[123I]FP-CIT SPECT in Atypical Degenerative Parkinsonism
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
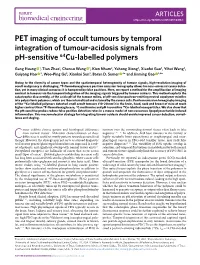
PET Imaging of Occult Tumours by Temporal Integration of Tumour-Acidosis Signals from Ph-Sensitive 64Cu-Labelled Polymers
ARTICLES https://doi.org/10.1038/s41551-019-0416-1 PET imaging of occult tumours by temporal integration of tumour-acidosis signals from pH-sensitive 64Cu-labelled polymers Gang Huang 1, Tian Zhao1, Chensu Wang 1, Kien Nham2, Yahong Xiong2, Xiaofei Gao3, Yihui Wang3, Guiyang Hao 2, Woo-Ping Ge3, Xiankai Sun2, Baran D. Sumer 4* and Jinming Gao 1,4* Owing to the diversity of cancer types and the spatiotemporal heterogeneity of tumour signals, high-resolution imaging of occult malignancy is challenging. 18F-fluorodeoxyglucose positron emission tomography allows for near-universal cancer detec- tion, yet in many clinical scenarios it is hampered by false positives. Here, we report a method for the amplification of imaging contrast in tumours via the temporal integration of the imaging signals triggered by tumour acidosis. This method exploits the catastrophic disassembly, at the acidic pH of the tumour milieu, of pH-sensitive positron-emitting neutral copolymer micelles into polycationic polymers, which are then internalized and retained by the cancer cells. Positron emission tomography imaging of the 64Cu-labelled polymers detected small occult tumours (10–20 mm3) in the brain, head, neck and breast of mice at much higher contrast than 18F-fluorodeoxyglucose, 11C-methionine and pH-insensitive 64Cu-labelled nanoparticles. We also show that the pH-sensitive probes reduce false positive detection rates in a mouse model of non-cancerous lipopolysaccharide-induced inflammation. This macromolecular strategy for integrating tumour acidosis should enable improved cancer detection, surveil- lance and staging. ancer exhibits diverse genetic and histological differences tumours over the surrounding normal tissues often leads to false from normal tissues1. -

Modafinil Tablets
PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION PrAURO-MODAFINIL Modafinil Tablets 100 mg House Standard Central Nervous System Stimulant Auro Pharma Inc. 3700 Steeles Avenue West, Suite # 402 Date of Revision: Woodbridge, ON, L4L 8K8, August 8, 2019. CANADA Submission Control Number: 230314 Page 1 of 41 Table of Contents PART I: HEALTH PROFESSIONAL INFORMATION ......................................................... 3 SUMMARY PRODUCT INFORMATION .................................................................... 3 INDICATIONS AND CLINICAL USE .......................................................................... 3 CONTRAINDICATIONS ............................................................................................... 4 WARNINGS AND PRECAUTIONS .............................................................................. 4 ADVERSE REACTIONS .............................................................................................. 12 DRUG INTERACTIONS .............................................................................................. 16 DOSAGE AND ADMINISTRATION .......................................................................... 19 OVERDOSAGE ............................................................................................................ 21 ACTION AND CLINICAL PHARMACOLOGY ........................................................ 21 STORAGE AND STABILITY ...................................................................................... 23 DOSAGE FORMS, COMPOSITION AND PACKAGING -

A Technique for Standardized Central Analysis of 6-18F-Fluoro-L-DOPA PET Data from a Multicenter Study
A Technique for Standardized Central Analysis of 6-18F-Fluoro-L-DOPA PET Data from a Multicenter Study Alan L. Whone, MRCP1; Dale L. Bailey, PhD2; Philippe Remy, PhD3; Nicola Pavese, MD1; and David J. Brooks, DSc1 1Division of Neuroscience and MRC Clinical Sciences Centre, Faculty of Medicine, Imperial College, Hammersmith Hospital, London, United Kingdom; 2Department of Nuclear Medicine, Royal North Shore Hospital, Sydney, Australia; and 3CEA-Centre National de la Recherche Scientifique Unite´ de Recherche Associe´e 2210, Service Hospitalier Frederic Joliot, Orsay, France tralized analysis offers the potential for improved detection of We have recently completed a large 6-18F-fluoro-L-DOPA (18F- outcomes due to the standardization of the analytic approach DOPA) PET study comparing rates of loss of dopamine terminal and allows the analysis of large numbers of PET studies. function in Parkinson’s disease (PD) patients taking either the Key Words: PET; 18F-DOPA; Parkinson’s disease; progression; dopamine agonist ropinirole or L-DOPA. This trial involved a central analysis “distributed acquisition/centralized analysis” method, in which J Nucl Med 2004; 45:1135–1145 18F-DOPA images were acquired at 6 different PET centers around the world and then analyzed at a single site. To our knowledge, this is the first time such a centralized approach has been employed with 18F-DOPA PET and this descriptive basic science article outlines the methods used. Methods: One hun- With rapid advances in molecular medicine, the pro- dred eighty-six PD patients were randomized (1:1) to ropinirole duction of neuroprotective or neurorestorative agents that or L-DOPA therapy, and 18F-DOPA PET was performed at base- affect the progression of degenerative conditions such as line and again at 2 y. -

