptions of the building, diocese and neighborhood, financials and attendance, current staff and other parish data. Areas where we seek leadership include: Taking an activist role in addressing major political and social issues; becoming more proactive in developing our financial stewardship; and growing our youth ministry. -

E H R I C H S G R a H N Rengifo
s t e v e n j o h a n n e s e h r i c h s G r a h n e r i k r e n G i fo t h o m a s b e k a s s t e p h a n b a r e a a . j . l a z a 2010 Hofstra University Men’s Soccer Quick Facts Location: Hempstead, New York 11549 Director of Special Events: table of contents Founded: 1935 Chrissy Arnone Enrollment: 12,100 Athletic Department Phone: 1 Quick Facts/ Nickname: Pride (516) 463-6750 Table of Contents Colors: Gold, White and Blue 2 This is Hofstra University Affiliation: NCAA Division I Senior Assistant Director of Athletic Conference: Colonial Athletic Association Communications/ 4 Head Coach Richard Nuttall Home Field: Hofstra Soccer Stadium Soccer Contact: Jeremy Kniffin 6 Assistant Coaches (1,600) Office Phone: (516) 463-6759 7 2010 Roster Surface: Field Turf Office Fax: (516) 463-5033 8 2010 Outlook Press Table Phone: (516) 523-6185 Cell Phone: (516) 523-6185 10 Player Bios E-mail Address: 23 Hofstra University President President: Stuart Rabinowitz [email protected] Faculty Athletics Representative: Associate Director of Athletics for 24 University Senior Dr. Michael Barnes Communications: Administration/Trustees Director of Athletics: Jack Hayes Stephen Gorchov 25 Hofstra University Director Executive Associate Director of Athletics: Office Phone: (516) 463-4933 of Athletics Danny McCabe Senior Sports Information Director: 26 Hofstra Athletic Administration Senior Associate Director of Athletics: Jim Sheehan and Head Coaches Cindy Lewis Office Phone: (516) 463-6764 28 Hofstra Heritage Associate Director of Athletics for -

New York State Public Transportation Safety Board Rail Safety Section Abbreviated Report Case Number: 9260
NEW YORK STATE PUBLIC TRANSPORTATION SAFETY BOARD RAIL SAFETY SECTION ABBREVIATED REPORT CASE NUMBER: 9260 DATE OF ACCIDENT: February 2, 2007 CARRIER: MTA Long Island Rail Road TYPE OF INCIDENT: Evacuation SYNOPSIS: On Friday, February 2, 2007, at approximately 6:37 p.m., the LIRR movement bureau placed a block on the four main line tracks in the Valley interlocking after the Valley Tower Operator reported that an electrical power wire was hanging low across the tracks. Valley Tower is located in the town of Valley Stream and the power wire from a Long Island Power Authority (LIPA) sub-station on the north side of the right-of-way extends overhead across to the south side of tracks. The wire had sagged to approximately five feet above the Long Beach #2 track; 10 feet above the Montauk #2 track; and four feet above the top of the head car on train #4153 on Montauk #1 track were it had stopped adjacent to the Valley Tower. The wire did not come into contact with the train. The movement bureau established a block on the #1 and #2 tracks of both the Montauk and the Atlantic lines, effectively shutting down traffic through the interlocking. This affected train movement on the Montauk, Far Rockaway, West Hempstead and Long Beach Branches. A total of 14 trains (eight eastbound and six westbound) were delayed between the Hall Interlocking (west of Jamaica Station) and the Merrick Station on the Montauk Branch when third rail power was shut off. Of the above trains, 8 of them stopped within the limits of the Valley Interlocking.