Modafinil and Modafinil Analogues: Free Radical Mechanism of the Eugeroic and Cognitive Enhancment Effect Clifford Fong
Modafinil and modafinil analogues: free radical mechanism of the eugeroic and cognitive enhancment effect Clifford Fong To cite this version: Clifford Fong. Modafinil and modafinil analogues: free radical mechanism of the eugeroic and cognitive enhancment effect. [Research Report] Eigenenergy. 2018. hal-01933737 HAL Id: hal-01933737 https://hal.archives-ouvertes.fr/hal-01933737 Submitted on 24 Nov 2018 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Modafinil and modafinil analogues: free radical mechanism of the eugeroic and cognitive enhancment effect Clifford W. Fong Eigenenergy, Adelaide, South Australia. Keywords: Modafinil, modafinil-like analogues, eugeroic effect, cognitive enhancement, free radicals, quantum mechanics Abbreviations Dopamine DA, dopamine transporter DAT, Dissociative electron transfer or attachment DET, Linear free energy relationship LFER, free energy of water desolvation ΔG desolv,CDS , lipophilicity free energy ΔG lipo,CDS, cavity dispersion solvent structure of the first solvation shell CDS, highest occupied molecular orbital HOMO, lowest unoccupied molecular orbital LUMO, multiple correlation coefficient R 2, the F test of significance, standards errors for the estimate (SEE) and standard errors of the variables SE(ΔG desolCDS ), SE(ΔG lipoCDS ), SE(Dipole Moment), SE (Molecular Volume), transition state TS, reactive oxygen species ROS. -

DICOM Conformance Template
g GE Heathcare Technical Publications Direction 5507068-1EN (DOC1584283) Revision 1 DaTQUANT Application™ DICOM CONFORMANCE STATEMENT Copyright 2015 by General Electric Co. Do not duplicate g GE Heathcare LIST OF REVISIONS REV DATE DESCRIPTION PAGES APPR. 1 May 2015 Initial Release All M. Mesh DATQUANT APPLICATION GE Healthcare DICOM CONFORMANCE STATEMENT DIR 5507068-1EN (DOC1584283) REV 1 THIS PAGE LEFT INTENTIONALLY BLANK DATQUANT APPLICATION GE Healthcare DICOM CONFORMANCE STATEMENT DIR 5507068-1EN (DOC1584283) REV 1 CONFORMANCE STATEMENT OVERVIEW DaTQUANT application is an application that uses NM and CT images and creates NM, SC and MFSC images. Table 0.1 provides an overview of the network services supported by the DaTQUANT application. Table 0.1 – APPLICATION SOP Classes User of Object Creator of Instances Object Instances Transfer Secondary Capture Image Storage No Yes Multi-frame True Color Secondary Capture Image Storage No Yes Nuclear Medicine Image Storage Yes Yes Computerized Tomography Image Storage Yes No 4 DATQUANT APPLICATION GE Healthcare DICOM CONFORMANCE STATEMENT DIR 5507068-1EN (DOC1584283) REV 1 1. INTRODUCTION ............................................................................................................... 8 1.1 Overview ..................................................................................................................................................................... 8 1.2 Overall DICOM Conformance Statement Document Structure .......................................................................... -

Brain Imaging
Publications · Brochures Brain Imaging A Technologist’s Guide Produced with the kind Support of Editors Fragoso Costa, Pedro (Oldenburg) Santos, Andrea (Lisbon) Vidovič, Borut (Munich) Contributors Arbizu Lostao, Javier Pagani, Marco Barthel, Henryk Payoux, Pierre Boehm, Torsten Pepe, Giovanna Calapaquí-Terán, Adriana Peștean, Claudiu Delgado-Bolton, Roberto Sabri, Osama Garibotto, Valentina Sočan, Aljaž Grmek, Marko Sousa, Eva Hackett, Elizabeth Testanera, Giorgio Hoffmann, Karl Titus Tiepolt, Solveig Law, Ian van de Giessen, Elsmarieke Lucena, Filipa Vaz, Tânia Morbelli, Silvia Werner, Peter Contents Foreword 4 Introduction 5 Andrea Santos, Pedro Fragoso Costa Chapter 1 Anatomy, Physiology and Pathology 6 Elsmarieke van de Giessen, Silvia Morbelli and Pierre Payoux Chapter 2 Tracers for Brain Imaging 12 Aljaz Socan Chapter 3 SPECT and SPECT/CT in Oncological Brain Imaging (*) 26 Elizabeth C. Hackett Chapter 4 Imaging in Oncological Brain Diseases: PET/CT 33 EANM Giorgio Testanera and Giovanna Pepe Chapter 5 Imaging in Neurological and Vascular Brain Diseases (SPECT and SPECT/CT) 54 Filipa Lucena, Eva Sousa and Tânia F. Vaz Chapter 6 Imaging in Neurological and Vascular Brain Diseases (PET/CT) 72 Ian Law, Valentina Garibotto and Marco Pagani Chapter 7 PET/CT in Radiotherapy Planning of Brain Tumours 92 Roberto Delgado-Bolton, Adriana K. Calapaquí-Terán and Javier Arbizu Chapter 8 PET/MRI for Brain Imaging 100 Peter Werner, Torsten Boehm, Solveig Tiepolt, Henryk Barthel, Karl T. Hoffmann and Osama Sabri Chapter 9 Brain Death 110 Marko Grmek Chapter 10 Health Care in Patients with Neurological Disorders 116 Claudiu Peștean Imprint 126 n accordance with the Austrian Eco-Label for printed matters. -

Lettirs to Th Editor Radiation Injury from Interstitial Injection Of
DEPARTMENTS Lettirs to th Editor Radiation Injury from Interstitial Injection of measuring approximately 2 cm x 1 cm. Monitoring of the site Iodine-131-Iodocholesterol demonstrated retention of 131!(Fig. 2). On the basis of serial counts, the half-time was 5.5 days at the i.v. injection site. TO THE EDITOR: A 44-yr-oldman wasinvestigatedfor recur The absorbeddose deliveredto the overlyingskin cannot be rent Cushing's disease. An adrenal gland scan was initiated with precisely calculated because it has a very strong inverse depend injection of 34-MBq of ‘31I-iodocholesterol over a 5-mm interval. ence on the interstitial volume occupied by the injectate, and this Prior to injection, blood was withdrawn into the hub of the volume is not accurately known. The absorbed dose can be syringe to ensure correct i.v. placement. At the conclusion of the estimated by treating the interstitial volume occupied by the injection, the patient volunteered that the injection had been the injectate as a disk of the same area as the erythematous patch; least painful i.v. entry he had experienced. Seven days later, the thickness of this volume can be roughly estimated. The imaging failed to detect any radioactivity in the field of view volumeofdistributionwasassumedto remainconstantovertime centered on the adrenal glands. Monitoring of the injection site since the injectate is not water-soluble. The absorbed dose in this demonstrated essentially complete retention of the radiophar volume can be calculated by the method of Johns and Cun maceutical at the site. ningham (1). Because the model assumes no activity outside the The patient returned 13 days later (i.e., 20 days after the volume,the absorbeddose in the regionadjacentto this volume injection) to inquire about the tender pruritic and erythematous within the range of the beta particles (i.e., the skin) can be patch at the injection site at which time the photograph in Figure estimated to be halfthe dose inside the volume. -

Nuclear Pharmacy Quick Sample
12614-01_CH01-rev3.qxd 10/25/11 10:56 AM Page 1 CHAPTER 1 Radioisotopes Distribution for Not 1 12614-01_CH01-rev3.qxd 10/25/1110:56AMPage2 2 N TABLE 1-1 Radiopharmaceuticals Used in Nuclear Medicine UCLEAR Chemical Form and Typical Dosage P Distribution a b HARMACY Radionuclide Dosage Form Use (Adult ) Route Carbon C 11 Carbon monoxide Cardiac: Blood volume measurement 60–100 mCi Inhalation Carbon C 11 Flumazenil injection Brain: Benzodiazepine receptor imaging 20–30 mCi IV Q UICK Carbon C 11 Methionine injection Neoplastic disease evaluation in brain 10–20 mCi IV R Carbon C 11 forRaclopride injection Brain: Dopamine D2 receptor imaging 10–15 mCi IV EFERENCE Carbon C 11 Sodium acetate injection Cardiac: Marker of oxidative metabolism 12–40 mCi IV Carbon C 14 Urea Diagnosis of Helicobacter pylori infection 1 µCi PO Chromium Cr 51 Sodium chromate injection Labeling red blood cells (RBCs) for mea- 10–80 µCi IV suring RBC volume, survival, and splenic sequestration Cobalt Co 57 Cyanocobalamin capsules Diagnosis of pernicious anemia and 0.5 µCi PO Not defects of intestinal absorption Fluorine F 18 Fludeoxyglucose injection Glucose utilization in brain, cardiac, and 10–15 mCi IV neoplastic disease Fluorine F 18 Fluorodopa injection Dopamine neuronal decarboxylase activity 4–6 mCi IV in brain Fluorine F 18 Sodium fluoride injection Bone imaging 10 mCi IV Gallium Ga 67 Gallium citrate injection Hodgkin’s disease, lymphoma 8–10 mCi IV Acute inflammatory lesions 5 mCi IV Indium In 111 Capromab pendetide Metastatic imaging in patients with biopsy- -
Texas Controlled Substances Act
HEALTH AND SAFETY CODE TITLE 6. FOOD, DRUGS, ALCOHOL, AND HAZARDOUS SUBSTANCES SUBTITLE C. SUBSTANCE ABUSE REGULATION AND CRIMES CHAPTER 481. TEXAS CONTROLLED SUBSTANCES ACT SUBCHAPTER A. GENERAL PROVISIONS Sec.A481.001.AASHORT TITLE. This chapter may be cited as the Texas Controlled Substances Act. Acts 1989, 71st Leg., ch. 678, Sec. 1, eff. Sept. 1, 1989. Sec.A481.002.AADEFINITIONS. In this chapter: (1)AA"Administer" means to directly apply a controlled substance by injection, inhalation, ingestion, or other means to the body of a patient or research subject by: (A)AAa practitioner or an agent of the practitioner in the presence of the practitioner; or (B)AAthe patient or research subject at the direction and in the presence of a practitioner. (2)AA"Agent" means an authorized person who acts on behalf of or at the direction of a manufacturer, distributor, or dispenser. The term does not include a common or contract carrier, public warehouseman, or employee of a carrier or warehouseman acting in the usual and lawful course of employment. (3)AA"Commissioner" means the commissioner of state health services or the commissioner 's designee. (4)AA"Controlled premises" means: (A)AAa place where original or other records or documents required under this chapter are kept or are required to be kept; or (B)AAa place, including a factory, warehouse, other establishment, or conveyance, where a person registered under this chapter may lawfully hold, manufacture, distribute, dispense, administer, possess, or otherwise dispose of a controlled substance or other item governed by the federal Controlled Substances Act (21 U.S.C. -

Pharmacy and Poisons Act 1979
Q UO N T FA R U T A F E BERMUDA PHARMACY AND POISONS ACT 1979 1979 : 26 TABLE OF CONTENTS PART I PRELIMINARY 1 Short title 2 Interpretation PART II THE PHARMACY COUNCIL 3 The Pharmacy Council 4 Membership of the Council 4A Functions of the Council 4B Protection from personal liability 4C Annual Report 5 Proceedings of the Council, etc PART III REGISTRATION OF PHARMACISTS 6 Offence to practise pharmacy if not registered 7 Registration as a pharmacist 7A Re-registration as non-practising member 7AA Period of validity of registration 8 Code of Conduct 9 Pharmacy Profession Complaints Committee 10 Investigation of complaint by Committee 10A Inquiry into complaint by Council 10B Inquiry by Council of its own initiative 11 Surrender of registration 12 Restoration of name to register 1 PHARMACY AND POISONS ACT 1979 13 Proof of registration 14 Appeals 14A Fees 14B Amendment of Seventh Schedule 15 Regulations for this part PART IV REGISTRATION OF PHARMACIES 16 Register of pharmacies 17 Registration of premises as registered pharmacies 18 Unfit premises: new applications 19 Unfit premises: registered pharmacies 20 Appeals 21 When certificates of unfitness take effect 22 Regulations for this Part PART V CONTROL OF PRESCRIPTIONS AND IMPORTATION 23 Prescriptions to be in a certain form 23A Validity of a prescription 24 Supply by registered pharmacist of equivalent medicines 25 Restrictions on the importation of medicines 26 Declaration relating to imported medicines [repealed] PART VI CONTROL OF DRUGS 27 Certain substances to be sold on prescription -

Modafinil: a Review of Neurochemical Actions and Effects on Cognition
Neuropsychopharmacology (2008) 33, 1477–1502 & 2008 Nature Publishing Group All rights reserved 0893-133X/08 $30.00 www.neuropsychopharmacology.org Perspective Modafinil: A Review of Neurochemical Actions and Effects on Cognition ,1 1 Michael J Minzenberg* and Cameron S Carter 1Imaging Research Center, Davis School of Medicine, UC-Davis Health System, University of California, Sacramento, CA, USA Modafinil (2-[(Diphenylmethyl) sulfinyl] acetamide, Provigil) is an FDA-approved medication with wake-promoting properties. Pre-clinical studies of modafinil suggest a complex profile of neurochemical and behavioral effects, distinct from those of amphetamine. In addition, modafinil shows initial promise for a variety of off-label indications in psychiatry, including treatment-resistant depression, attention- deficit/hyperactivity disorder, and schizophrenia. Cognitive dysfunction may be a particularly important emerging treatment target for modafinil, across these and other neuropsychiatric disorders. We aimed to comprehensively review the empirical literature on neurochemical actions of modafinil, and effects on cognition in animal models, healthy adult humans, and clinical populations. We searched PubMed with the search term ‘modafinil’ and reviewed all English-language articles for neurochemical, neurophysiological, cognitive, or information-processing experimental measures. We additionally summarized the pharmacokinetic profile of modafinil and clinical efficacy in psychiatric patients. Modafinil exhibits robust effects on catecholamines, serotonin, glutamate, gamma amino-butyric acid, orexin, and histamine systems in the brain. Many of these effects may be secondary to catecholamine effects, with some selectivity for cortical over subcortical sites of action. In addition, modafinil (at well-tolerated doses) improves function in several cognitive domains, including working memory and episodic memory, and other processes dependent on prefrontal cortex and cognitive control. -

CT Myelogram Drugs to Avoid Hold for 48 Hours Before and 12 Hours After Your Myelogram UVA Neuroradiology
CT Myelogram Drugs to Avoid Hold for 48 Hours Before and 12 Hours After Your Myelogram UVA Neuroradiology Generic Name (Brand Name) Cidofovir (Vistide) Acetaminophen/butalbital (Allzital; Citalopram (Celexa) Bupap) Clomipramine (Anafranil) Acetaminophen/butalbital/caffeine Clonidine (Catapres; Kapvay) (Fioricet; Butace) Clorazepate (Tranxene-T) Acetaminophen/butalbital/caffeine/ Clozapine (Clozaril; FazaClo; Versacloz) codeine (Fioricet with codeine) Cyclizine (No Brand Name) Acetaminophen/caffeine (Excedrin) Cyclobenzaprine (Flexeril) Acetaminophen/caffeine/dihydrocodeine Desipramine (Norpramine) (Panlor; Trezix) Desvenlafaxine (Pristiq; Khedezla) Acetaminophen/tramadol (Ultracet) Dexmethylphenidate (Focalin) Aliskiren (Tekturna) Dextroamphetamine (Dexedrine; Amitriptyline (Elavil) ProCentra; Zenzedi) Amitriptyline and chlordiazepoxide Dextroamphetamine and amphetamine (Limbril) (Adderall) Amoxapine (Asendin) Diazepam (Valium; Diastat) Aripiprazole (Abilify) Diethylpropion (No Brand Name) Armodafinil (Nuvigil) Dimenhydrinate (Dramamine) Asenapine (Saphris) Donepezil (Aricept) Aspirin/caffeine (BC Powder; Goody Doripenem (Doribax) Powder) Doxapram (Dopram) Atomoxetine (Strattera) Doxepin (Silenor) Baclofen (Gablofen; Lioresal) Droperidol (No Brand Name) Benzphetamine (Didrex; Regimex) Duloxetine (Cymbalta) Benztropine (Cogentin) Entacapone (Comtan) Bismuth Ergotamine and caffeine (Cafergot; subcitrate/metronidazole/tetracycline Migergot) (Pylera) Escitalopram (Lexapro) Bismuth subsalicylate (Pepto-Bismol) Fluoxetine (Prozac; Sarafem)